3665
RAIDER: Rapid, anatomy-independent, deep learning-based chemical shift-encoded MRI1University College London, London, United Kingdom, 2University College London Hospital, London, United Kingdom
Synopsis
Keywords: Fat & Fat/Water Separation, Fat
Motivation: Despite recent advances, chemical shift-encoded MRI (CSE-MRI) remains a challenging problem and many algorithms are computationally expensive, leading to interest in deep learning-based methods. However, initial attempts have used convolutional neural networks (CNNs), which are limited by data requirements, poor generalisability across different anatomies (‘anatomy-dependence’) and training time.
Goal(s): To address these limitations, we propose a deep learning-based method known as RAIDER.
Approach: RAIDER uses two multilayer perceptrons (MLPs), each trained separately with simulated single-voxel data, to achieve ultrafast parameter estimation.
Results: RAIDER is several orders of magnitude faster than conventional fitting, with similar/better performance, and avoids the inherent limitations of CNN-based methods.
Impact: RAIDER delivers ‘ultrafast’ CSE-MRI processing whilst avoiding the data and training-time requirements and anatomy-dependence of CNN-based methods. It could simplify, accelerate and reduce the cost of CSE-MRI processing in both research and clinical practice.
Introduction
Chemical shift-encoded MRI (CSE-MRI) is a reliable, fast method for quantifying proton density fat fraction (PDFF) in a variety of organs and diseases (1–4). PDFF is now an established biomarker of hepatic steatosis (5–7), and is increasingly used in other organs including pancreas, muscle and bone marrow (8–13). A benefit of gradient echo-based techniques for PDFF quantification is that R2* measurements can be extracted simultaneously, enabling quantification of iron or calcium (14–16). Gradient echo-based CSE-MRI therefore provides a versatile method for assessing a variety of (patho)physiological processes.Despite the success of CSE-MRI, it remains challenging to consistently disentangle or separate the signals arising from water and fat. This challenge arises because the signal arising from water-dominant and fat-dominant tissues is very similar, giving rise to the so-called ’fat-water ambiguity’ problem. This issue can be particularly challenging in applications and anatomical regions where the B0 field is inhomogenous. Although sophisticated methods, including iterative region-growing methods (17,18) or graph-cut algorithms (19–22), have been developed to address this problem, these require potentially problematic assumptions, are computationally expensive and do not generalise well across different anatomies (‘anatomy-dependence’) or matrix sizes.
As a result of these limitations, there has been interest in using deep learning for CSE-MRI (23–26). However, initial attempts have relied on convolutional neural networks (CNNs), which typically require large training datasets and may not generalise beyond the specific anatomy and image matrix used for training. Furthermore, training CNNs is typically extremely slow, requiring many hours or even days (23–26).
To address these issues, we propose RAIDER, a method for Rapid, Anatomy-Independent DEep leaRning-based CSE-MRI, enabled by resolving model degeneracy.
Theory
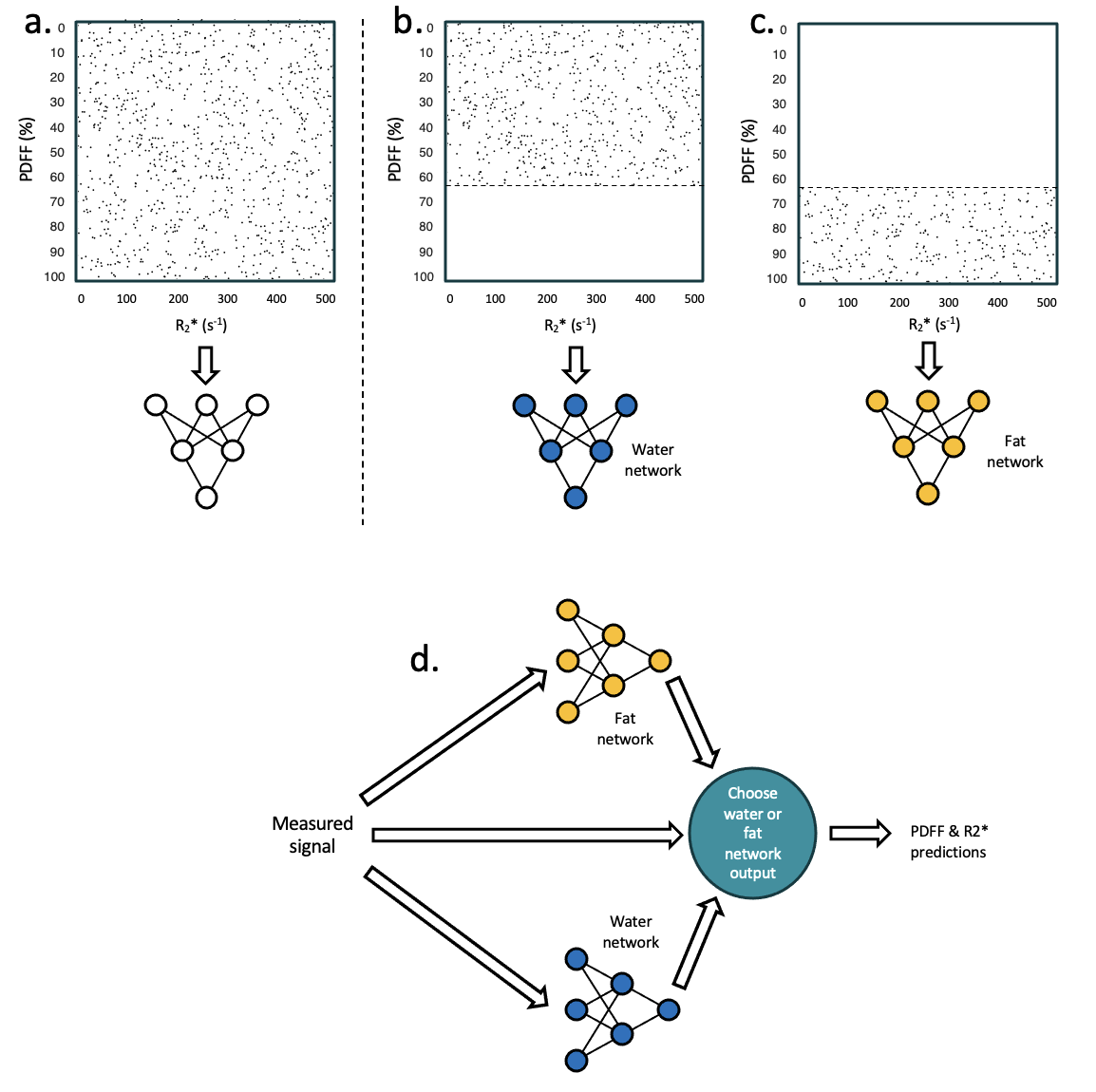
One way to substantially accelerate DL-based training and inference is to use multilayer perceptrons (MLPs) on single-voxel data rather than the much larger CNNs. However, a key challenge is that the MRI signal in a voxel can be very similar for two entirely different solutions (the ‘true’ and ‘swapped’ solutions). MLPs are typically unable to replicate such ‘one-to-many’ mappings and fail in these situations (27). Bishop suggested that this issue could be addressed by excluding implausible solutions from the parameter space during training (28); however, this approach does not help in situations where both candidate solutions are genuinely plausible, as with CSE-MRI.To address this, we use two separate networks, each trained on one part of parameter space, with the other ‘degenerate’ part of parameter space removed, to avoid degeneracy during training. Specifically, one ‘fat network’ is trained on the ‘high PDFF’ region of parameter space, with the low PDFF region excluded, and one ‘water network’ is trained on the ‘low PDFF’ region of parameter space, with the high PDFF region excluded (Figure 1a-c). The correct output from the two networks is chosen on the basis of fitting error or likelihood (Figure 1d).
Methods
The proposed approach was implemented using two MLPs (five fully-connected hidden layers with ELU activation functions), trained on simulated multi-echo gradient echo magnitude signals over the space of plausible PDFF and R2* values (Figure 1). Performance was assessed in simulation, a multisite, multivendor phantom dataset and in vivo datasets with various anatomies.Results and Discussion
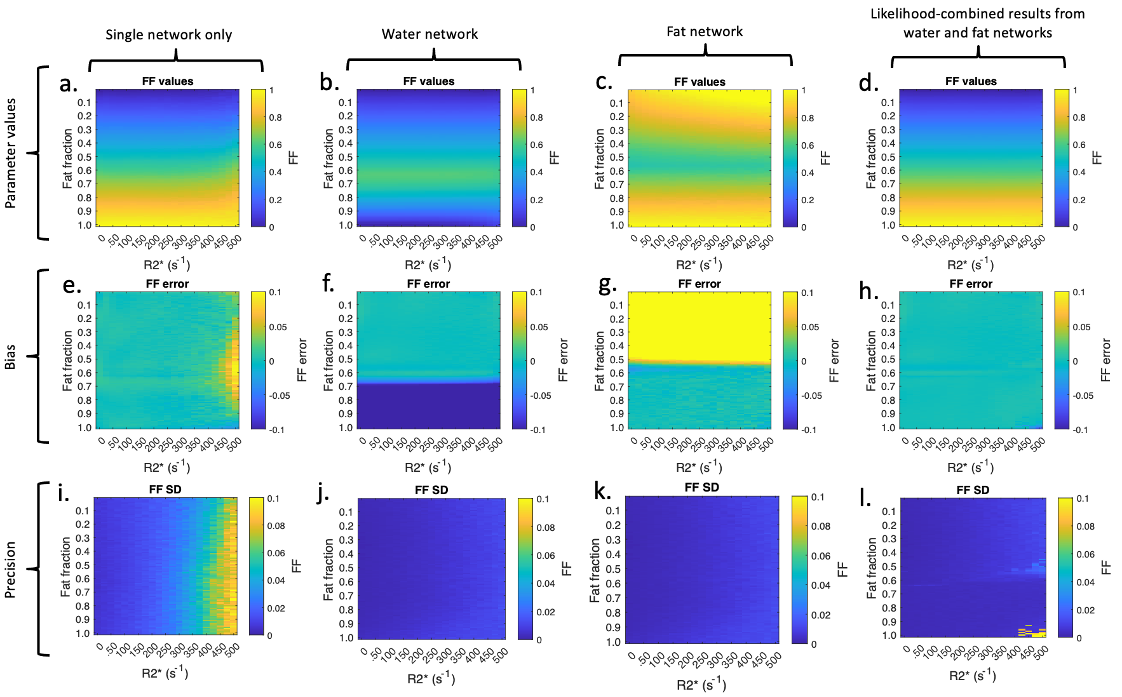
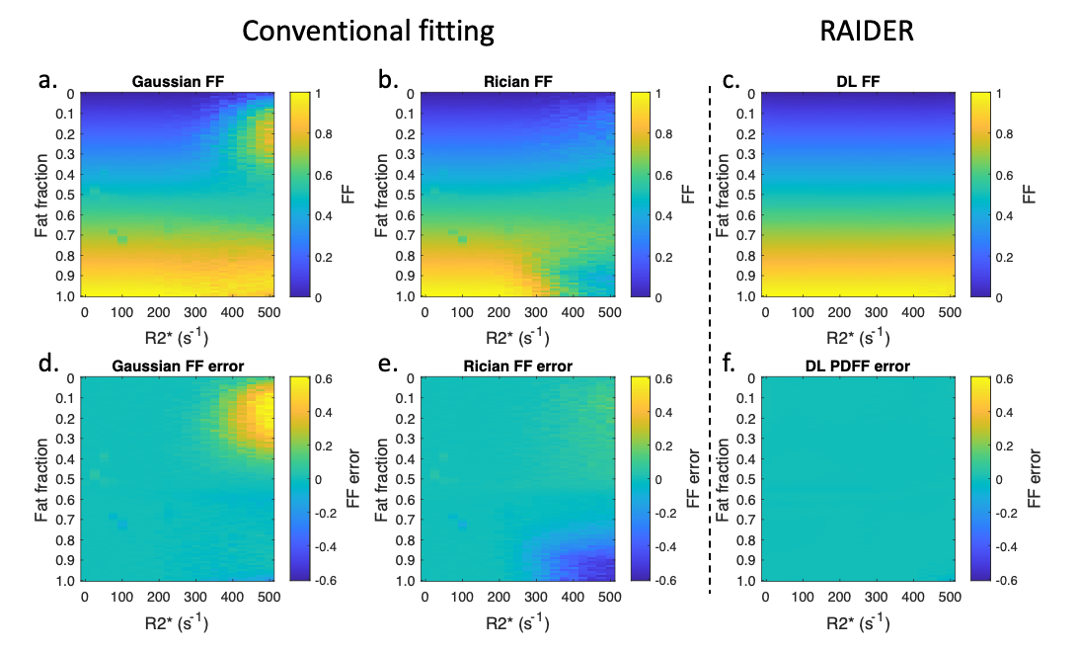
Figure 2 shows simulations demonstrating the performance of the dual network approach (RAIDER) compared to a single network. The single network produced estimates with relatively low bias at low R2* (e) but deteriorating bias and substantial imprecision (e,i) at high R2*. The individual RAIDER (water and fat) networks each produced good performance on the regions of parameter space they were trained on, and the likelihood-combined estimates produced low bias, high precision estimates across the parameter space (d,h,l).RAIDER substantially outperformed conventional fitting with both Gaussian and Rician likelihood models (Figure 3).
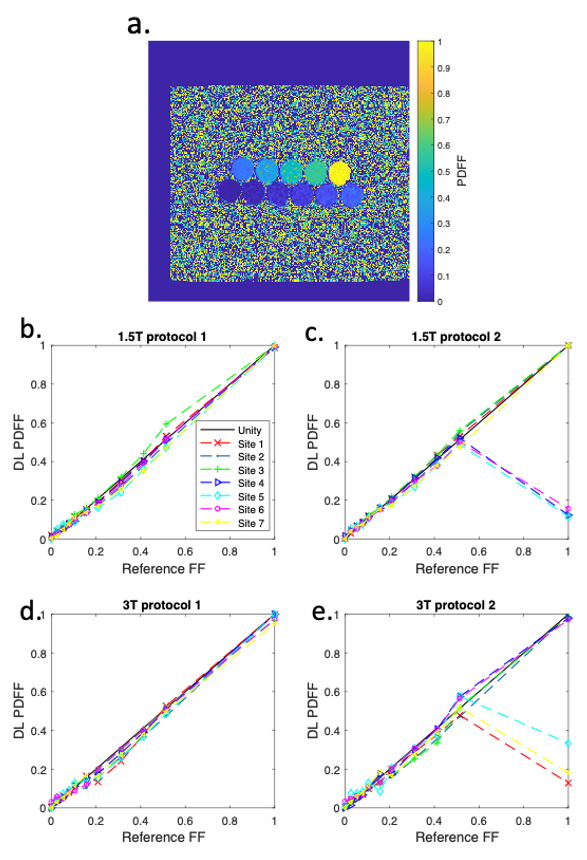
In the multivendor, multisite phantom dataset (Figure 4), RAIDER showed accurate measurements across field strengths and vendors, although with a degree of protocol dependence (performance was poorer for protocol 2), similar to with conventional magnitude fitting (29).
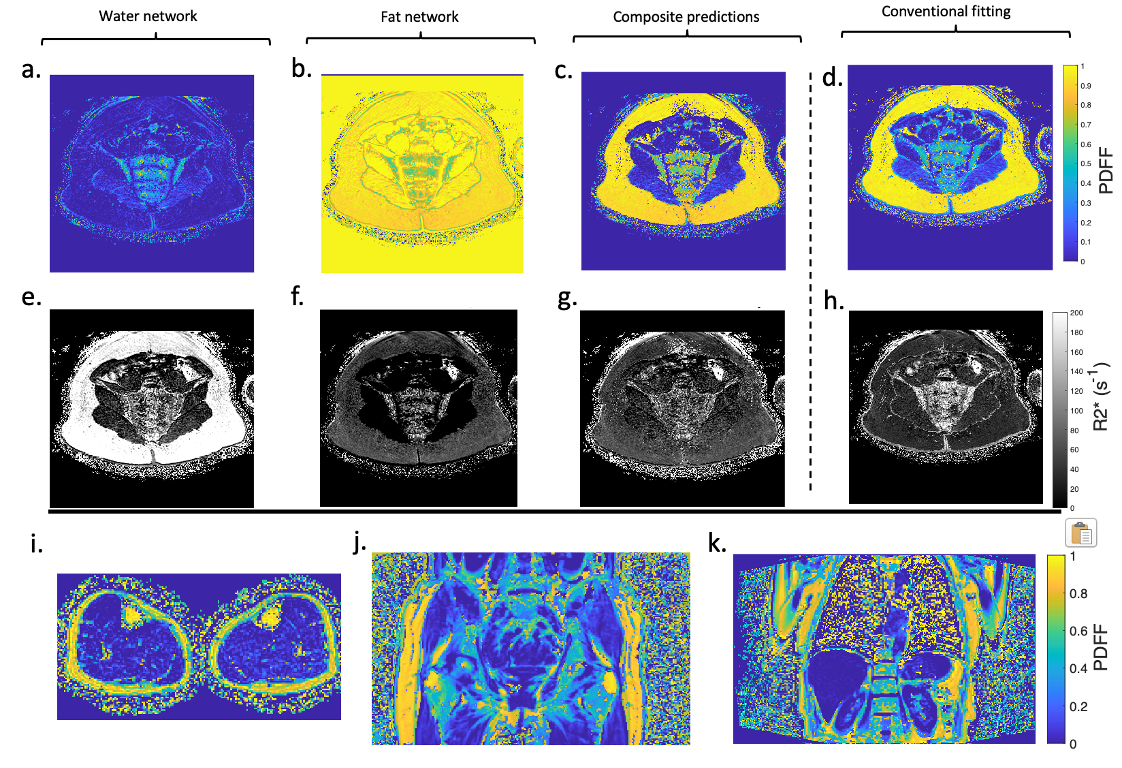
In vivo (Figure 5), RAIDER created good quality PDFF and R2* maps across a variety of anatomical regions.
Both RAIDER networks could be trained in 10-20 minutes. Inference was ~700 times faster than conventional fitting (29), taking 14𝜇𝑠/voxel compared to 10𝑚𝑠/voxel (1.3 seconds vs 15 minutes for a 300x300 slice).
Conclusion
RAIDER is several orders of magnitude faster than conventional fitting, with similar or better performance. It requires only simulated data for training, enabling it to generalise across matrix sizes and anatomies without anatomy-specific training, avoiding the anatomy dependence, data requirements and training time of CNN-based methods.Acknowledgements
Timothy J.P. Bray is supported by the Department of Health’s NIHR-funded Biomedical Research Centre at University College London Hospitals. Giulio V. Minore is supported by the EPSRC-funded UCL Centre for Doctoral Training in Intelligent, Integrated Imaging in Healthcare (i4health) (EP/S021930/1) and the Department of Health’s NIHR-funded Biomedical Research Centre at University College London Hospitals. This work was undertaken at UCLH/UCL, which receives funding from the UK Department of Health’s NIHR BRC funding scheme. The views expressed in this publication are those of the authors and not necessarily those of the UK Department of Health.References
1. Liu CY, McKenzie CA, Yu H, Brittain JH, Reeder SB. Fat quantification with IDEAL gradient echo imaging: Correction of bias from T1 and noise. Magn Reson Med. 2007;
2. Reeder SB, Wen Z, Yu H, Pineda AR, Gold GE, Markl M, et al. Multicoil Dixon Chemical Species Separation with an Iterative Least-Squares Estimation Method. Magn Reson Med. 2004;51(1):35–45.
3. Reeder SB, Pineda AR, Wen Z, Shimakawa A, Yu H, Brittain JH, et al. Iterative decomposition of water and fat with echo asymmetry and least-squares estimation (IDEAL): Application with fast spin-echo imaging. Magn Reson Med. 2005;54(3):636–44.
4. Yokoo T, Serai SD, Pirasteh A, Bashir MR, Hamilton G, Hernando D, et al. Linearity, Bias, and Precision of Hepatic Proton Density Fat Fraction Measurements by Using MR Imaging: A Meta-Analysis. Radiology. 2018;
5. Middleton MS, Van Natta ML, Heba ER, Alazraki A, Trout AT, Masand P, et al. Diagnostic accuracy of magnetic resonance imaging hepatic proton density fat fraction in pediatric nonalcoholic fatty liver disease. Hepatology. 2018;67(3):858–72.
6. Middleton MS, Heba ER, Hooker CA, Bashir MR, Fowler KJ, Sandrasegaran K, et al. Agreement Between Magnetic Resonance Imaging Proton Density Fat Fraction Measurements and Pathologist-Assigned Steatosis Grades of Liver Biopsies From Adults With Nonalcoholic Steatohepatitis. Gastroenterology. 2017;153(3):753–61.
7. Noureddin, M, Lam, J, Peterson, MR, Middleton, M, Hamilton G, Le T. Utility of magnetic resonance imaging versus histology for quantifying changes in liver fat in nonalcoholic fatty liver disease trials. Hepatology. 2013;58(6):1930–40.
8. Yoon JH, Lee JM, Lee KB, Kim SW, Kang MJ, Jang JY, et al. Pancreatic Steatosis and Fibrosis: Quantitative Assessment with Preoperative Multiparametric MR Imaging. Radiology. 2016;279(1):140–50.
9. Kühn JP, Berthold F, Mayerle J, Völzke H, Reeder SB, Rathmann W, et al. Pancreatic steatosis demonstrated at MR imaging in the general population: Clinical relevance. Radiology. 2015;276(1):129–36.
10. Morrow JM, Sinclair CDJ, Fischmann A, Machado PM, Reilly MM, Yousry TA, et al. MRI biomarker assessment of neuromuscular disease progression: A prospective observational cohort study. Lancet Neurol. 2015;15(1):65–77.
11. Janiczek RL, Gambarota G, Sinclair CDJ, Yousry TA, Thornton JS, Golay X, et al. Simultaneous T 2 and lipid quantitation using IDEAL-CPMG. Magn Reson Med. 2011;66(5):1293–302.
12. Bray TJP, Bainbridge A, Punwani S, Ioannou Y, Hall-Craggs MA. Simultaneous Quantification of Bone Edema/Adiposity and Structure in Inflamed Bone Using Chemical Shift-Encoded MRI in Spondyloarthritis. Magn Reson Med. 2018;79(2):1031–42.
13. Latifoltojar A, Hall-Craggs M, Bainbridge A, Rabin N, Popat R, Rismani A, et al. Whole-body MRI quantitative biomarkers are associated significantly with treatment response in patients with newly diagnosed symptomatic multiple myeloma following bortezomib induction. Eur Radiol. 2017;27(12):5325–36.
14. Hernando D, Kramer JH, Reeder SB. Multipeak fat-corrected complex R2* relaxometry: Theory, optimization, and clinical validation. Magn Reson Med. 2013;70(5):1319–31.
15. Hernando D, Levin YS, Sirlin CB, Reeder SB. Quantification of liver iron with MRI: State of the art and remaining challenges. Journal of Magnetic Resonance Imaging. 2014;
16. Wells SA, Schubert T, Motosugi U, Sharma SD, Campo CA, Kinner S, et al. Pharmacokinetics of Ferumoxytol in the Abdomen and Pelvis: A Dosing Study with 1.5- and 3.0-T MRI Relaxometry. Radiology. 2019;190489.
17. Yu H, Reeder SB, Shimakawa A, Brittain JH, Pelc NJ. Field map estimation with a region growing scheme for iterative 3-point water-fat decomposition. Magn Reson Med. 2005;54(4):1032–9.
18. Berglund J, Johansson L, Ahlström H, Kullberg J. Three-point Dixon method enables whole-body water and fat imaging of obese subjects. Magn Reson Med. 2010;63(6):1659–68.
19. Hernando D, Kellman P, Haldar JP, Liang ZP. Robust water/fat separation in the presence of large field inhomogeneities using a graph cut algorithm. Magn Reson Med. 2010;63(1):79–90.
20. Cui C, Wu X, Newell JD, Jacob M. Fat water decomposition using globally optimal surface estimation (GOOSE) algorithm. Magn Reson Med. 2015 Mar 1;73(3):1289–99.21. Cui C, Shah A, Wu X, Jacob M. A rapid 3D fat–water decomposition method using globally optimal surface estimation (R-GOOSE). Magn Reson Med. 2018 Apr 1;79(4):2401–7.
22. Berglund J, Skorpil M. Multi-scale graph-cut algorithm for efficient water-fat separation. Magn Reson Med. 2017 Sep 1;78(3):941–9.
23. Goldfarb JW, Craft J, Cao JJ. Water–fat separation and parameter mapping in cardiac MRI via deep learning with a convolutional neural network. Journal of Magnetic Resonance Imaging. 2019 Aug 1;50(2):655–65.
24. Andersson J, Ahlström H, Kullberg J. Separation of water and fat signal in whole-body gradient echo scans using convolutional neural networks. Magn Reson Med. 2019 Sep 1;82(3):1177–86.
25. Jafari R, Spincemaille P, Zhang J, Nguyen TD, Luo X, Cho J, et al. Deep neural network for water/fat separation: Supervised training, unsupervised training, and no training. Magn Reson Med. 2021 Apr 1;85(4):2263–77.
26. Liu K, Li X, Li Z, Chen Y, Xiong H, Chen F, et al. Robust water–fat separation based on deep learning model exploring multi-echo nature of mGRE. Magn Reson Med. 2021 May 1;85(5):2828–41.
27. Guerreri M, Epstein S, Azadbakht H, Zhang H. Resolving Quantitative MRI Model Degeneracy with Machine Learning via Training Data Distribution Design. In 2023. p. 3–14.
28. Bishop C, Roach C. Fast curve fitting using neural networks. Rev Sci Instrum. 1992;63(10):4450–6.
29. Bray TJP, Bainbridge A, Lim E, Hall-Craggs MA, Zhang H. MAGORINO: Magnitude-only fat fraction and R*2 estimation with Rician noise modeling. Magn Reson Med. 2023 Mar 1;89(3):1173–92.
Figures