3695
Towards predicting tumor pathology with radiopathomic analysis of multi-parametric MRI in patients with newly-diagnosed gliomas1Radiology and Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States, 2UCSF/UC Berkeley Graduate Program in Bioengineering, University of California, San Francisco, San Francisco, CA, United States, 3Center for Intelligent Imaging, University of California, San Francisco, San Francisco, CA, United States, 4Department of Pathology, University of California, San Francisco, San Francisco, CA, United States
Synopsis
Keywords: Tumors (Pre-Treatment), Tumor
Motivation: Noninvasive identification of malignant regions in glioma can help guide diagnosis and subsequent treatment planning.
Goal(s): This study aims to create models to predict and elucidate limitations in radiopathomic mapping of invasiveness in glioma using multiparametric physiologic and metabolic MRI.
Approach: A large, unique multiparametric MRI dataset with tissue is leveraged to compare various machine learning models of %ki-67 and cellularity (cells/mm2).
Results: : The best binary model achieved a CV-AUC =0.82 and CV-AUC = 0.75 for a binarized ki-67 and cellularity. Best ki-67 continuous predictions were in the 10-fold CV SVM and 4-fold ensemble model for continuous cellularity.
Impact: Multiparametric MRI can non-invasively predict histopathology. Including physiologic and/or metabolic MRI boosts histopathological predictions, however performance is also impacted by standardization of data quality.
Introduction
The use of metabolic and physiologic MRI in combination with machine learning has the potential to enable noninvasive localization of the most proliferative tumor regions that could spatially guide biopsy sampling, aid the surgeon in increasing the extent of resection by defining more accurate tumor margins, identify areas of infiltrating tumor that remain after resection, and guide radiation treatment.1 This study leverages a unique multi-parametric MRI dataset with tissue samples of known spatial coordinates to noninvasively predict measures of cellular proliferation (%Ki-67) and cellularity (cells/mm2) and examine how dataset size and quality, input image parameters, and various training regimes can impact model predictions of histopathological measures.Methods
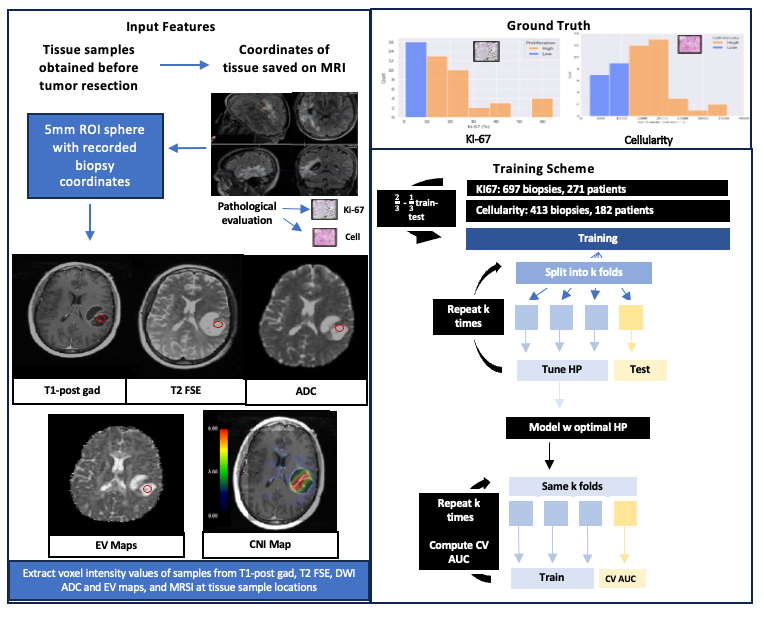
Subjects and Tissue Samples: 697 tissue samples from 271 patients newly-diagnosed with a pathologically confirmed glioma were analyzed in this study. One to ten tissue samples with known coordinates on MRI were evaluated histopathologically for the presence of tumor cellularity and proliferation with %Ki-67 (Figure 1).Image Acquisition: MR examinations were performed on a 3T GE scanner using an eight-channel phased-array head coil. Standard anatomical imaging included T2-weighted, T2-FLAIR, and pre-/post-contrast 3D T1-weighted IR-SPGR. Diffusion-weighted images were obtained with either 6 or 24 directions and b=1000s/mm2 or 55 directions and b=2000s/mm2 (1.2mm3 isotropic resolution). Lactate-edited 3D 1H-MRSI were acquired using PRESS volume localization, CHESS/VSS water/lipid suppression, and flyback-echo-planar readout (TR=1100-1250ms, TE=144ms, overpress-factor=1.5, nominal voxel-size=1cc, 988Hz sweep-width, and 712 dwell-points).
Processing: Anatomical and DWI data were aligned to the T1-post-contrast image and normalized to the mode of intensities in normal-appearing brain tissue. Mean voxel intensities from spherical 5-mm diameter ROIs centered at the location of the tissue samples were extracted from anatomic and DWI. For MRSI, spectral arrays were first shifted in k-space to reconstruct a spectral voxel centered at the coordinates of each tissue sample location before baseline-subtraction, frequency-/phase-correction, and quantification of peak heights and indices. A total of 23 imaging parameters (Figure 2) were quantified.
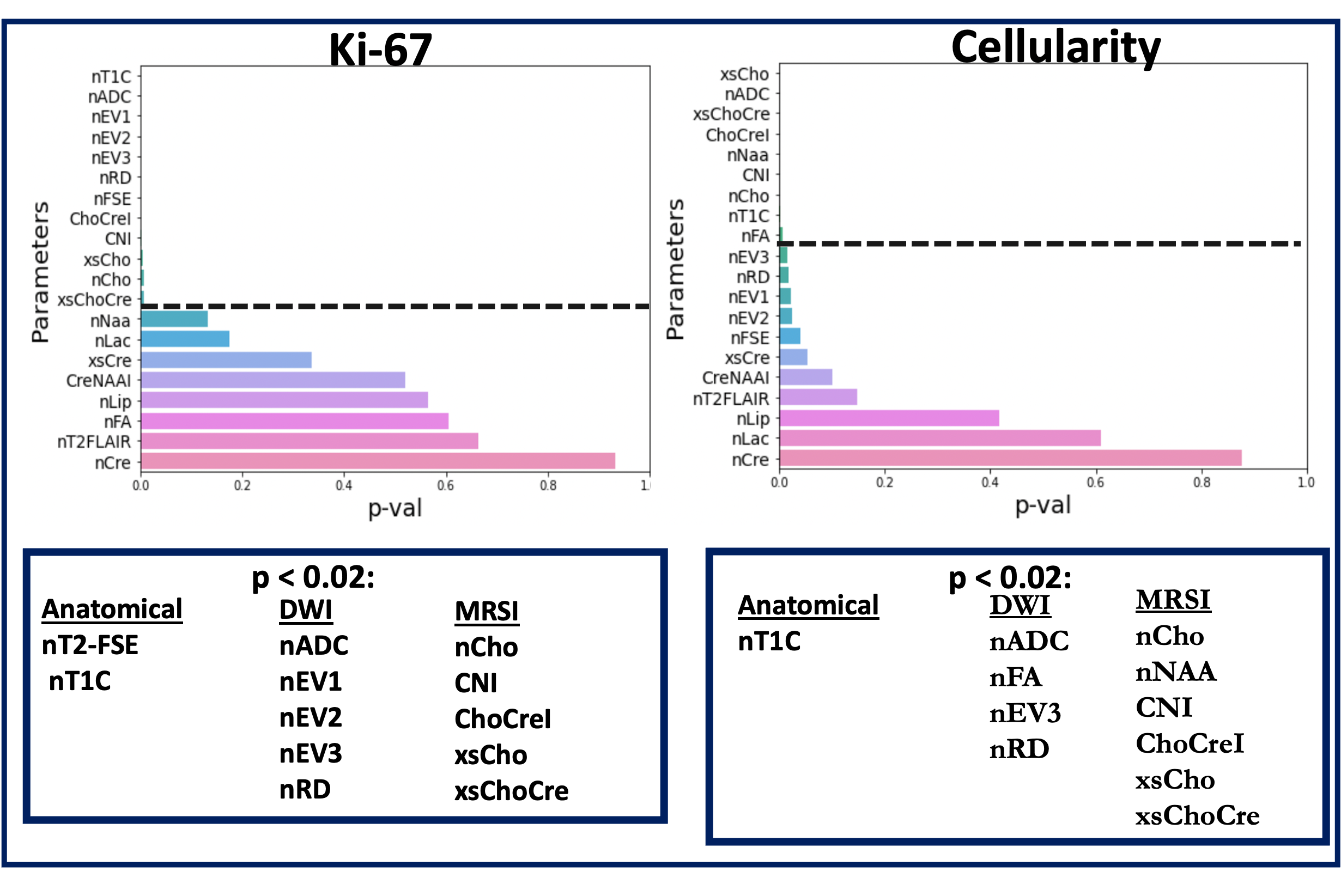
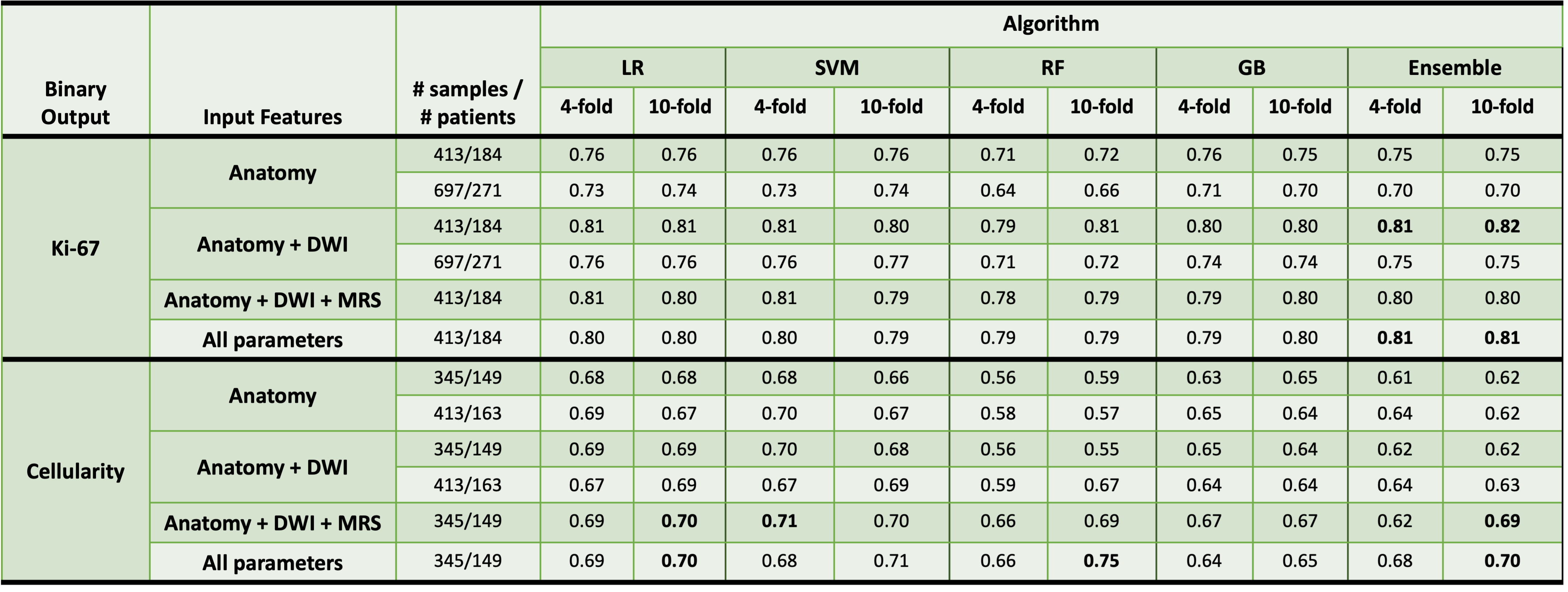
Machine Learning: Logistic (binary)/linear (continuous) regression, support vector machine (SVM), random forest (RF), gradient boosting (GB), and soft-voting ensemble algorithms were leveraged to build voxel-wise predictive models of binarized %ki-67 and cellularity, with a ki-67 threshold of 10% and cellularity of 1190 cells/mm2, as well as their continuous counterparts. The 23 imaging metrics were first tested for association with the histopathological measures through a univariate regression analysis with cutoff p-value<0.02 to determine significance for use in modeling (Figure 2). To examine the effects of including physiologic and metabolic MRI, variety of imaging protocols, cross-validation training schemes, and utility of performing feature selection, models with increasing inputs across all algorithms and training datasets were compared: anatomical-MRI-only, anatomical+DWI, anatomical+DWI+MRSI, and all parameters (no feature selection), trained with both 4-fold and 10-fold cross validation.
Results and Discussion
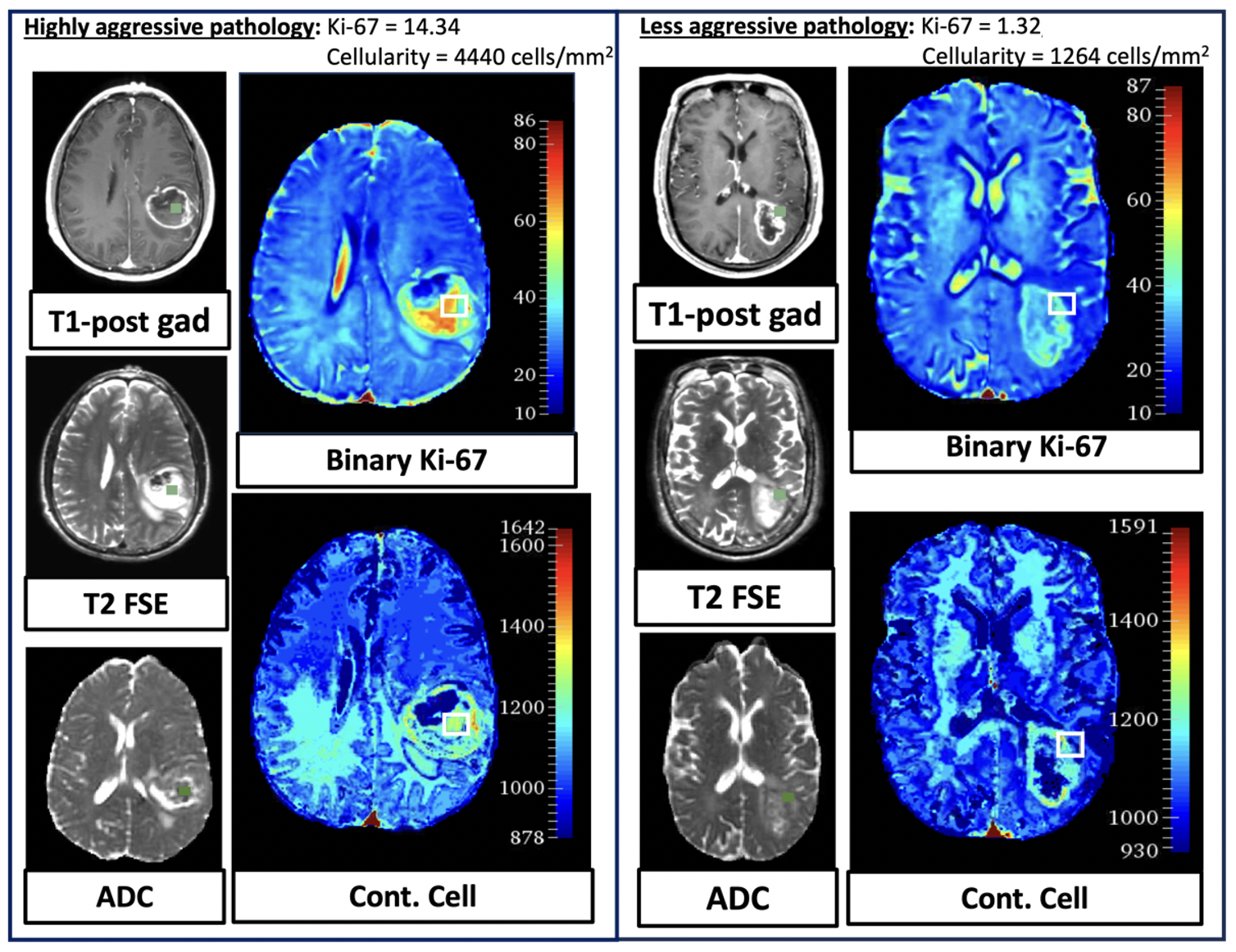
Predicting Ki-67: Figure 2 shows imaging metrics that are significantly associated with ki-67 and cellularity. As ADC was highly correlated with the remaining diffusion metrics which didn’t improve model performance, only ADC was utilized in subsequent modeling. Our best binary model achieved a CV-AUC=0.82 for a binarized ki-67 and utilized T2-FSE, T1C, and ADC as inputs into the ensemble algorithm trained on the smaller subset of data with uniform acquisition protocol (Figure 3). The addition of ADC demonstrated the greatest impact on ki-67 prediction across all algorithms, training regimes, and training sets. MRS metrics and increasing the number of folds in CV did not significantly improve performance. For the continuous modeling (Figure 4), SVM outperformed the other ML algorithms, and 10-fold CV with the smaller dataset further improved performance. Example spatial maps are illustrated in Figure 5 for tissue samples with high and low ki-67.Predicting Cellularity: Our best model for predicting binarized cellularity achieved a CV-AUC=0.75 and included all possible input parameters from anatomic, DWI, and MRSI in an RF model. Models predicting cellularity also seemed to be more sensitive to training regime, as larger performance changes are seen between 4-fold and 10-fold cross validation and including metabolic metrics was helpful across all modeling strategies. The comparatively lower performance to ki-67 suggests that cellularity is harder to predict with imaging metrics despite increased input features and training data size. Ensemble with 4-fold CV outperformed the other ML algorithms for the continuous prediction. Spatial maps for high and low cellularity are similarly displayed in Figure 5.
Conclusion
Our results demonstrate the feasibility of radiopathomic mapping of newly-diagnosed gliomas and suggest that ki-67 is easier to predict than cellularity using advanced multiparametric non-invasive imaging metrics and highlights the importance of including ADC and higher-quality, uniform acquisition protocols for radiopathomic mapping with multi-parametric MRI.Acknowledgements
NIH-NCI: P01CA118816References
[1] Uehara, K., Sasayama, T., Miyawaki, D. et al. Patterns of failure after multimodal treatments for high-grade glioma: effectiveness of MIB-1 labeling index. Radiat Oncol 7, 104 (2012).Figures