3649
Deep Learning for Predicting Prostate Cancer with Gray-Zone Prostate-Specific Antigen Levels to Reduce Unnecessary Biopsies1Shaanxi Provincial People's Hospital, xi'an, China, 2Philips Healthcare, beijing, China, 3Philips Healthcare, xi'an, China
Synopsis
Keywords: Prostate, Machine Learning/Artificial Intelligence
Motivation: Radiologists face challenges in the accurate prediction of prostate cancer (PCa) with gray-zone PSA levels. Deep learning (DL) evaluated PCa with gray-zone PSA levels remains unclear.
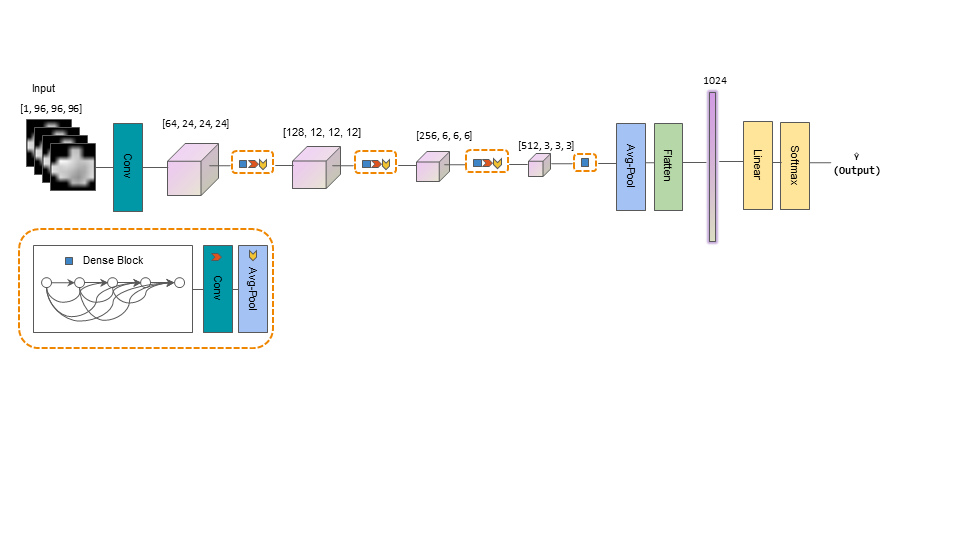
Goal(s): The aim of this work was to investigate the comparative performance of DL and radiologists. We trained a 3D DenseNet 121 model for automatic PCa classification with gray-zone PSA levels.
Approach: We trained a 3D DenseNet 121 model for automatic PCa classification with gray-zone PSA levels.
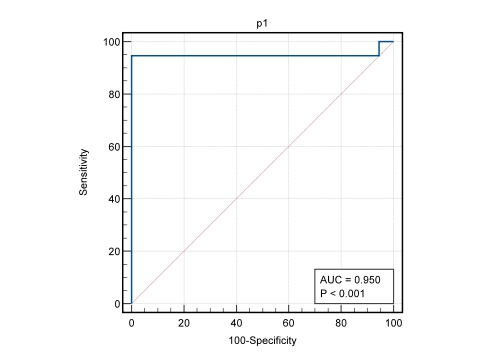
Results: The DL model yielded an AUC of 0.95 (0.85-1.0) for the identification of PCa with gray-zone PSA levels in the test set, significantly improving performance over the inexperienced radiologists.
Impact: The deep learning model yielded an AUC of 0.95 (0.85-1.0) for the identification of PCa with gray-zone PSA levels in the test set, significantly improving performance over the inexperienced radiologists.
Introduction
Gray-zone prostate-specific antigen (PSA) levels (4–10.0 ng/mL) have poor sensitivity and specificity for prostate cancer (PCa) prediction, and biopsy results have been reported to be positive in only 11.8–25% of patients with gray-zone PSA levels. This indicates that 75–88.2% of patients undergo unnecessary needle biopsies, putting them at risk of complications. Multiparametric magnetic resonance imaging (mp-MRI) based on Prostate Imaging Reporting and Data System (PI-RADS) has shown a moderate-to-good diagnostic performance in the prediction of PCa in patients with gray-zone PSA levels. PI-RADS exhibits certain limitations, notably its low specificity and inadequate inter-reader reproducibility.Thus, it is necessary to develop a quantitative and objective diagnostic method to improve the performance of PI-RADS for predicting PCa in patients with gray-zone PSA levels. The conventional Radiomics approach requires considerable effort in carefully engineering the features and using feature selection strategies before training a machine learning classifier. Deep learning(DL) approaches with the use of convolutional neural networks are gaining prominence in research studies for the characterisation of PCa. However, DL has not yet been assessed the PCa with gray-zone PSA levels.The aim of this work was to evaluate the comparative performance of DL and radiologists.Materials and methods
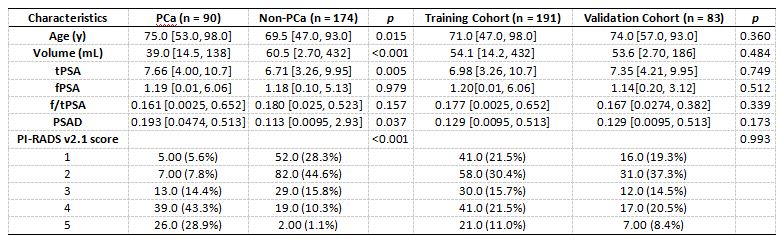
In all, 274 patients (184 non-PCa and 90 PCa) with gray-zone PSA levels that underwent mpMRI were included in this retrospective study. Among the 274 patients, 280 lesions (>50 mm3) were extracted (184 non-PCa and 96 PCa). MpMRI exams were prospectively reported using PI-RADS v2.1 by two inexperienced radiologists. The proposed DL framework is illustrated in Figure 1. We developed a framework using DenseNet 121 as the backbone. The 280 lesions were randomly divided with a 8:2 ratio into training and test sets (n=224 and 56, respectively) with stratified sampling. The training set contains 147 non-PCa and 77 PCa samples. The test set contains 37 non-PCa and 19 PCa samples. Data on the clinical risk factors related to PCa with gray-zone PSA levels (such as PI-RADS V2.1 category, age, prostate volume, and serum PSA level) were collected for all patients. Lesion volumes of interest (VOI) from T2-weighted imaging (T2WI) and apparent diffusion coefficient (ADC) imaging were annotated by two radiologists. The model was trained using ADC images. We used AUCs with 95% CIs to assess the performance on the test set and radiologists for the diagnosis of PCa with gray-zone PSA levels. The difference in AUCs between the models were tested for statistical significance using DeLong’s test.Results
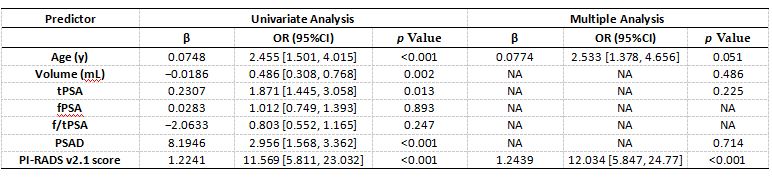
The univariate logistic regression analysis suggested that among clinical factors, patient age, PV, tPSA, PSAD, and PI-RADS V2.1 score were significant factors for predicting PCa in patients with PSA in the gray zone (table 1). The multiple logistic analysis showed that the PI-RADS V2.1 score were important factors that could be used as independent predictors. The outcomes of the univariate and multiple logistic regression analyses are presented in table 2. The AUC, sensitivity, and specificity of the radiologists were 0.866 (0.783–0.950), 0.842 (0.724–0.916), and 0.846 (0.655–0.941), respectively. The DL model based on case level yielded an AUC, sensitivity, and specificity of 0.95 (0.85-1.0) ,0.95 (0.74-1.0) and 0.97 (0.86-1) for identification of PCa with gray-zone PSA levels in the test data set(figure 2), significantly improving performance over the inexperienced radiologists.Discussion
In this study, we trained a DL model to identify PCa with gray-zone PSA levels on biparametric MRI. The DL model significantly outperformed inexperienced radiologists in identification of PCa, as indicated by DeLong’s test. An important role for MRI in PCa is to reduce the number of unnecessary biopsies in patients suspected of harboring clinical significantly PCa. Since DL predictions are given on a continuous scale, they allow for more precise configure ability compared to PI-RADS, which is reported on a five-point Likert scale. We cannot generalize our conclusions to all prostate MRI manufacturers. This generalization would require extending training with more data from other vendors.We plan to expand our data set by collecting multi-vendor data and constructed an integrated nomogram combining deep learning, PI-RADS score, and clinical variables to develop a more general DL CAD model in the future.Conclusions
DL, is an effective and non-invasive method for predicting PCa with gray-zone PSA levels. DL could reach better performance than inexperienced radiologists.Acknowledgements
We are grateful to all the participants for their cooperation and patience.References
1. Roobol, M.J.; Kranse, R.; Bangma, C.H.; et al. Screening for prostate cancer: Results of the Rotterdam section of the European randomized study of screening for prostate cancer. Eur. Urol. 2013, 64, 530–539.
2.Park, T.Y.; Chae, J.Y.; Kim, J.W.;et al. Prostate-specific antigen mass and free prostate-specific antigen mass for predicting the prostate volume of korean men with biopsy-proven benign prostatic hyperplasia. Korean J. Urol. 2013, 54, 609–614.
3. Huang, P.; Chen, Y.H.; Chen, S.H.; et al. Influence of prostatic calculi on the results of prostate biopsy in patients with a PSA level of 4-10μg /L. Natl. J. Androl. 2021, 27, 718–724.
4.Wang, R.; Wang, J.; Gao, G.; et al. Prebiopsy mp-MRI Can Help to Improve the Predictive Performance in Prostate Cancer: A Prospective Study in 1,478 Consecutive Patients. Clin. Cancer Res. 2017, 23, 3692–3699.
5.Mussi, T.C.; Yamauchi, F.I.; Tridente, C.F.; et al. Interobserver Agreement and Positivity of PI-RADS Version 2 Among Radiologists with Different Levels of Experience. Acad. Radiol. 2019, 26, 1017–1022.
6.Li, M.j.; Chen, T.; Zhao, W.l.;et al. Radiomics prediction model for the improved diagnosis of clinically significant prostate cancer on biparametric MRI. Quant. Imaging Med. Surg. 2020, 10, 368–379.
7.Liang, L.; Zhi, X.; Sun, Y.;et al. A Nomogram Based on a Multiparametric Ultrasound Radiomics Model for Discrimination Between Malignant and Benign Prostate Lesions. Front. Oncol. 2021, 11, 610785.
Figures