3704
Evaluation of the grading efficacy of preoperative MRI for grades Ⅱ and Ⅲ intracranial solitary fibrous tumor1Magnetic Resonance Department, 1st Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 2MR Research Collaboration, Siemens Healthineers, Beijing, China
Synopsis
Keywords: Tumors (Pre-Treatment), Tumor
Motivation: Retrospective study
Goal(s): This study analyzed the general clinical features and preoperative MRI features of patients with Grade Ⅱ and Ⅲ intracranial solitary fibrous tumor (ISFT).
Approach: Intergroup comparison was conducted according to postoperative pathological grade. Binary logistic regression was performed to identify effective imaging indexes that could predict pathological grade.
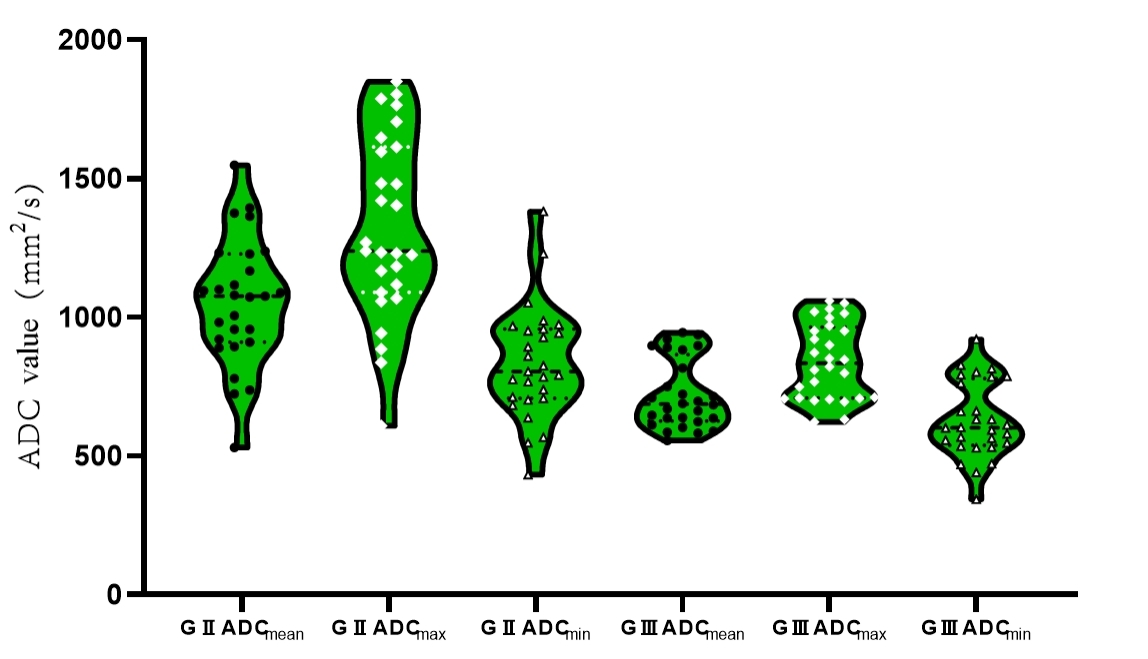
Results: There were differences between grades in tumor location; skull invasion; signal characteristics of T2-FLAIR and DWI images; and ADCmax, ADCmean and ADCmin. ADCmin was the only effective imaging index that could predict pathological grade.
Impact: Retrospective analysis showed that preoperative ADCmin can effectively predict grade Ⅱ and Ⅲ tumors in patients with ISFT, which will provide an important reference basis for preoperative grading of ISFT.
Introduction
Intracranial solitary fibrous tumor (ISFT) is a rare tumor type originating from the meningeal stroma, accounting for less than 1% of all intracranial tumors , and the main treatment method is surgical resection. There are significant differences in biological behavior and prognosis between grades Ⅱ and Ⅲ ISFT. Therefore, effective preoperative assessment of ISFT classification can provide an important theoretical basis for patients to formulate personalized treatment plans.This study retrospectively analyzed the clinical information, preoperative MRI characteristics, and intraoperative findings of 55 patients with postoperative pathology-confirmed ISFT. Preoperative MRI features were sought that could effectively predict ISFT grade, with the goal of providing a basis for clinical treatment according to imaging findings in patients with ISFT.Methods
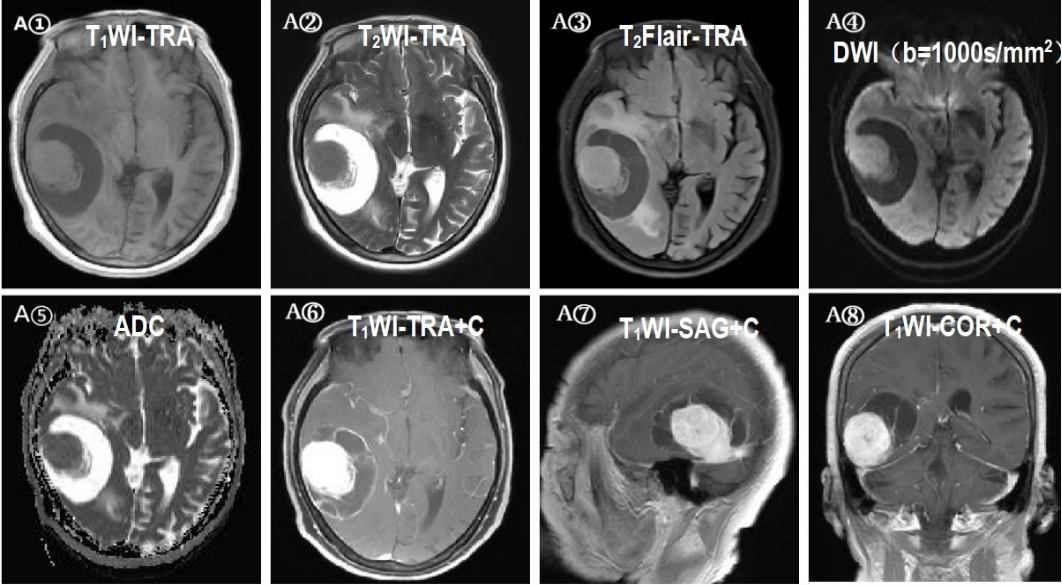
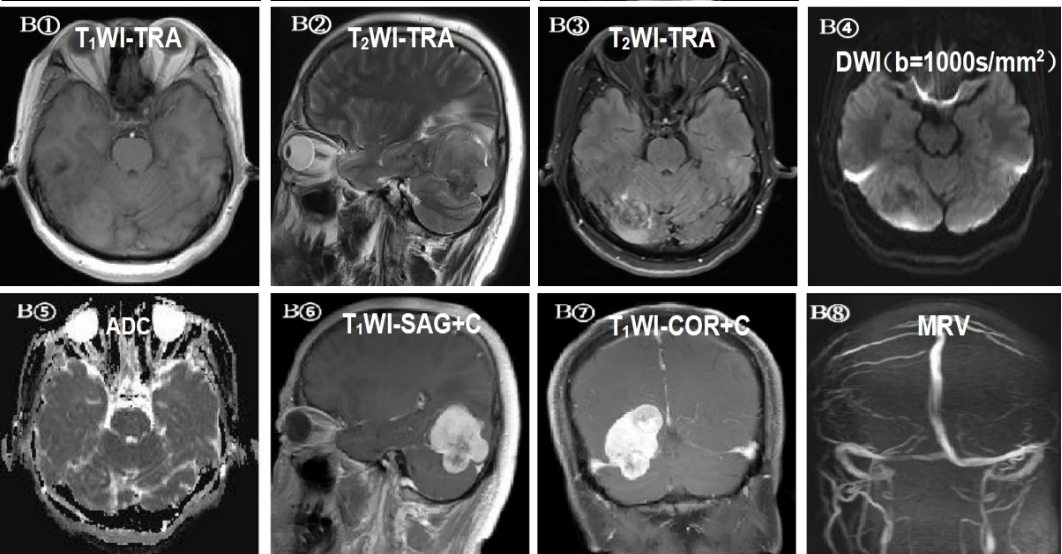
This retrospective analysis included 55 patients with ISFT who underwent surgery in our hospital from June 2012 to December 2022 and had pathologically confirmed WHO CNS 5th Grade Ⅱ or Grade Ⅲ. All patients underwent preoperative superconducting MRI on a 3T MR scanner (MAGNETOM Skyra, Verio, Prisma, Siemens Healthcare, Erlangen, Germany). The scanning sequence and parameters were as follows: 1) transverse and sagittal T1-weighted imaging (T1WI): slice thickness (ST)= 5 mm, echo time (TE) = 2.5 ms; 2) transverse T2-weighted imaging (T2WI): ST = 5 mm, TE = 2.5 ms; 3) transverse T2-fluid-attenuated inversion recovery (FLAIR): ST = 5 mm, repetition time (TR) = 6500 ms, TE = 85 ms; 4) transverse diffusion-weighted imaging (DWI): ST = 5 mm; TR = 4600 ms, TE = 80 ms, b=0, 1000 s/mm2, and ADC map automatically reconstructed after scanning; and 5) conventional dynamic enhanced (DCE)-MRI: ST= 5 mm, TE = 2.5 ms. Gadolinium meglumine (Gd-DTPA, Guangzhou Kangchen Pharmaceutical Co., China) was intravenously injected with a dose of 0.1 mmol/kg and flow rate of 2 ml/s. All imaging data were independently evaluated by two associate chief radiologists with >8 years of experience using the picture archiving and communication system (PACS). The following parameters were evaluated: T1WI , T2WI , T2-FLAIR and DWI (b=1000 s/mm2) signal characteristics, tumor location and distribution, cross-midline status, peritumoral edema, intralesional hemorrhage, focus necrosis/cystic degeneration, tumor empty vessel , tumor maximum diameter (mm), enhancement mode, and meningeal tail. The maximum apparent diffusion coefficient (ADCmax), average ADC (ADCmean), and minimum ADC (ADCmin) were calculated. The independent samples t-test or Mann-Whitney U test was used to compare continuous data between the two groups; the Pearson Chi-square test or Fisher’s exact test was used to compare categorical data between the groups. Bivariate logistic regression was performed to construct a comprehensive model; receiver operating characteristic (ROC) curves were generated and areas under the curve (AUCs) were calculated to determine the value of each parameter in the differential diagnosis of grades Ⅱ and Ⅲ ISFT.Results
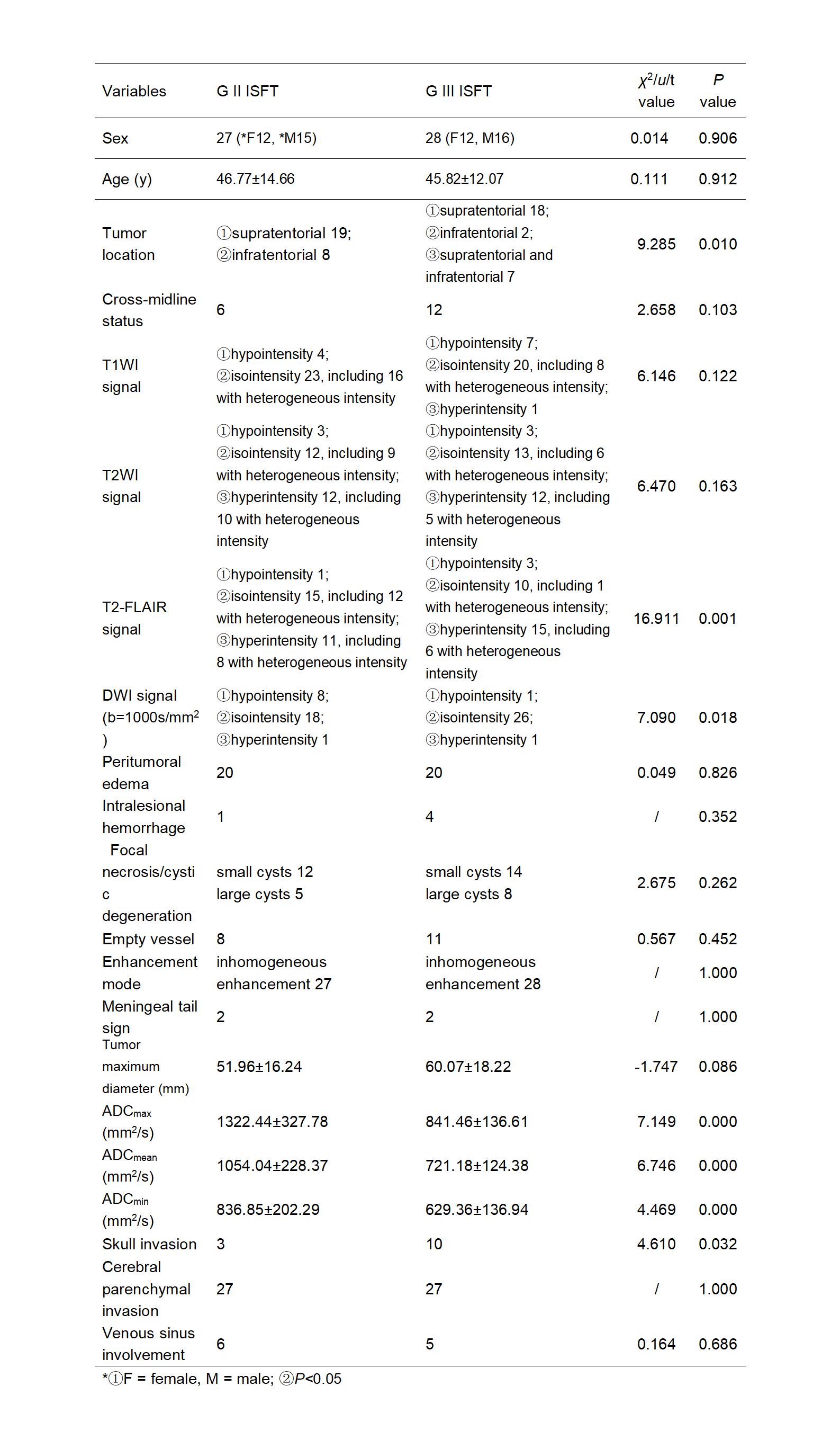
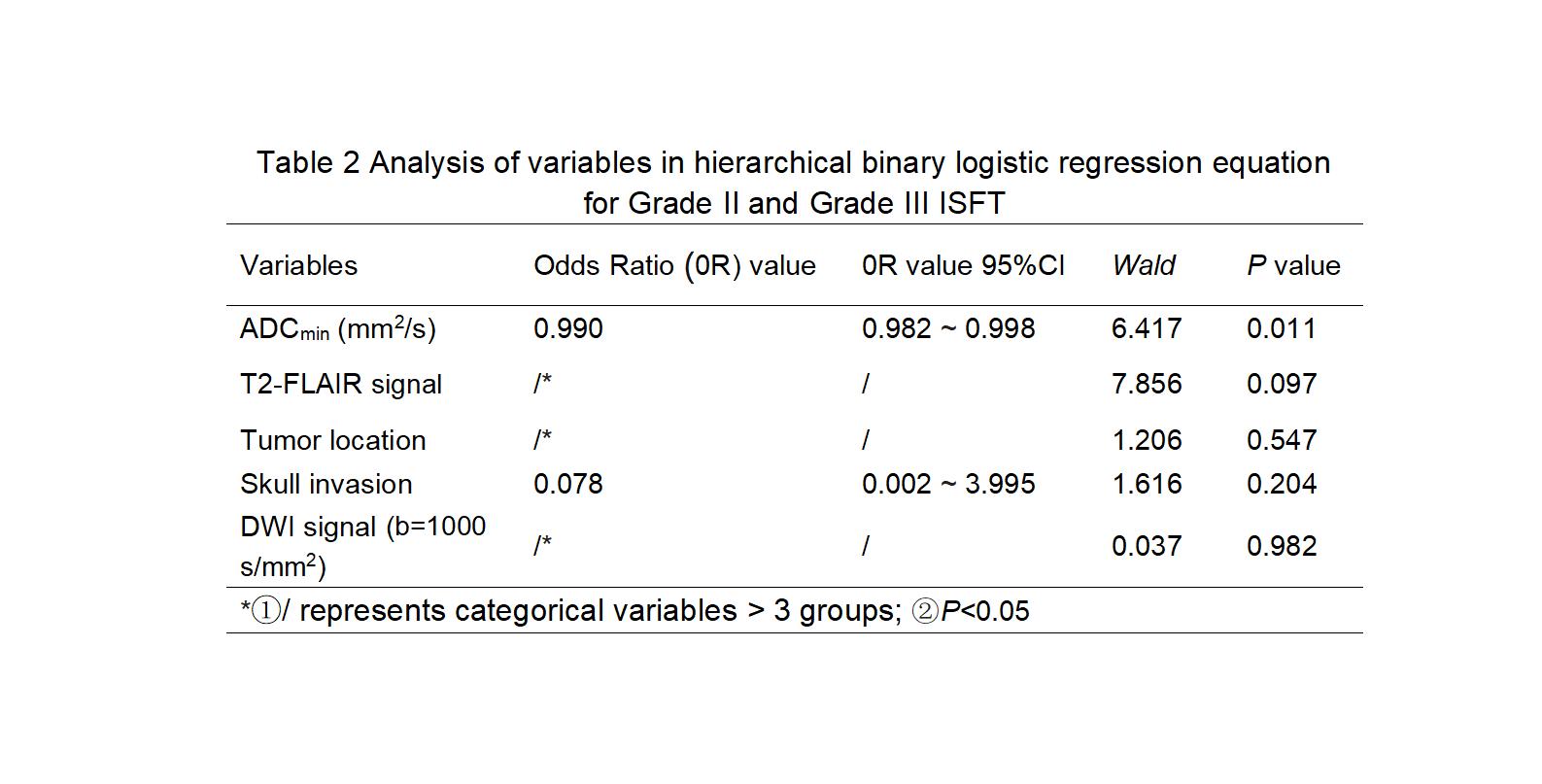
The mean age at onset was similar between patients with grades Ⅱ and Ⅲ ISFT (46.77±14.66 years and 45.82±12.07 years, respectively). The proportions of men among patients with grades Ⅱ and Ⅲ ISFT were slightly higher than the proportions of female patients (male/female: 1.25 [15/12] and 1.33 [16/12], respectively).There were significant differences between grades Ⅱ and Ⅲ ISFT in T2-FLAIR signal, DWI signal, ADCmax, ADCmin, ADCmean, tumor location, and skull invasion (P=0.001, P=0.018, P=0.000, P=0.000, P=0.000, P=0.010, and P=0.032, respectively) (Fig 1, Table 1). There were no significant differences in age, sex, cross-midline status, T1WI signal, T2WI signal, peritumoral edema, intralesional hemorrhage, focal necrosis/cystic degeneration, tumor empty vessel shadow, enhancement mode, meningeal tail sign, maximum tumor diameter, brain parenchyma invasion, or venous sinus involvement between grades Ⅱ and Ⅲ ISFT (all P>0.05) (Fig 2, Fig 3). Binary logistic regression analysis showed that when ADCmin was included in the regression equation, the model accuracy was 89.1% (Table 2). ROC curve analysis showed that the AUC of ADCmin was 0.805 (0.688, 0.922), with 74.1% sensitivity and 75.0% specificity. The ADCmin cutoff value was 672 mm2/s.Discussion and Conclusion
In this study, ADCmax, ADCmean and ADCmin were lower in patients with grade Ⅲ ISFT than in patients with grade Ⅱ ISFT. The proportion of tumor spans supratentorial and infratentorial, and the rate of skull invasion were higher in patients with grade Ⅲ ISFT than in patients with grade Ⅱ ISFT. The study found that there was a close relationship between tumor tissue and brain tissue and adhesion between leptomeninges or brain tissue in almost all patients with ISFT. These findings have not been reported in previous studies. However, ADCmin was the only effective imaging index in preoperative grading of grades Ⅱ and Ⅲ ISFT; it will help to improve the imaging-based grading of ISFT.Acknowledgements
Thanks to Chen Rui , Liu Chenchen ,Wang Wei Jian , Bai Jie ,Ma Xiaoyue for their contribution and support to this research.References
1.Louis DN, Perry A, Wesseling P, et al. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol. 2021 Aug 2;23(8):1231-1251. doi: 10.1093/neuonc/noab106. PMID: 34185076; PMCID: PMC8328013.2.Giordan E, Marton E, Wennberg AM,et al. A review of solitary fibrous tumor/hemangiopericytoma tumor and a comparison of risk factors for recurrence, metastases, and death among patients with spinal and intracranial tumors. Neurosurg Rev. 2021 Jun;44(3):1299-1312. doi: 10.1007/s10143-020-01335-x. Epub 2020 Jun 18. PMID: 32556679. 3.Sung KS, Moon JH, Kim EHet al. Solitary fibrous tumor/hemangiopericytoma: treatment results based on the 2016 WHO classification. J Neurosurg. 2018 Mar 1:1-8. doi: 10.3171/2017.9.JNS171057. Epub ahead of print. PMID: 29521591.4.Shin DW, Kim JH, Chong S, et al. Intracranial solitary fibrous tumor/hemangiopericytoma: tumor reclassification and assessment of treatment outcome via the 2016 WHO classification. J Neurooncol. 2021 Sep;154(2):171-178. doi: 10.1007/s11060-021-03733-7. Epub 2021 Aug 20. PMID: 34417710.5.Ronchi A, Cozzolino I, Zito Marino F, et al. Extrapleural solitary fibrous tumor: A distinct entity from pleural solitary fibrous tumor. An update on clinical, molecular and diagnostic features. Ann Diagn Pathol. 2018 Jun;34:142-150. doi: 10.1016/j.anndiagpath.2018.01.004. Epub 2018 Apr 9. PMID: 29660566.6.Ratneswaren T, Hogg FRA, Gallagher MJ, et al. Surveillance for metastatic hemangiopericytoma-solitary fibrous tumors-systematic literature review on incidence, predictors and diagnosis of extra-cranial disease. J Neurooncol. 2018 Jul;138(3):447-467. doi: 10.1007/s11060-018-2836-2. Epub 2018 Mar 17. PMID: 29551003.7.Thway K, Ng W, Noujaim J,et.al. The Current Status of Solitary Fibrous Tumor: Diagnostic Features, Variants, and Genetics. Int J Surg Pathol. 2016 Jun;24(4):281-92. doi: 10.1177/1066896915627485. Epub 2016 Jan 25. PMID: 26811389.8.Ge W, Yu DC, Chen G, et al. Clinical analysis of 47 cases of solitary fibrous tumor. Oncol Lett. 2016 Oct;12(4):2475-2480. doi: 10.3892/ol.2016.4967. Epub 2016 Aug 8. PMID: 27698815; PMCID: PMC5038456.9.Li X, Tan L, Ouyang X, Jiang J,et al . Magnetic resonance features of meningeal solitary fibrous tumors. Oncol Lett. 2018 Jun;15(6):8825-8832. doi: 10.3892/ol.2018.8426. Epub 2018 Apr 4. PMID: 29805622; PMCID: PMC5950533.10.Tariq MU, Din NU, Abdul-Ghafar J,et al . The many faces of solitary fibrous tumor; diversity of histological features, differential diagnosis and role of molecular studies and surrogate markers in avoiding misdiagnosis and predicting the behavior. Diagn Pathol. 2021 Apr 20;16(1):32. doi: 10.1186/s13000-021-01095-2. PMID: 33879215; PMCID: PMC8059036.11.Liu Y, Tao X, Shi H, et al. MRI findings of solitary fibrous tumours in the head and neck region. Dentomaxillofac Radiol. 2014;43(3):20130415. doi: 10.1259/dmfr.20130415. Epub 2014 Feb 3. PMID: 24720608; PMCID: PMC4064629.12.Zhou JL, Liu JL, Zhang J, et al. Thirty-nine cases of intracranial hemangiopericytoma and anaplastic hemangiopericytoma: a retrospective review of MRI features and pathological findings. Eur J Radiol. 2012 Nov;81(11):3504-10. doi: 10.1016/j.ejrad.2012.04.034. Epub 2012 May 31. PMID: 22658867.13.Chen Z, Ma L, Lou X, et al. Diagnostic value of minimum apparent diffusion coefficient values in prediction of neuroepithelial tumor grading. J Magn Reson Imaging. 2010 Jun;31(6):1331-8. doi: 10.1002/jmri.22175. PMID: 20512884.14.Higano S, Yun X, Kumabe T, et al. Malignant astrocytic tumors: clinical importance of apparent diffusion coefficient in prediction of grade and prognosis. Radiology. 2006 Dec;241(3):839-46. doi: 10.1148/radiol.2413051276. Epub 2006 Oct 10. PMID: 17032910.Figures