3724
RF power deposition magnification in MRI of fractured passive metallic implants1Berlin Ultrahigh Field Facility (B.U.F.F.), Max-Delbrück-Center for Molecular Medicine in the Helmholtz Association, Berlin, Germany, 2Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt Universität zu Berlin, Berlin, Germany, 3MRI.TOOLS GmbH, Berlin, Germany
Synopsis
Keywords: Safety, Safety
Motivation: MRI of (biodegradable) passively conducting implants is challenged by potential elevation of RF power deposition (SAR) in the vicinity of an implant. Accidental implant fractures or fissures due to dynamic degradation of biodegradable implants alter the implants’ structure. This mechanical impact induces changes in the electromagnetic response of the system versus an intact implant.
Goal(s): Recognizing this clinical and patient safety challenge, this work first examines the SAR magnification caused by implant fracture
Approach: The efficacy of an optimized parallel excitation vectors deduced from a multi-objective genetic algorithm is demonstrated.
Results: Reduction of SAR magnification in fractured implant using the optimized excitation vector.
Impact: Amplification of RF power deposition in MRI of fractured metallic implants constitutes a patient safety hazard. This risk can be mitigated with parallel transmission using GA-driven excitation. This approach provides a viable clinical alternative for MRI monitoring of implantation sites.
Introduction
MRI of passive metallic implants is challenged by induced RF power deposition constraints[1]. Recognizing these constraints, established approaches focus on imaging regions outside of the implantation site and usually put the most weight on offsetting SAR constraints[2]. Biodegradable orthopedic implants provide improved patient comfort by making implant removal surgery obsolete[3]. This benefit is facilitated and supported by monitoring the implant/tissue interface and the close vicinity of the implant which requires careful SAR considerations. To meet this goal, we previously established an optimized excitation vector approach[4], which provides a solution for parallel transmission (pTX) that can address B1+ and SAR inhomogeneities for the intended use of small implant structures such as bone screws. However, the impact of implant fractures on RF power deposition of non-degradable[5,6] and biodegradable implants[7] has not been investigated so far. Recognizing this gap and clinical need, this work elucidates potential SAR elevation due to implant fractures. It also examines the feasibility of using an optimized excitation vector pTX tailored to reduce this SAR elevation. This study is of high relevance for clinical MRI practice due to the ever-growing population equipped with (biodegradable) implants.Material and method
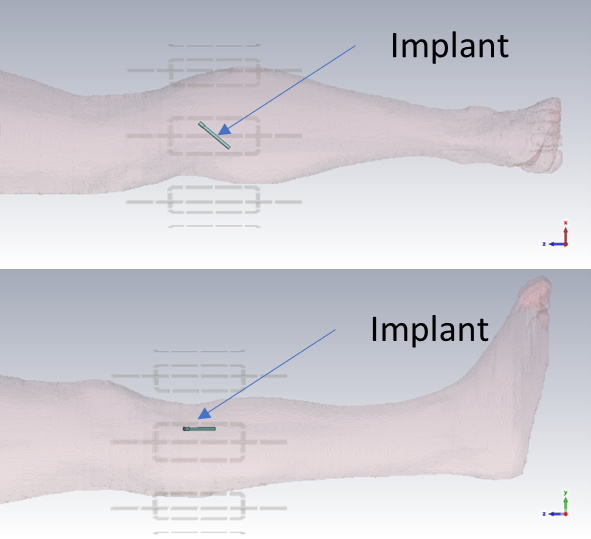
Electromagnetic simulations (f=300MHz) were performed in the CST studio suite (CST MWS, 2023) using the human voxel model Duke[8] and an eight-channel RF transceiver knee array composed of eight pairs of loops and fractionated dipoles (figure1). The output of the EMF simulations was further processed using in-house MATLAB scripts. The simulation setup consists of a cylindrical shape implant (R=2mm, L=70mm) mimicking a (bio-degradable) screw placed in the Tibia. Maximum 1g-SAR was first calculated for the non-fractured implant. To mimic an implant fracture, a 0.5mm wide fissure was implemented. The location of this fracture was moved in 5mm intervals across the implant. The RF array was driven in pTx mode by a) degenerate Birdcage (BC) mode and b) an optimized excitation vector tailored for MRI of implantation sites using a multi-objective genetic algorithm (GA)[4]Result
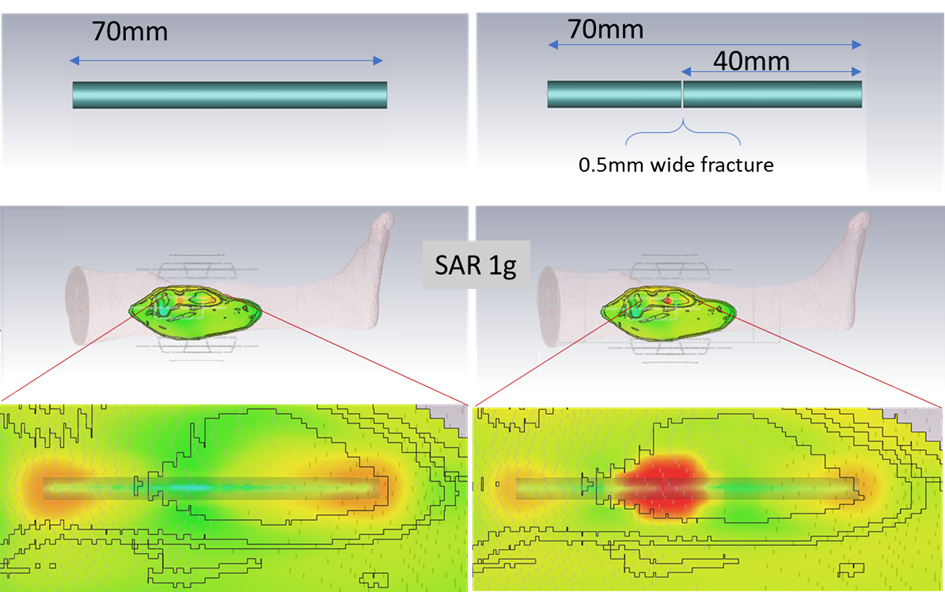
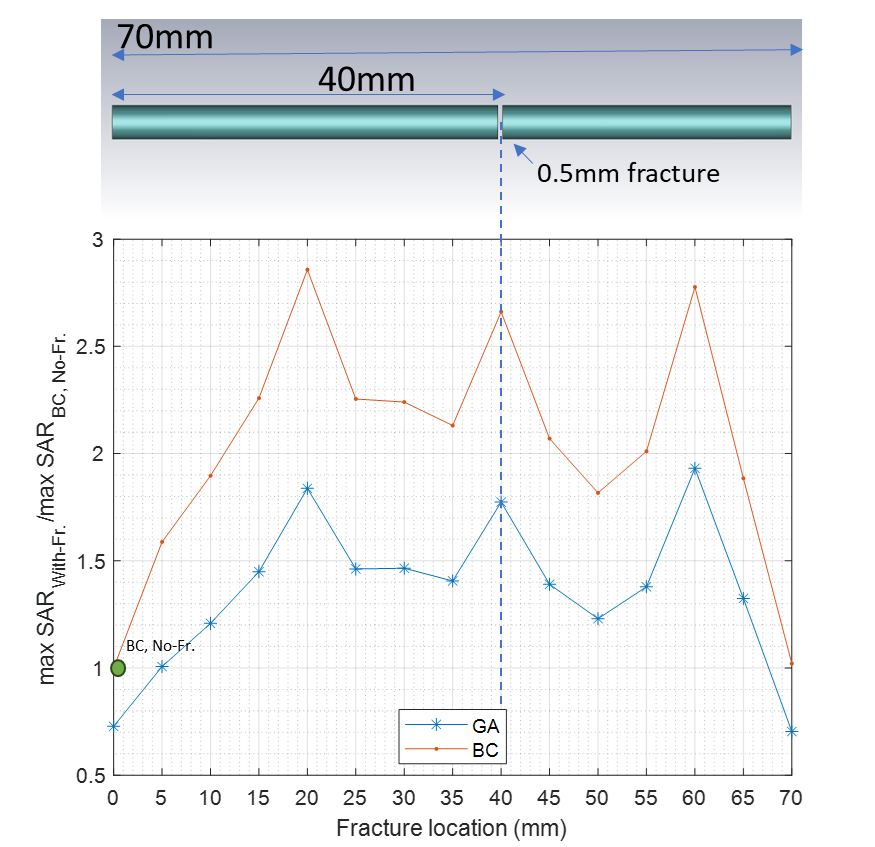
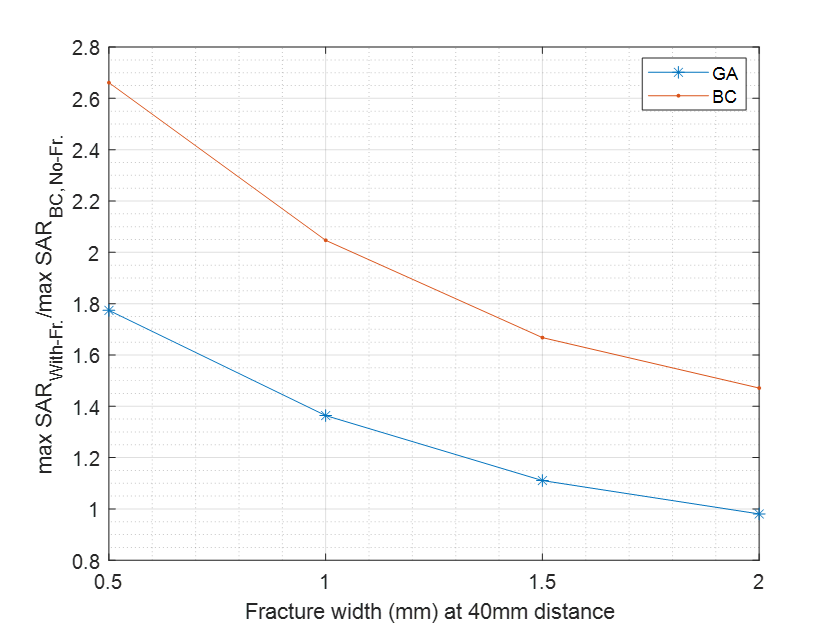
Figure2 shows 1g-SAR maps obtained from BC excitation of the non-fractured implant. It also presents the case where a 0.5mm fracture was implemented at a 40mm distance from the tip of the implant. The data highlight maximum SAR elevation around the tip of the intact implant. In the case of the fractured implant, the most pronounced SAR elevation was found at the location of the 0.5mm wide fissure. Figure3 depicts the maximum 1g-SAR obtained from a series of fractured implants normalized to 1g-SAR derived for the non-fractured implant using the BC mode (SAR BC, No-Fr.). The fractures are 0.5mm wide, and their location was moved along the long axis of the implant in 5mm increments. 1g-SAR was determined for BC- and GA-driven excitation vectors. The asymmetry seen in the normalized 1g-SAR plot is due to the non-parallel positioning of the implant with respect to the RF coil and the asymmetric nature of the voxel model. For the fractured implant configurations, our simulations revealed a 1g-SARmax amplification of up to 285% for the BC excitation. For the GA-driven excitation vector a 1g-SARmax increase of 193% with respect to SAR BC, No-Fr. was observed. Upon averaging 1g-SAR across all fracture locations an average elevation of 139% was determined for the GA-driven excitation vector. BC-driven excitations yielded an increase of 210% 1g-SARaveraged compared to SAR BC, No-Fr.Figure4 depicts 1g-SAR of the fractured implant at 40mm against different fracture widths.
Discussion and conclusion
MRI-aided monitoring of implantation sites in patients with (bio-degradable) implants presents an under-estimated and under-investigated clinical challenge. Any implant fracture alters the electromagnetic response of the implant leading to severe SAR elevation compared to the non-fractured counterpart. This RF power deposition phenomenon can be attributed to the fractioned dipole nature of the fractured implant[9] with a capacitance placed at the fractured point. The significant elevation of the E-field at the fracture point induces SAR elevation in surrounding tissues and may put patient safety at risk. Our findings demonstrate that the BC excitation yields magnification of RF power deposition in intact implants. This adverse effect is even more pronounced in the case of implant fractures. This observation compromises or even prohibits safe MRI protocol planning for implant monitoring using the BC mode. Our findings demonstrate that GA-driven excitation vectors are less susceptible to SAR amplification induced by implant fractures. This makes GA-driven pTX a viable clinical alternative for MRI monitoring of implantation sites. Notwithstanding the 71% reduction in averaged 1-gSAR elevation supported by the GA approach, further research is warranted to reduce or even eliminate 1g-SAR amplification around the fissure of a fractured implant.Acknowledgements
References
1. Winter, L., et al., MRI-Related Heating of Implants and Devices : A Review Physics of Implant Heating. 2020. p. 1-20.
2. Winter, L., et al., Parallel transmission medical implant safety testbed: Real-time mitigation of RF induced tip heating using time-domain E-field sensors. 2020.
3. Espiritu, J., M. Meier, and J.-M. Seitz, The current performance of biodegradable magnesium-based implants in magnetic resonance imaging: A review. 2021. p. 4360-4367.
4. Berangi, M., et al., MRI of Implantation Sites Using Parallel Transmission of an Optimized Radiofrequency Excitation Vector. Tomography, 2023. 9(2): p. 603-620.
5. Tallarico, M., et al., Implant Fracture: A Narrative Literature Review. Prosthesis, 2021. 3(4): p. 267-279. 6. Wu, K., B. Li, and J.J. Guo, Fatigue Crack Growth and Fracture of Internal Fixation Materials in In Vivo Environments—A Review. Materials, 2021. 14(1): p. 176.
7. Chandra, G. and A. Pandey, Biodegradable bone implants in orthopedic applications: a review. Biocybernetics and Biomedical Engineering, 2020. 40(2): p. 596-610.
8. Gosselin, M.-C., et al., Development of a new generation of high-resolution anatomical models for medical device evaluation: the Virtual Population 3.0. Physics in Medicine & Biology, 2014. 59(18): p. 5287.
9. Raaijmakers, A.J.E., et al., The fractionated dipole antenna: A new antenna for body imaging at 7 Tesla. 2016.
Figures