3697
Clinical Validation of Deep Learning-Accelerated vs. Wave-CAIPI Post-Contrast 3D-T1 MPRAGE for Evaluation of Intracranial Enhancing Lesions1Radiology, Massachusetts General Hospital, Boston, MA, United States, 2Massachusetts General Hospital, Boston, MA, United States, 3Siemens Healthcare GmbH, Erlangen, Germany, Erlangen, Germany, 4Siemens Medical Solutions USA, Boston, MA., Boston, MA, United States, 5Siemens Medical Solutions USA, Boston, MA, Boston, MA, United States
Synopsis
Keywords: Tumors (Pre-Treatment), Neuro, MR value, AI & Machine Learning
Motivation: Deep learning (DL)-enabled reconstruction has emerged as a promising approach to accelerate MRI exams; however, the performance of DL-accelerated 3D sequences for the detection of intracranial enhancing lesions has not been clinically investigated.
Goal(s): To evaluate post-contrast DL-accelerated 3D-T1-MPRAGE compared to state-of-the-art Wave-CAIPI accelerated 3D T1-MPRAGE for evaluation of intracranial enhancing lesions.
Approach: Two neuroradiologists performed head-to-head evaluation of 115 cases of post-contrast DL- vs. Wave-CAIPI-MPRAGE for visualization of dural, parenchymal, leptomeningeal, and ependymal enhancement; sharpness; noise; artifacts; and overall diagnostic quality.
Results: Highly accelerated post-contrast DL-T1-MPRAGE achieved noninferior image quality to the standard clinically validated Wave-CAIPI accelerated sequence.
Impact: Deep-learning-accelerated post-contrast 3D T1-MPRAGE demonstrates robust diagnostic quality in visualizing enhancing intracranial pathology in all compartments while maintaining similar perception of noise and artifact. DL offers a powerful approach to accelerating post-contrast 3D T1-MPRAGE for clinical and research studies.
Body of the Abstract
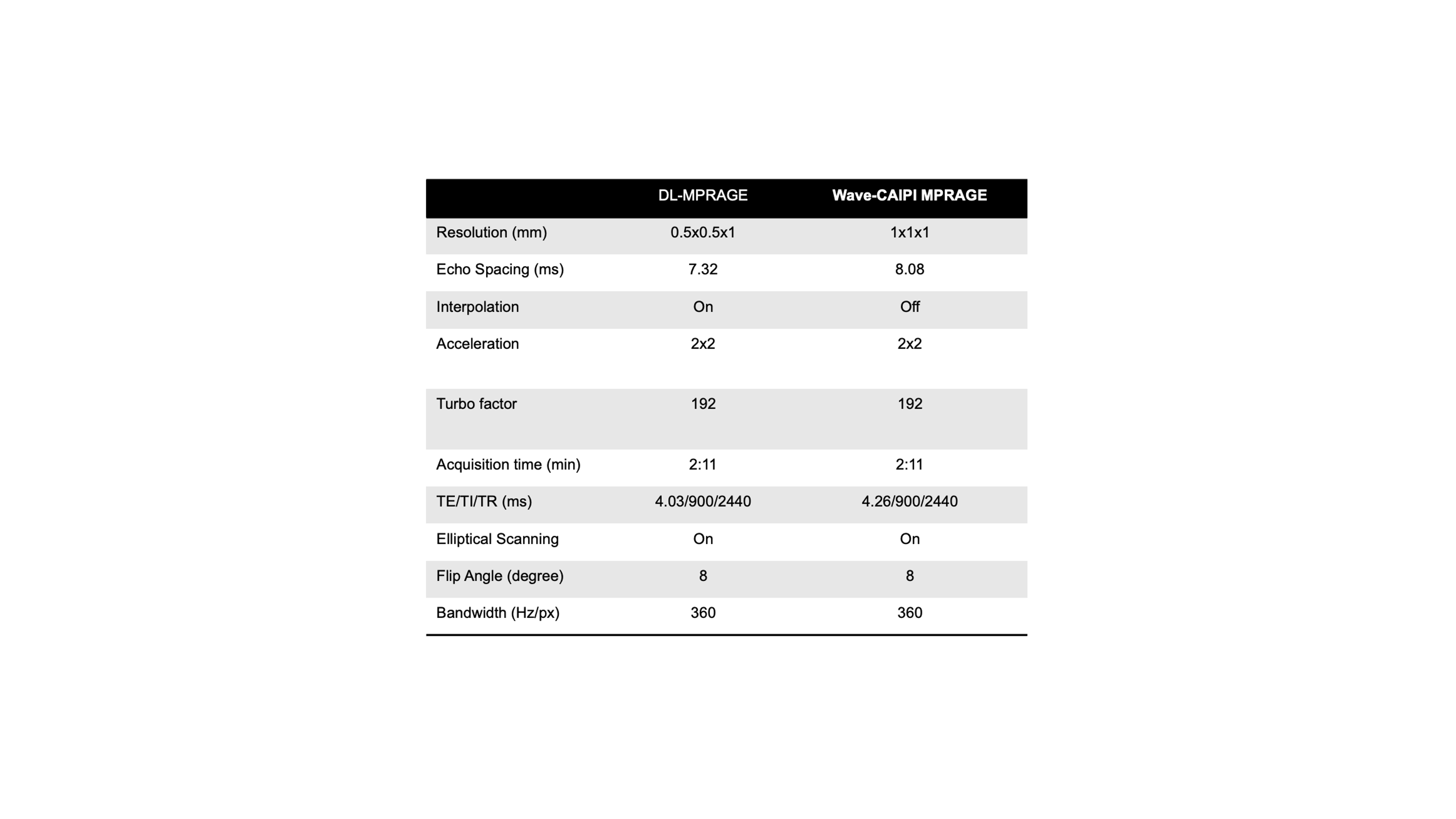
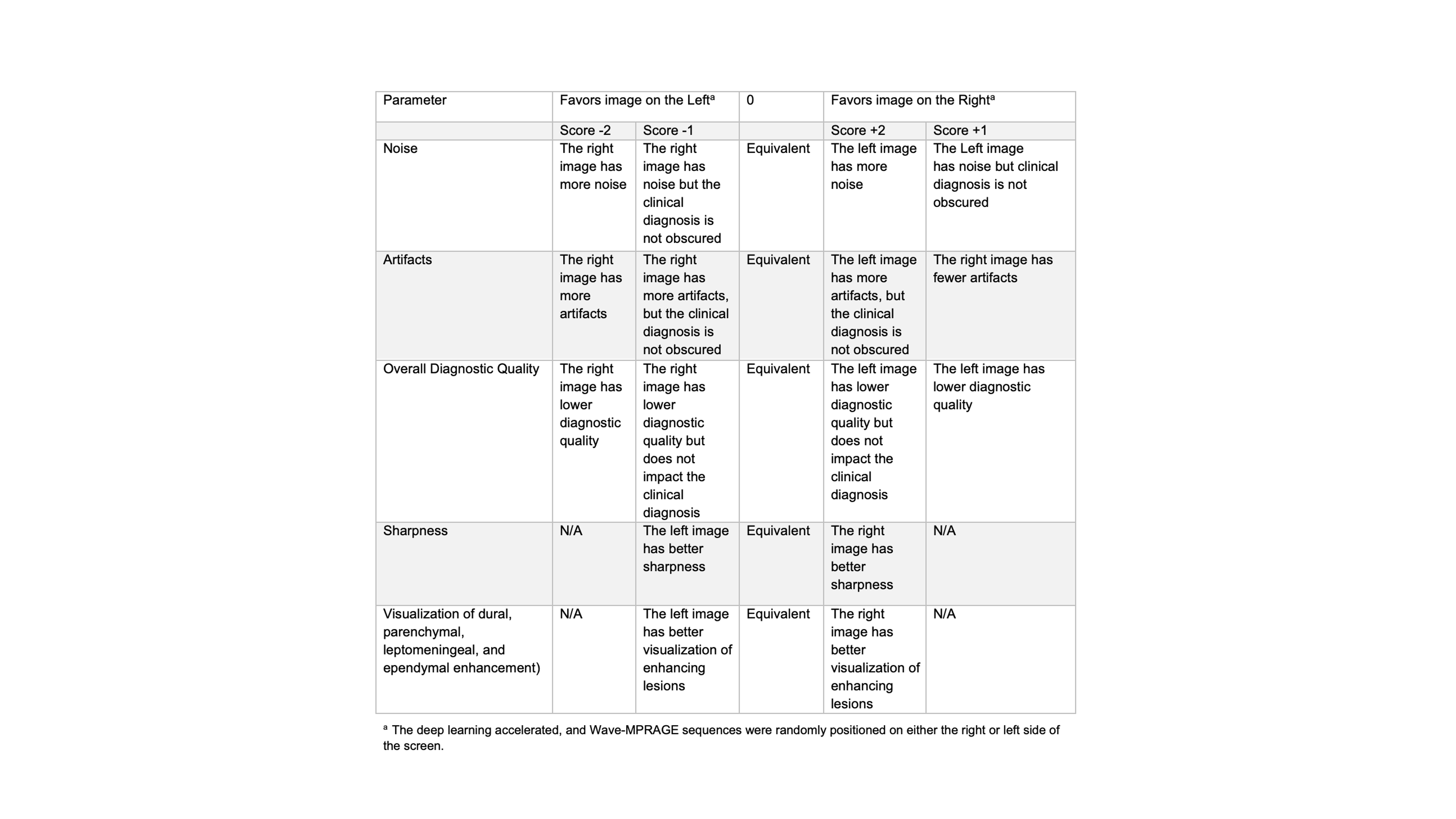
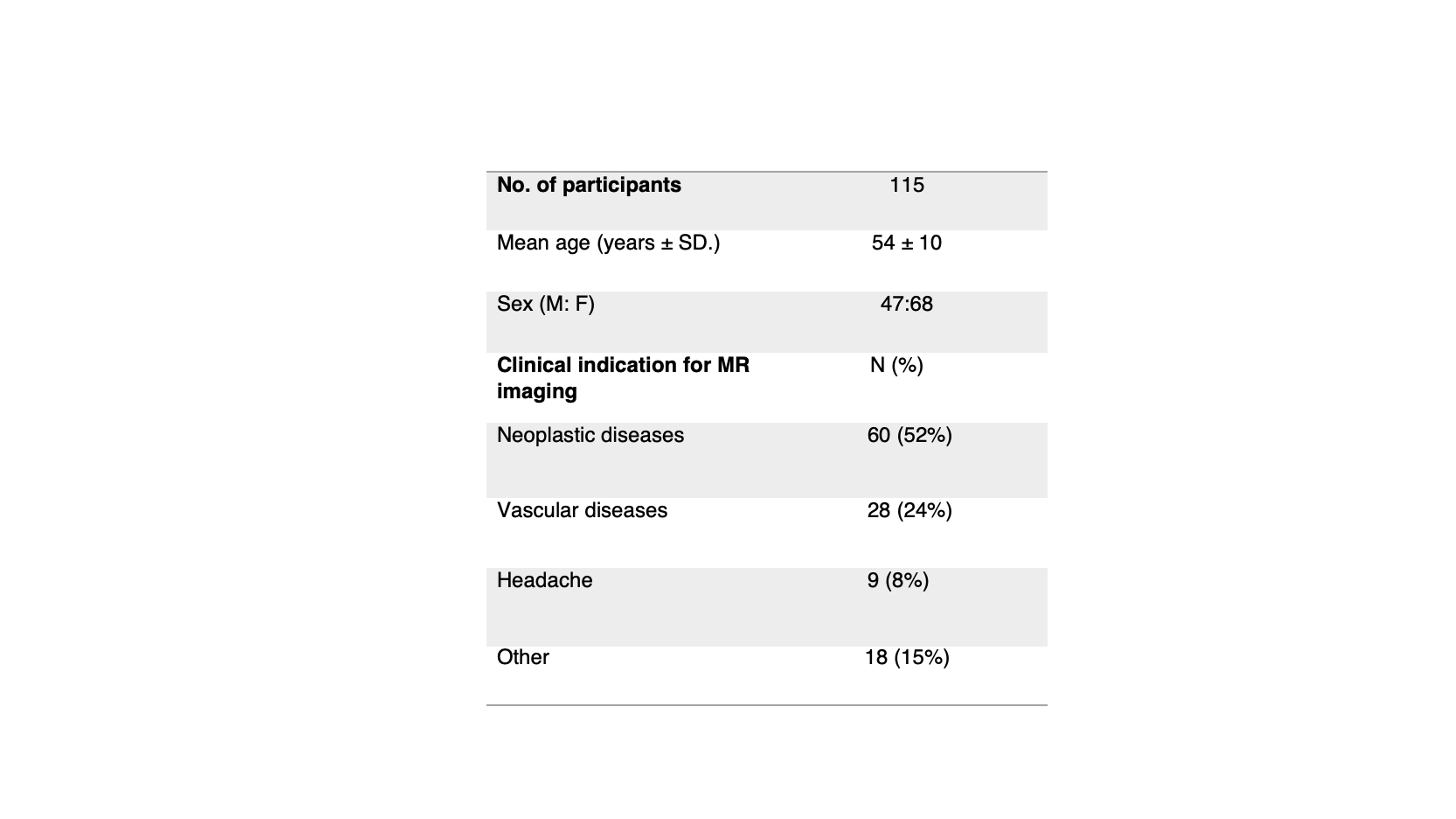
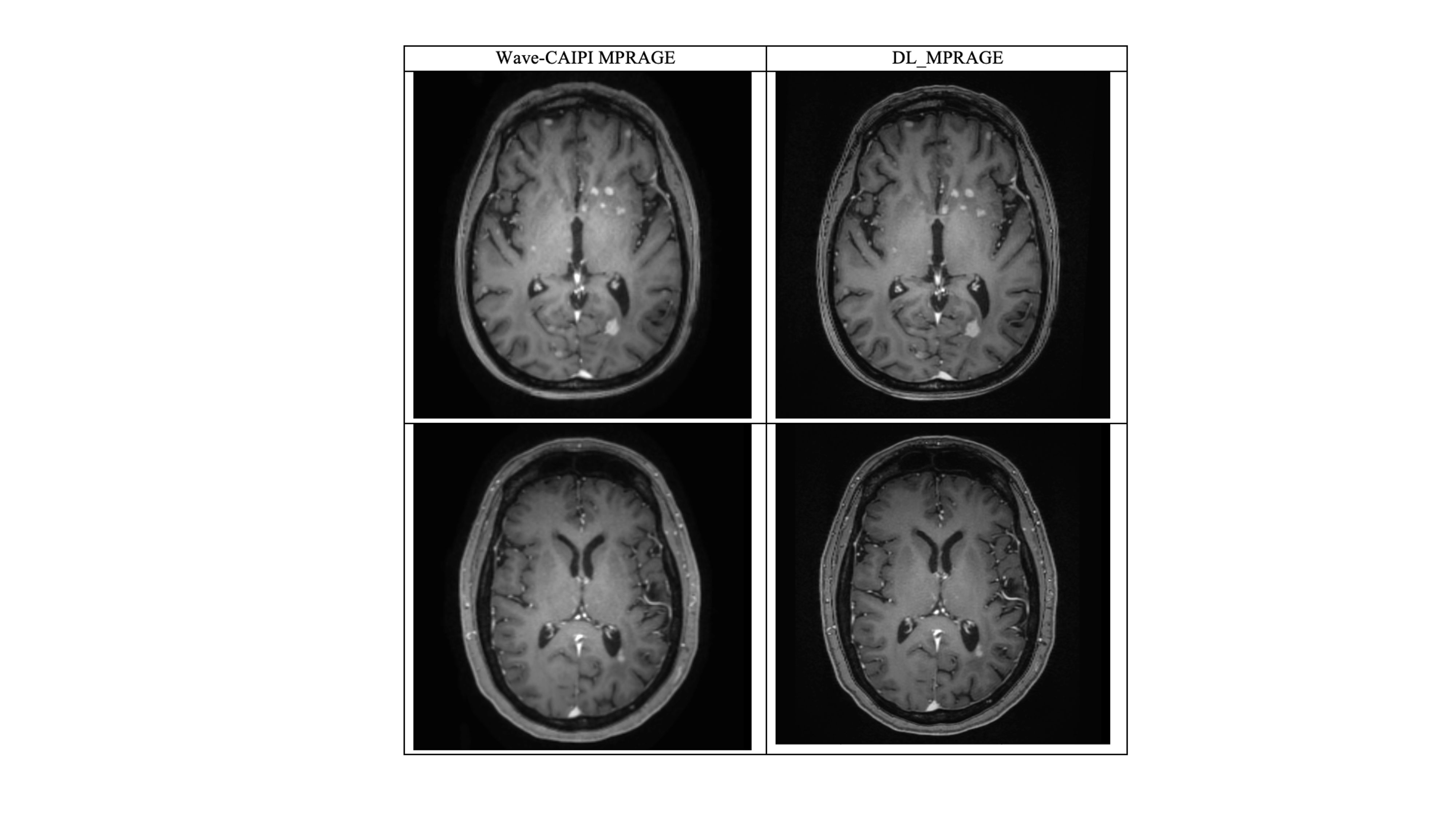
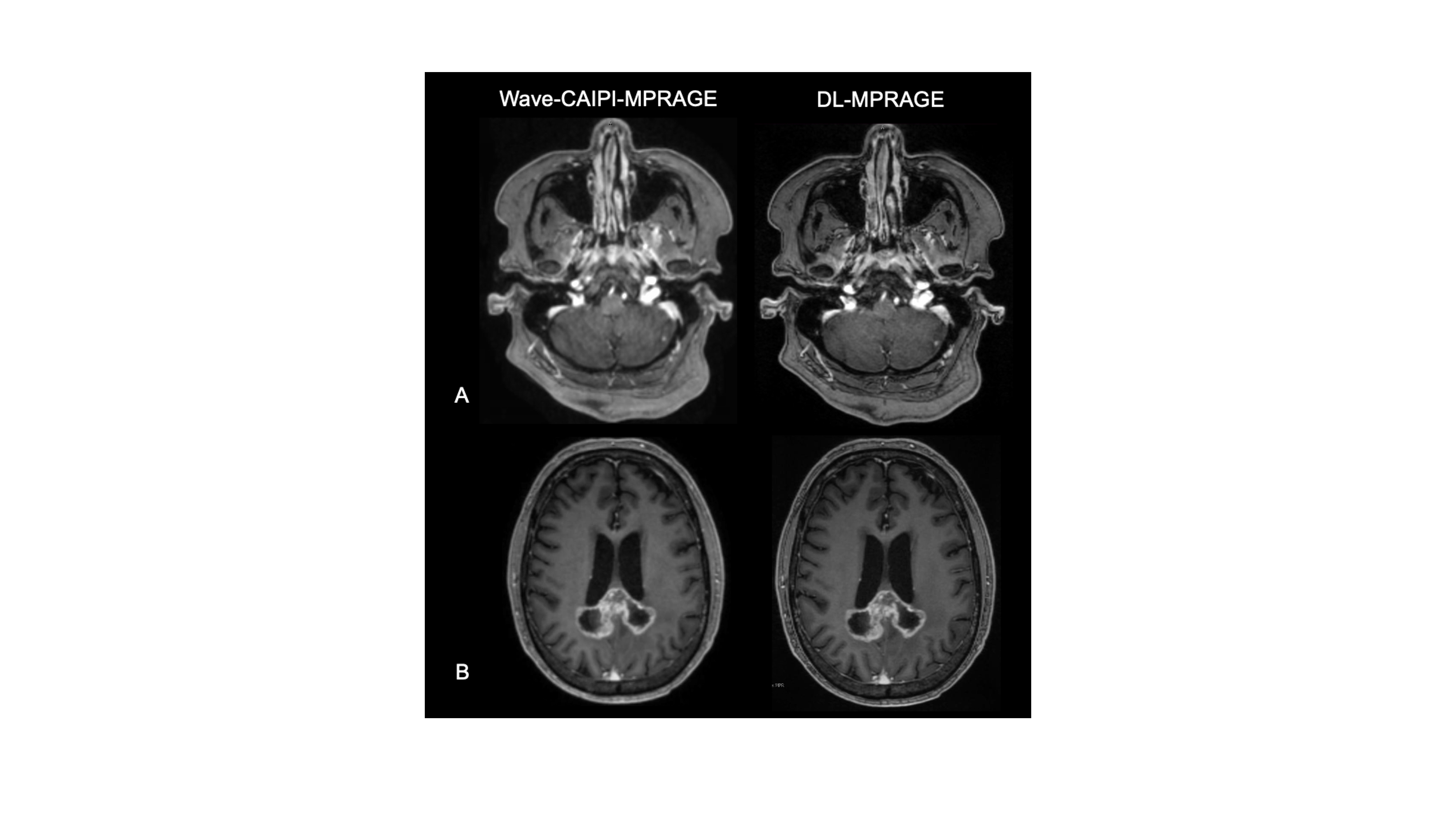
Introduction: Contrast-enhanced 3D T1-weighted magnetization prepared rapid gradient echo (MPRAGE) is the most commonly used and recommended sequence for 3D evaluation of brain tumor burden [1]. However, the standard MPRAGE sequence is lengthy (5 minutes or longer) and prone to motion artifact. Deep learning (DL) methods have begun to be applied for denoising and interpolation of data during image reconstruction, enhancing image quality and accelerating MRI scan times. When combined with k-space undersampling, these techniques have demonstrated non-inferiority in several studies [2, 3]. In this study, we assessed a novel DL-accelerated T1-weighted MPRAGE (DL-MPRAGE) sequence for detection of intracranial enhancing brain lesions relative to a state-of-the-art physics-based accelerated Wave-CAIPI MPRAGE sequence. Contrast-enhanced Wave-CAIPI 3D T1-MPRAGE was recently shown to be noninferior to a standard 3D T1-MPRAGE sequence for the visualization and diagnosis of enhancing brain lesions [4]. Methods: This prospective study was IRB approved and HIPAA compliant. During October 2023, 115 consecutive adult patients undergoing brain MRI with and without contrast on 3T MRI scanners (MAGNETOM Vida, Siemens Healthcare) were recruited in an outpatient setting. The scan protocol included a Wave-CAIPI post-contrast T1-MPRAGE (acquisition time [TA]=2:11 min) [4] and a research application post-contrast DL-T1-MPRAGE (TA=2:11 min). A two-step deep learning-based reconstruction process was employed. The first step, inspired by variational networks [10], involved six iterations alternating between data consistency updates and neural network evaluation. The second step incorporated a super-resolution algorithm for additional enhancement [4, 11]. Wave- and DL-MPRAGE sequences were obtained using comparable parameters (Fig. 1), including R = 2x2 acceleration, flip angle of 8 degrees, and TR/TE/TI of 2440/4.03/900 for DL- and 2440/4.26/900 for Wave-MPRAGE. Two independent neuroradiologists (11 and 5 years of experience) performed head-to-head evaluation of both sequences using a published 5-point scale (Fig. 2) [4] in the following categories: visualization of dural, parenchymal, leptomeningeal, and ependymal enhancement; sharpness; noise; artifacts; and overall diagnostic quality. A third board-certified neuroradiologist (12 years of experience) adjudicated cases with discrepant ratings. A 15% noninferiority margin was used to test whether post-contrast DL-T1-MPRAGE was noninferior to Wave-CAIPI T1-MPRAGE. Results and Discussion: 115 patients (68F/47M, mean age: 54±10 years) were recruited. The most common clinical indication for MRI examination was the study of neoplastic disease in 52% (60 of 115) of study participants, followed by vascular diseases in 24% (28 of 115), and headache in 8% (9 in 115) of participants (Fig. 3). In the head-to-head analysis, abnormal enhancement was detected in 60 of 115 cases (52%). Of the 60 cases that showed abnormal enhancement, 36 (60%) had parenchymal enhancement, 45 (75%) had dural enhancement, 7 (11.6%) had leptomeningeal enhancement, and 6 (10%) had ependymal enhancement. In 37 of 60 (61.6%) cases with enhancing lesions, the raters visualized pathological enhancement in more than one category. DL-T1-MPRAGE was noninferior to Wave-CAIPI T1-MPRAGE for delineating enhancing lesions with unanimous agreement on all cases with enhancing pathology. DL-T1-MPRAGE was noninferior to Wave-CAIPI T1-MPRAGE in the perception of noise (p<0.0001), artifact (p<0.0001), sharpness (p=0.001). With respect to overall diagnostic image quality, DL- and Wave-T1-MPRAGE were rated as equivalent in 114 of 115 (99%) cases. The DL sequence was preferred in 1 of 115 (1%) cases. Figure 4 shows two representative cases acquired using Wave-CAIPI-T1-MPRAGE and DL-T1-MPRAGE. Conclusion: Deep-learning-accelerated MPRAGE achieved noninferior image quality to the state-of-the-art clinically validated Wave-CAIPI accelerated sequence. This new technique demonstrates robust diagnostic quality in visualizing intracranial enhancing pathology in all compartments while maintaining similar perception of noise and artifact. DL-T1-MPRAGE may be useful in accelerating image acquisition across a variety of clinical and research studies.Acknowledgements
This work was supported by a research grant from Siemens Healthineers.References
1. Ellingson B, Bendszus M, Boxerman J et al. Consensus recommendations for a standardized Brain Tumor Imaging Protocol in clinical trials. Neuro Oncol. 2015 Sep; 17(9): 1188–1198.
2. Rudie J.D., Gleason T., Barkovich M.J., Wilson D.M., Shankaranarayanan A., Zhang T., et al. Clinical assessment of deep learning-based super-resolution for 3D volumetric brain MRI. Radiol. Artif. Intell. 2022;4(2) .
3. Bash S., Wang L., Airriess C., Zaharchuk G., Gong E., Shankaranarayanan A., et al. Deep learning enables 60% accelerated volumetric brain MRI while preserving quantitative performance: a prospective, multicenter, multireader trial. AJNR Am. J. Neuroradiol. 2021;42(12):2130–2137.
4. Goncalves Filho ALM, Awan KM, Conklin J, Ngamsombat C, Cauley SF, Setsompop K, et al. Validation of a highly accelerated post-contrast wave-controlled aliasing in parallel imaging (CAIPI) 3D-T1 MPRAGE compared to standard 3D-T1 MPRAGE for detection of intracranial enhancing lesions on 3-T MRI. 2022:1–11.
5. Nakarmi U, Cheng JY, Rios EP, Mardani M, Pauly JM, Ying L, et al. Multi-scale Unrolled Deep Learning Framework for Accelerated Magnetic Resonance Imaging. Proc IEEE Int Symp Biomed Imaging. 2020;2020:1056-9.
6. Henschel L, Kugler D, Reuter M. FastSurferVINN: Building resolution-independence into deep learning segmentation methods-A solution for HighRes brain MRI. Neuroimage. 2022;251:118933.
7. Estler A, Hauser TK, Mengel A, Brunnee M, Zerweck L, Richter V, et al. Deep Learning Accelerated Image Reconstruction of Fluid-Attenuated Inversion Recovery Sequence in Brain Imaging: Reduction of Acquisition Time and Improvement of Image Quality. Acad Radiol. 2023.
8. Dai-Viet T, Li-Thiao-Te S, Luong M, Thuong L-T, Dibos F, Rocchisani JM. Example-based super-resolution for enhancing spatial resolution of medical images. Annu Int Conf IEEE Eng Med Biol Soc. 2016;2016:457-60.
9. Tian Q, Bilgic B, Fan Q, Ngamsombat C, Zaretskaya N, Fultz NE, et al. Improving in vivo human cerebral cortical surface reconstruction using data-driven super-resolution. Cereb Cortex. 2021;31:463-82. 10. Hammernik K, Klatzer T, Kobler E, et al. Learning a variational network for reconstruction of accelerated MRI data. Magn Reson Med 2018; 79: 3055–3071.
11. Afat S, Wessling D, Afat C et al (2022) Analysis of a Deep Learning-Based Superresolution Algorithm Tailored to Partial Fourier Gradient Echo Sequences of the Abdomen at 1.5 T: Reduction of Breath-Hold Time and Improvement of Image Quality. Invest Radiol 57:157-162
Figures