3719
Multi-echo phase-based quantitative T2 and T2* mapping - a feasibility study1Fetal-Neonatal Neuroimaging & Developmental Science Center, Boston Children’s Hospital, Boston, MA, United States, 2Department of Radiology, Harvard Medical School, Boston, MA, United States, 3Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Charlestown, MA, United States
Synopsis
Keywords: Quantitative Imaging, Relaxometry, Phase-Based T2 mapping, T2* (star) mapping
Motivation: To provide strategies for accurate, and high-fidelity quantitative T2 and T2* quantitative imaging.
Goal(s): To study the feasibility of simultaneous quantification of T2 and T2* using gradient-echo readouts at 3T.
Approach: We employed a multi-GRE-based acquisition with optimized TR and RF phase increments to estimate T2 and T2* maps from the acquired phase and magnitude images, respectively. We demonstrated the accuracy and feasibility of our methods, both in the ISMRM/NIST phantom and in vivo.
Results: Phase-based T2 mapping method can be combined with T2* mapping while increasing the accuracy of the T2 estimation.
Impact: This work shows that it is feasible quantify simultaneously T2 and T2* using a single multi-echo GRE acquisition.
Introduction
Over the past decade or more, many multiparametric quantitative mapping techniques have been introduced, each leveraging various advanced MRI acquisition and reconstruction methods.1–8 While most use the magnitude images of a given acquisition, recently Wang et al9 has introduced a technique that estimates T2 value from the phase images of a gradient-recalled-echo (GRE) acquisition, which has also been successfully applied to 7T imaging.10 In this work, we aim to optimize the sequence parameters, namely TR, flip angle and RF phase increment, to improve T2 estimation accuracy and enable T2* mapping, which requires a longer TR. We also aim to mitigate the effect of B1+ inhomogeneities by acquiring a B1+ map to adapt the T2 estimation to each voxel. We have tested our proposed methods both in the ISMRM/NIST and in a adult healthy volunteer, showing that high quality T2 and T2* maps at 1.1 mm3 isotropic resolution can be obtained in 14 minutes.11,12Methods
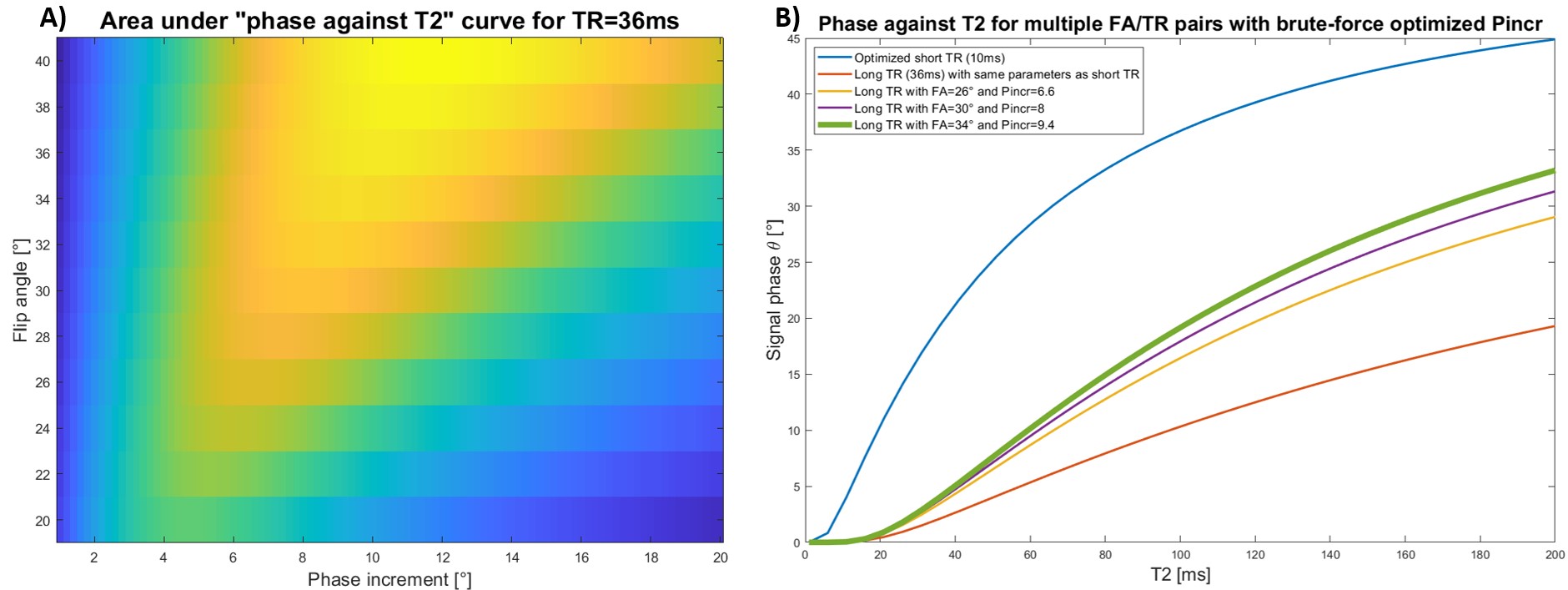
As demonstrated in 9, Bloch simulations can be used to show that phase images of GRE acquisitions obtained with a short TR (~10ms) and a small inter-repetition RF phase increment have a strong monotonic dependence on T2 relaxation. Further, to isolate T2-dependent phase from background phase, at least two datasets with opposed RF phase increments are acquired. We have repeated these Bloch simulations, but extended the “acceptable” ranges for the values of the flip angle (FA) and RF phase increments (Pincr) in order to find a combination of these parameters that allows for T2* mapping (thus increasing the TR) and to provide a more linear relationship between phase and T2 values, which would improve the accuracy of the T2 estimates. As seen in Figure 1b the most optimal FA/Pincr pair at a TR of 36ms is FA=34° and Pincr=9.4°. We limited the flip angle to 34° to mitigate SNR losses due to being further away from the Ernst angle.Data Collection
All data was acquired on a 3T Siemens Skyra scanner (Siemens Healthcare) using the 32-channel head receive array. We have coded up a custom GRE acquisition capable of employing a user-defined RF phase increment. Two different GRE acquisitions were acquired, both using FOV= 246x246mm3, matrix size=224x224, 176 slices, voxel size=1.1mm and GRAPPA acceleration factor of R=2. The first one used TR=10ms (RF increments = ±3°, TE=2.66ms, FA=15°, TA=3mins/scan). The other used TR=36ms (RF increments=±9.4°, TEs=[3.79,9.12,14.45,19.78,25.11,30.44]ms, FA=34°, TA=3mins/scan). The second acquisition used the 6 echoes to estimate a T2* map. These acquisitions were performed in the ISMRM/NIST system phantom, as well as one healthy adult volunteer. Regular GRAPPA reconstruction was performed to obtain magnitude and phase images from all the acquisitions.B1+ maps were acquired using a 2D two-shot acquisition with turbo-flash readouts using pre-saturation RF pulse preceding one of the shots. FOV’s size and orientation matched those of the GRE acquisitions; matrix size=64x64, 39 slices, voxel size=3.8x3.8x3.0mm3; TR=15s, TE=2.66ms, RGRAPPA=2, TA=32s.
Lastly, a series of single-echo spin-echo (SE-SE) acquisitions at multiple TEs were acquired in order to obtain the “ground-truth” T2 estimates. FOV’s size and orientation, as well as the matrix and voxel size were match to the GRE acquisitions. These were single slice acquisitions with TR=410ms, no acceleration and the set of TE values acquired were [25,50,100,200,400]ms, TA=6.5mins for all five acquisitions.
Results
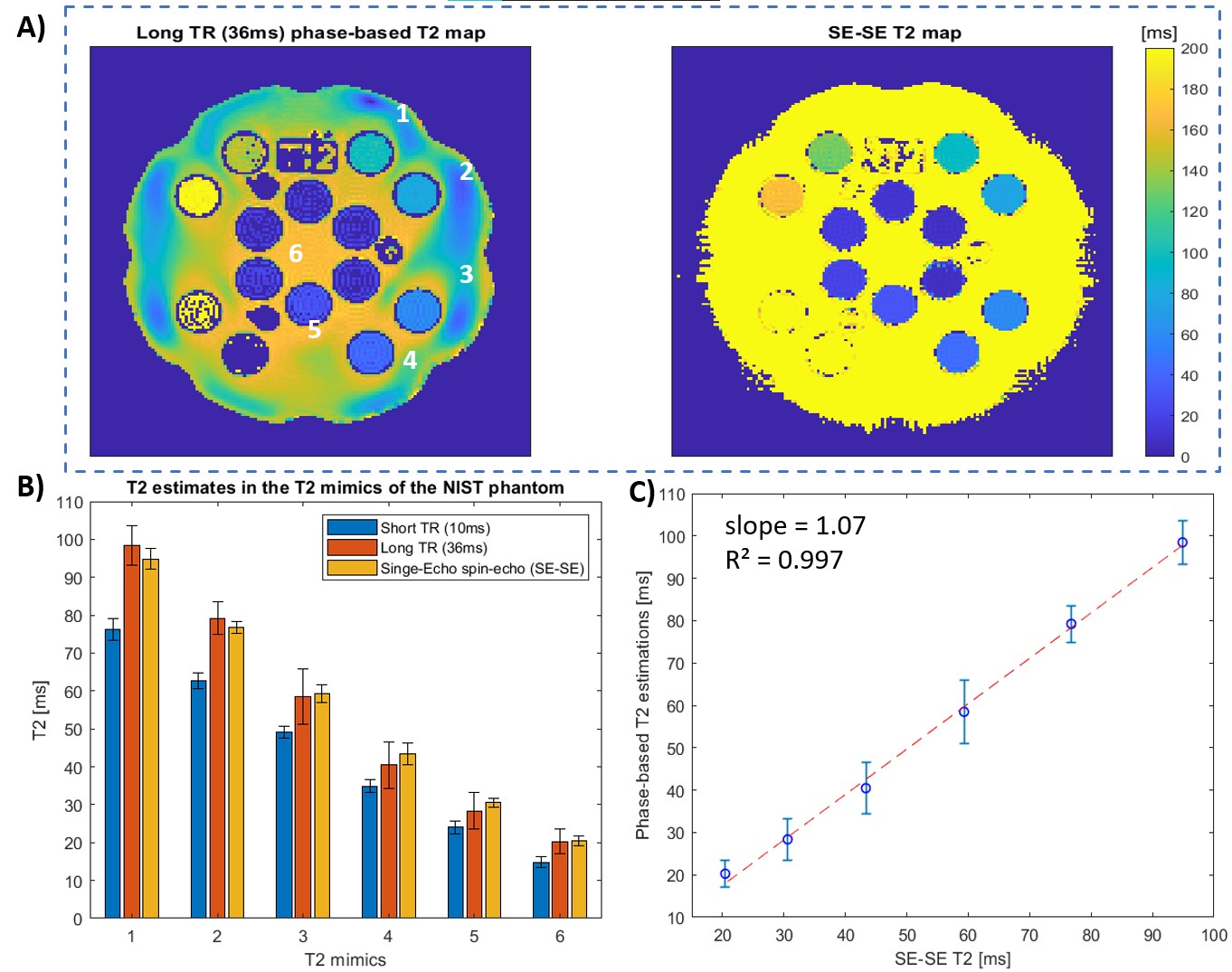
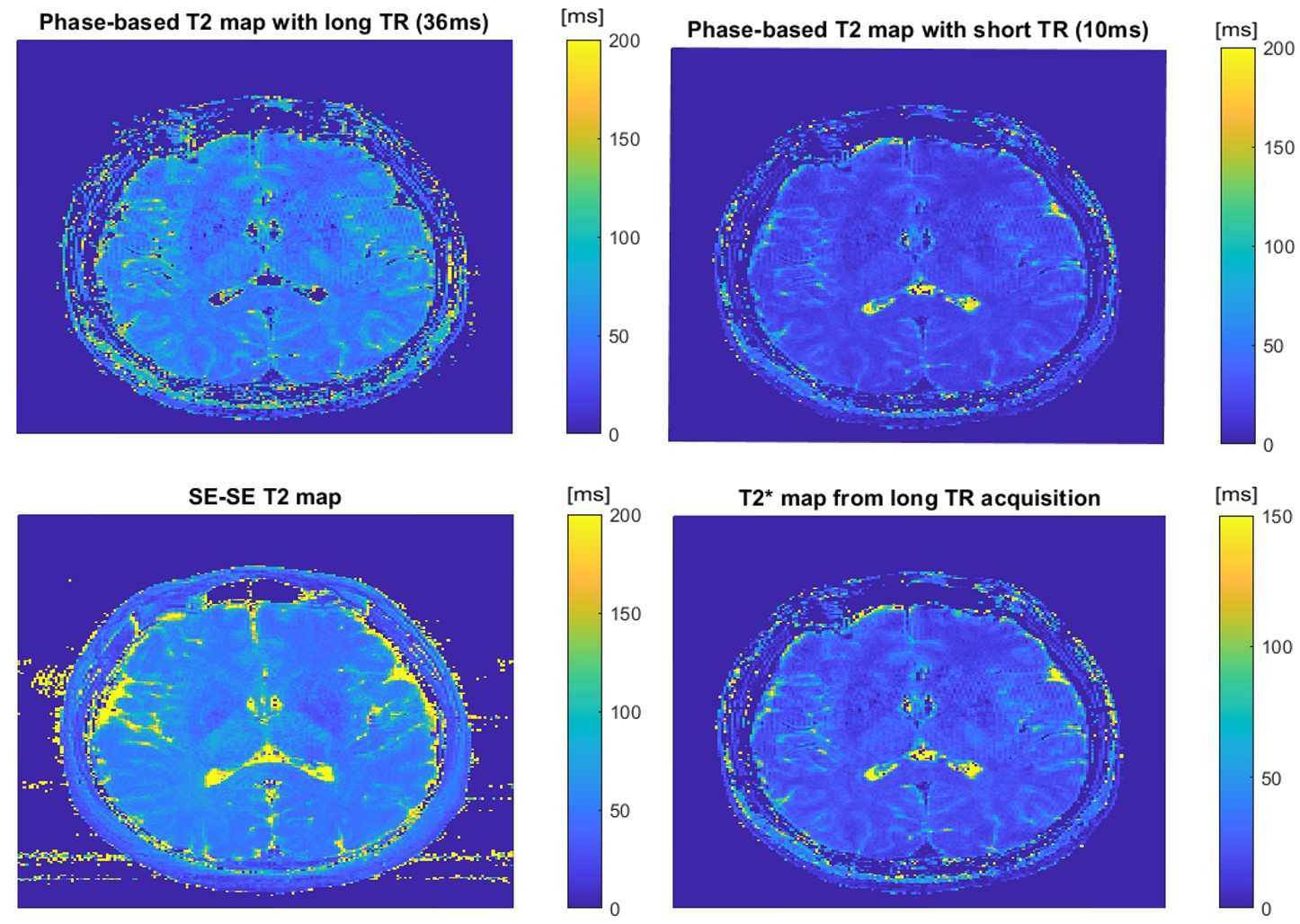
Figure 2 shows results from the estimated T2 values of the “T2 plate” of the ISMRM/NIST phantom from our two different GRE acquisitions (short TR/single TE and long TR/multiple TEs) as well as from a “ground truth” single-echo spin-echo (SE-SE) acquisitions acquired at multiple echoes. As it can be seen, the single-echo/short-TR acquisition significantly underestimates T2, (see Fig 2B) while the multi-echo/long-TR one obtains T2 values that are in much better correspondence to the ground-truth values as calculated from the SE-SE acquisitions (see Fig 2A and C).Figure 3 shows in vivo maps from two phase methods using short and long TR as well as the “ground-truth” T2 estimates, along-side the T2* maps.
Discussion and Conclusion
We demonstrated that the accuracy of the T2 estimation using phase GRE data can be improved by extending the TR and choosing the optimal FA and RF phase increments. Lengthening the TR inadvertently increases the overall scan time, but in the same time opens the possibilities to acquire multiple echoes which could be used to: 1. Estimated quantitative T2* maps that can be helpful in various clinical applications as complimentary information to the estimated T2 maps; and 2. Exploit advanced reconstruction techniques, that takes advantage of multiple sets of images from the different echoes to jointly reconstruct them at high accelerated factors11,12.Acknowledgements
No acknowledgement found.References
1. Ma D, Gulani V, Seiberlich N, et al. Magnetic resonance fingerprinting. Nature. 2013;495(7440):187-192.2. Helms G, Dathe H, Kallenberg K, Dechent P. High-resolution maps of magnetization transfer with inherent correction for RF inhomogeneity and T1 relaxation obtained from 3D FLASH MRI. Magn Reson Med. 2008;60(6):1396-1407.
3. Ma S, Nguyen CT, Han F, et al. Three-dimensional simultaneous brain T , T , and ADC mapping with MR Multitasking. Magn Reson Med. 2020;84(1):72-88.
4. Deoni SCL, Peters TM, Rutt BK. High-resolution T1 and T2 mapping of the brain in a clinically acceptable time with DESPOT1 and DESPOT2. Magn Reson Med. 2005;53(1):237-241.
5. Ehses P, Seiberlich N, Ma D, et al. IR TrueFISP with a golden-ratio-based radial readout: fast quantification of T1, T2, and proton density. Magn Reson Med. 2013;69(1):71-81.
6. Haacke EM, Chen Y, Utriainen D, et al. STrategically Acquired Gradient Echo (STAGE) imaging, part III: Technical advances and clinical applications of a rapid multi-contrast multi-parametric brain imaging method. Magn Reson Imaging. 2020;65:15-26.
7. Kvernby S, Warntjes MJB, Haraldsson H, Carlhäll CJ, Engvall J, Ebbers T. Simultaneous three-dimensional myocardial T1 and T2 mapping in one breath hold with 3D-QALAS. J Cardiovasc Magn Reson. 2014;16(1):102.
8. Cho J, Gagoski B, Kim TH, et al. Time-efficient, high-resolution 3T whole-brain relaxometry using 3D-QALAS with wave-CAIPI readouts. Magn Reson Med. September 2023. doi:10.1002/mrm.29865
9. Wang X, Hernando D, Reeder SB. Erratum to: Phase-based T mapping with gradient echo imaging (Magn Reson Med. 2020; 84:609-619). Magn Reson Med. 2022;88(2):1015.
10. Seginer A, Schmidt R. Phase-based fast 3D high-resolution quantitative T MRI in 7 T human brain imaging. Sci Rep. 2022;12(1):14088.
11. Bilgic B, Kim TH, Liao C, et al. Improving parallel imaging by jointly reconstructing multi-contrast data. Magn Reson Med. 2018;80(2):619-632.
12. Haldar JP. Low-rank modeling of local k-space neighborhoods (LORAKS) for constrained MRI. IEEE Trans Med Imaging. 2014;33(3):668-681.
Figures