3656
Preoperative prediction of IDH1-mutation in intrahepatic cholangiocarcinoma based on Gd-EOB-DTPA-enhanced MRI and MRI-derived habitats1The First Affiliated Hospital, Sun Yat-Sen University, guangzhou, China, 2The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, China
Synopsis
Keywords: Liver, Cancer, Habitat imaging
Motivation: Isocitrate dehydrogenase 1 (IDH1) mutation is an important therapeutic target for intrahepatic cholangiocarcinoma (ICC).
Goal(s): To achieve non-invasive prediction of IDH1 mutation in ICC to assist in clinical management.
Approach: Preoperative Gd-EOB-DTPA-enhanced MRI features and clinical information were retrospectively collected. Habitat analysis was performed based on pre- and post-enhancement T1 maps. Nomogram prediction model was established based on filtered variables.
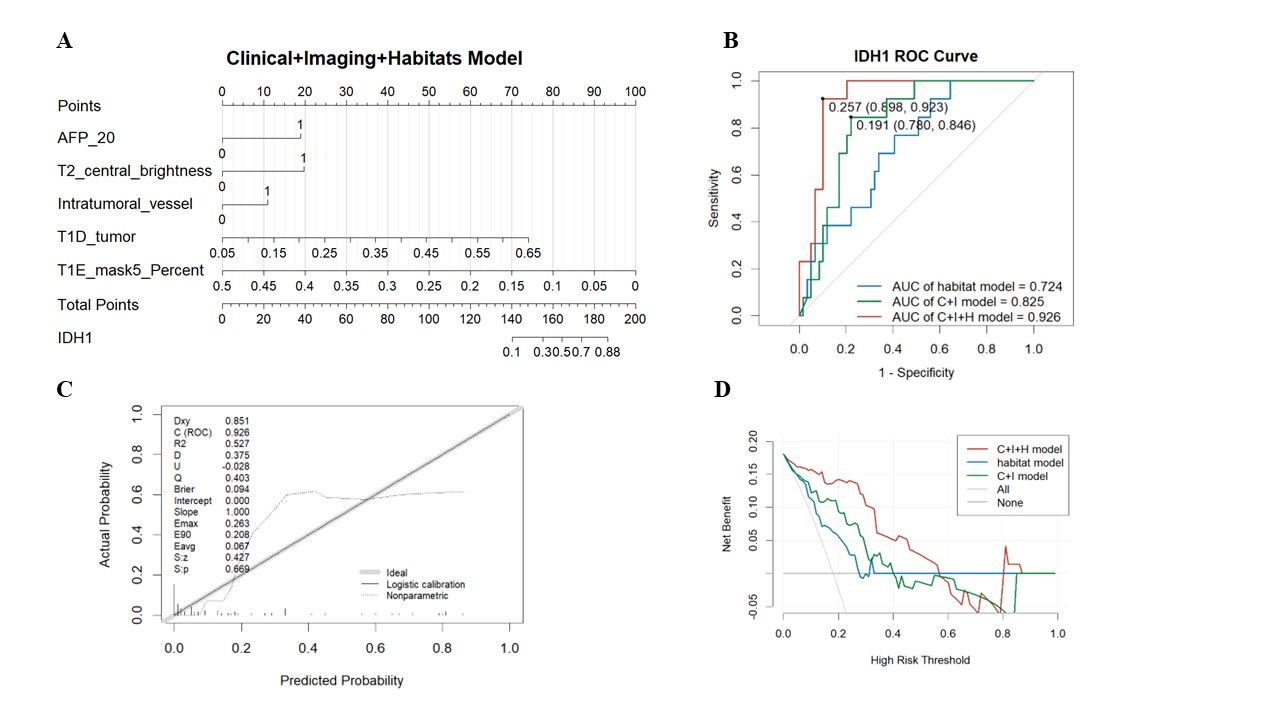
Results: Higher serum AFP level, higher T1 change ratio, more frequent intratumoral vessel and T2 central brightness, and habitat 5 are risk factors for IDH1-mutated ICC. The combined nomogram model demonstrated the highest diagnostic performance over the clinilal+imaging model and the habitat model.
Impact: The proposed strategy, Gd-EOB-DTPA-enhanced MRI and T1–based habitat imaging, can be applied for preoperatively and noninvasively identifying IDH1-mutation status in ICC, which offers potential benefits in terms to aid in clinical management.
Introduction
In recent years, the incidence of intrahepatic cholangiocarcinoma (ICC) has gradually increased, but with a poor 5-year survival rate of only 5-10% [1]. Innovative precision therapies are dedicated to finding genetic targets, with drugs targeting isocitrate dehydrogenase 1 (IDH1) mutations showing promising efficacy. Relevant drugs have been successively approved for ICC treatment and included in the subsequent-line therapy [2,3]. However, the mutation status of IDH1 depends on histopathological examination. Magnetic resonance imaging (MRI)-based imaging features and machine learning are widely studied to evaluate the microstructure of liver cancer which is important to enable non-invasive assessment [4,5]. Additionally, habitat imaging allows for the quantification and visualization of various subregions within the tumor [6,7]. The purpose of this study was to develop an approach using Gd-EOB-DTPA-enhanced MRI and MRI-derived habitat imaging for preoperatively predicting IDH1 mutation status of ICC.Methods
Eighty-five patients with preoperative Gd-EOB-DTPA-enhanced MRI examination were prospectively included and randomly assigned to the training set (n=59) and the test set (n=26). IDH1 mutation status was confirmed by next generation sequencing or immunohistochemical analysis. MRI including morphological T1WI, multi-phase enhanced imaging, hepatobiliary phase imaging, T2WI and pre- and post-enhanced T1 mapping on 3T systems (Verio/Prisma/Vida, Siemens Healthcare, Erlangen, Germany). MRI features were qualitatively and quantitatively reviewed by two radiologists. A clinical and imaging (C+I) nomogram model was developed by the risk factors from clinical variables and MRI features explored. Then validated and evaluated with the test set. The pre- and post-enhanced T1 mapping images were matched to outline tumors of two sequences with one region of interest. Matchable tumors without severe artifacts were screened for habitat analysis (n=73). The ICC lesions were divided into five habitats, and the volume fraction of each habitat was quantified. A combined nomogram model was constructed using the C+I nomogram model and habitat fraction. The diagnostic accuracy was evaluated using the area under the receiver operating characteristic curves (AUCs), and 95% confidence intervals (CIs). Delong test was used to compare the diagnostic accuracy of models. A p<0.05 was considered statistically significant.Results
The IDH1 mutation rate was 20% (17/85). IDH1-mutated ICC exhibited significantly higher serum AFP level, higher T1 change ratio, more frequent intratumoral vessel and T2 central brightness (p < 0.05), which were selected into the C+I model. C+I model performed well in both training and test set (AUC = 0.860 and 0.800). After habitat analysis, habitat 5 was identified as a risk factor for IDH1 and added to the combined model (Figure1). The combined nomogram model demonstrated the highest diagnostic performance (AUC = 0.926, 95% CI: 0.866-0.986), followed by the C+I model (AUC = 0.825, 95% CI: 0.724-0.927) and habitat model (AUC = 0.724, 95% CI: 0.586-0.861). Delong test indicates that the combined model outperforms the other two models (p < 0.05). Decision curve analysis implies that the combined nomogram model offered more net benefit in identifying IDH1 mutation compared to the other models.Discussion
This was a preliminary feasibility study of MRI and habitat analysis for the preoperative evaluation of IDH1 mutation in ICC. The results suggest that clinical information and imaging features are strongly associated with IDH1 mutations and allow for noninvasive prediction. As T1 change ratio was found to be an independent risk factor, we chose to conduct the habitat analysis based on pre- and post-contrast T1 mapping and identified habitat5 associated with IDH1 mutation. T1 change ratio in Gd-EOB-DTPA-enhanced MRI usually indicates cellular uptake of the contrast agent. Considering that the abundant fibrous and mucus components within the ICC may also allow the retention of contrast in the cellular interstitial space, the correlation needs further analysis. The association between IDH1 mutations and AFP levels is unclear in ICC [9]. As AFP is an important marker in hepatic stem cells, the relationship between IDH1 mutations and carcinogenesis also deserves further study. Although T2 central brightness was one of the risk factors included in the C+I model, the differences in T2 relative signal ratio (tumor: erector spinae) and ADC values were not significant. This may have been influenced by the small sample size and awaits further studies in the future.Conclusions
MRI and habitat imaging shows clinical potential for noninvasively and preoperatively determining the IDH1-mutation status of ICC with high accuracy, offering potential benefits in terms to aid in clinical management.Acknowledgements
Not applicable.References
1.Brindley PJ, Bachini M, Ilyas SI, Khan SA, Loukas A, Sirica AE, Teh BT, Wongkham S, Gores GJ. Cholangiocarcinoma. Nat Rev Dis Primers. 2021 Sep 9;7(1):65. doi: 10.1038/s41572-021-00300-2. PMID: 34504109; PMCID: PMC9246479.
2.Lavacchi D, Caliman E, Rossi G, Buttitta E, Botteri C, Fancelli S, Pellegrini E, Roviello G, Pillozzi S, Antonuzzo L. Ivosidenib in IDH1-mutated cholangiocarcinoma: Clinical evaluation and future directions. Pharmacol Ther. 2022 Sep;237:108170. doi: 10.1016/j.pharmthera.2022.108170. Epub 2022 Mar 13. PMID: 35296436.
3. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Biliary Tract Cancer (Version 2.2023- May 10, 2023). Fort Washington: NCCN, 2023.
4. Tang M, Zhou Q, Huang M, Sun K, Wu T, Li X, Liao B, Chen L, Liao J, Peng S, Chen S, Feng ST. Nomogram development and validation to predict hepatocellular carcinoma tumor behavior by preoperative gadoxetic acid-enhanced MRI. Eur Radiol. 2021 Nov;31(11):8615-8627. doi: 10.1007/s00330-021-07941-7. Epub 2021 Apr 20. PMID: 33877387.
5. Dong Z, Huang K, Liao B, Cai H, Dong Y, Huang M, Zhou X, Jia Y, Xu L, Luo Y, Li ZP, Feng ST. Prediction of sorafenib treatment-related gene expression for hepatocellular carcinoma: preoperative MRI and histopathological correlation. Eur Radiol. 2019 May;29(5):2272-2282. doi: 10.1007/s00330-018-5882-4. Epub 2018 Dec 13. PMID: 30547202.
6. Min JH, Kim YK, Choi SY, Kang TW, Lee SJ, Kim JM, Ahn S, Cho H. Intrahepatic Mass-forming Cholangiocarcinoma: Arterial Enhancement Patterns at MRI and Prognosis. Radiology. 2019 Mar;290(3):691-699. doi: 10.1148/radiol.2018181485. Epub 2019 Jan 8. PMID: 30620253.
7. Verma R, Correa R, Hill VB, Statsevych V, Bera K, Beig N, Mahammedi A, Madabhushi A, Ahluwalia M, Tiwari P. Tumor Habitat-derived Radiomic Features at Pretreatment MRI That Are Prognostic for Progression-free Survival in Glioblastoma Are Associated with Key Morphologic Attributes at Histopathologic Examination: A Feasibility Study. Radiol Artif Intell. 2020 Nov 11;2(6):e190168. doi: 10.1148/ryai.2020190168. PMID: 33330847; PMCID: PMC7706886.
8. Zhang Y, Yang C, Sheng R, Dai Y, Zeng M. Predicting the recurrence of hepatocellular carcinoma (≤ 5 cm) after resection surgery with promising risk factors: habitat fraction of tumor and its peritumoral micro-environment. Radiol Med. 2023 Oct;128(10):1181-1191. doi: 10.1007/s11547-023-01695-6. Epub 2023 Aug 19. PMID: 37597123.
9.Wang C, Jing H, Sha D, Wang W, Chen J, Cui Y, Han J. HBV-associated intrahepatic cholangiocarcinoma with high serum alpha-fetoprotein: a case report with review of literature. BMC Infect Dis. 2016 Jun 14;16:295. doi: 10.1186/s12879-016-1643-7. PMID: 27301956; PMCID: PMC4908691.
Figures