3643
Accelerating renal ASL MRI with 3D Cartesian TSE using deep learning-based Compressed SENSE.1Philips Healthcare, Shanghai, China, 2MR R&D, Philips Healthcare, Suzhou, China, 3MR Application, Philips Healthcare, Suzhou, China
Synopsis
Keywords: Kidney, Kidney, ASL, 3D Cartesian TSE, CS-AI, Deep Learning
Motivation: Motion and breathing can compromise 3D renal ASL MRI, reducing SNR and causing artifacts. Shorter-time acquisition is crucial for its clinical utility
Goal(s): To Evaluate the potential of CS-AI in accelerating renal ASL MRI with 3D Cartesian TSE.
Approach: We accelerated renal ASL MRI 2-, 4-, and 6 times using CS-AI, comparing with SENSE.
Results: CS-AI-accelerated images exhibited superior SNR and quality compared to SENSE, without affecting RBF quantification.
Impact: This study may enhance the clinical utility of 3D renal ASL, particularly in discerning perfusion alterations in small-sized lesions like small renal masses.
Introduction
Single-slice 2D readout is commonly suggested for renal ASL MRI due to its compatibility with multiple signal averages. However, it has limited spatial coverage [1]. Multi-slice 2D acquisition allows for greater coverage, but it may result in suboptimal background suppression (BGS) and SNR [2]. A promising alternative to 2D acquisitions is 3D Cartesian TSE, which offers improved SNR and is compatible with optimal BGS. It has demonstrated its potential in renal ASL studies [2-4]. However, due to the presence of breathing and more pronounced motion in the abdomen, prolonged scan times of 3D renal ASL can lead to reduced SNR and the potential for artifacts. This emphasizes the need to accelerate the acquisition for practical clinical application. A recent development is the introduction of a compressed sensing artificial intelligence (CS-AI) framework, which is based on an adaptive-CS-Network. This approach has demonstrated significant potential in accelerating various MR imaging techniques across different applications [5]. Therefore, the purpose of this study is to assess the feasibility of employing CS-AI to accelerate renal ASL imaging using 3D Cartesian TSE.Methods
Renal perfusion imaging was performed on a 3T Philips scanner (Ingenia Elition, Philips Healthcare, Best, The Netherlands) using pseudo-continuous arterial spin labeling (pCASL) with BGS. With IRB approval, the imaging was performed in five healthy volunteers in an axial orientation. The acquisition employed a 3D Cartesian TSE sequence with low-high profile ordering and a radial turbo direction. Additional parameters included: TR/TE = 4700/12 ms, FOV = 200x300x100 mm3, matrix = 68x102 with 33 slices, acquired resolution = 3x3x6 mm3, reconstructed resolution = 3x3x3 mm3, ETL = 80, echo spacing = 2.1 ms, label duration = 1.8 s, post-label delay = 1.8 s, NSA = 1, and 4 BGS pulses. CS-SENSE acquisitions were conducted with acceleration factors of 2-fold, 4-fold, and 6-fold, taking 3:00 min, 1:35 min, and 1:07 min, respectively. The acquired data were then reconstructed using an artificial intelligence (AI)-based algorithm. For comparison, SENSE acquisitions with 2-fold, 4-fold, and 6-fold accelerations were conducted in 2:33 min, 1:35 min, and 1:07 min, respectively. Additionally, an ASL acquisition with no acceleration was performed in 5:00 min, serving as a reference for image quality. To quantify Renal Blood Flow (RBF), M0 images were acquired using CS-AI with 2-fold, 4-fold, and 6-fold accelerations, in 1:30 min, 0:48 min, and 0:33 min, respectively. Additionally, M0 images were obtained without acceleration in 2:28 min.RBF quantification was carried out following the recommended method [1]. Subsequently, RBF maps were generated for each of the ASL/M0 acquisitions using CS-AI and for the acquisitions without acceleration. ROIs were manually delineated in various areas of the renal cortex on the RBF maps, and the mean RBF values within these ROIs were recorded. Linear regression and Bland-Altman analysis were employed to assess the agreement between the ROI-based mean RBF values calculated from the ASL/M0 images obtained with 2-fold accelerated CS-AI and those acquired without acceleration.
Results
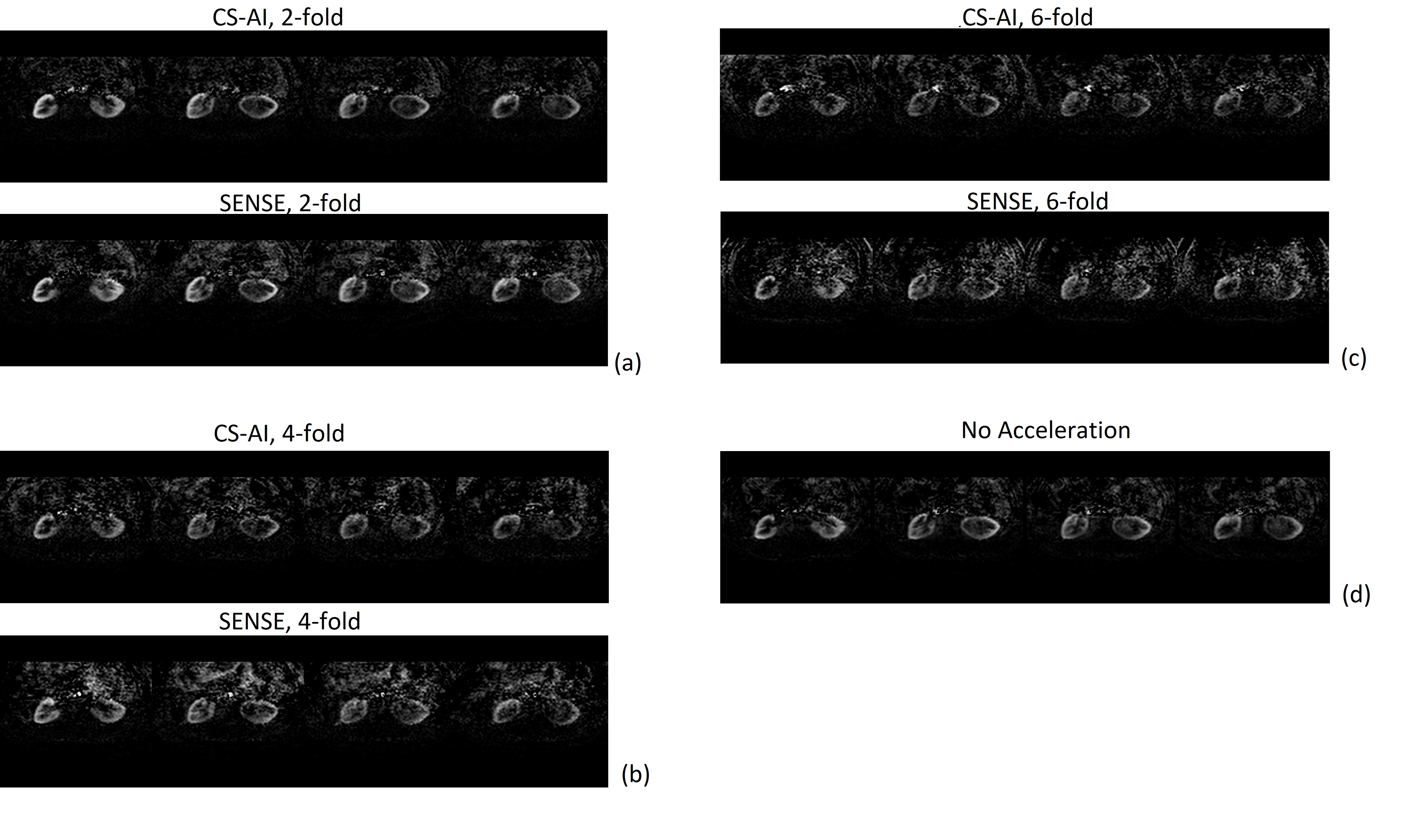
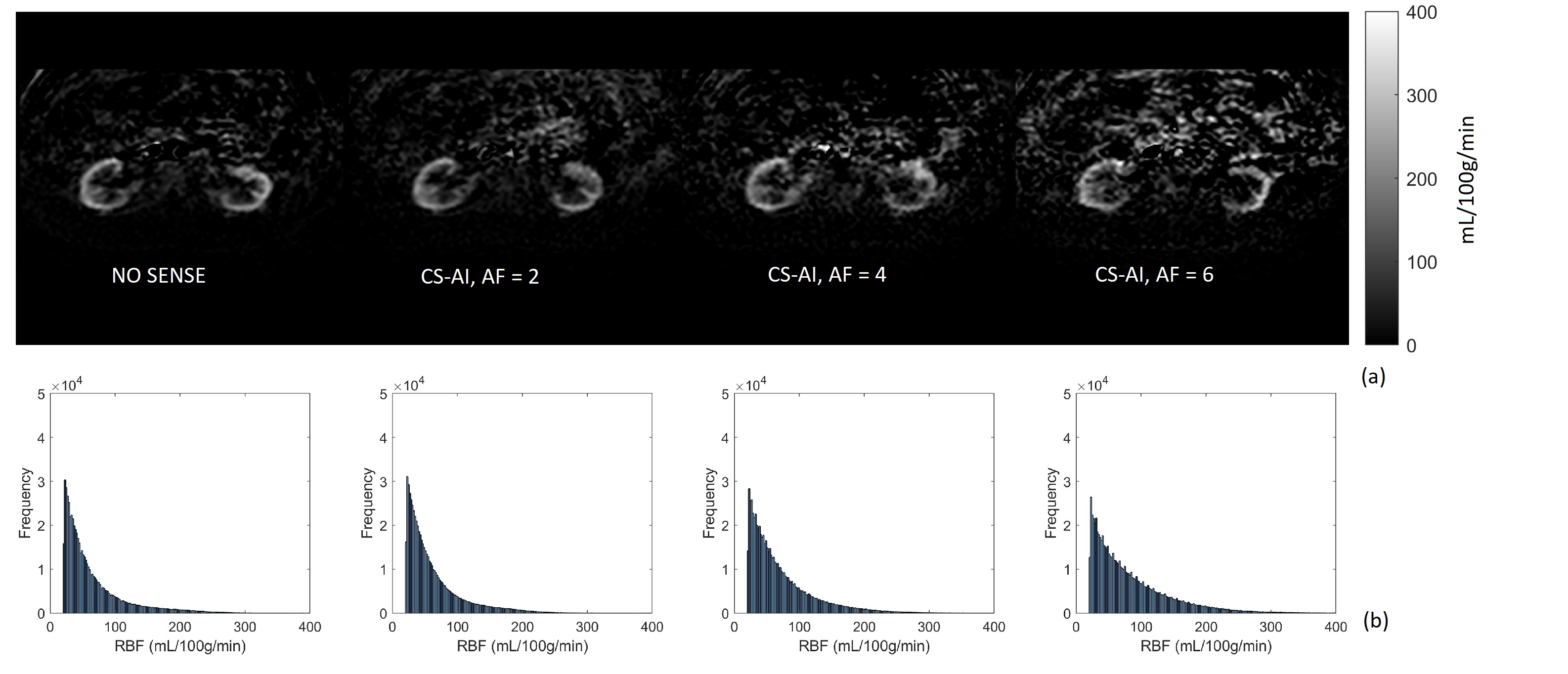
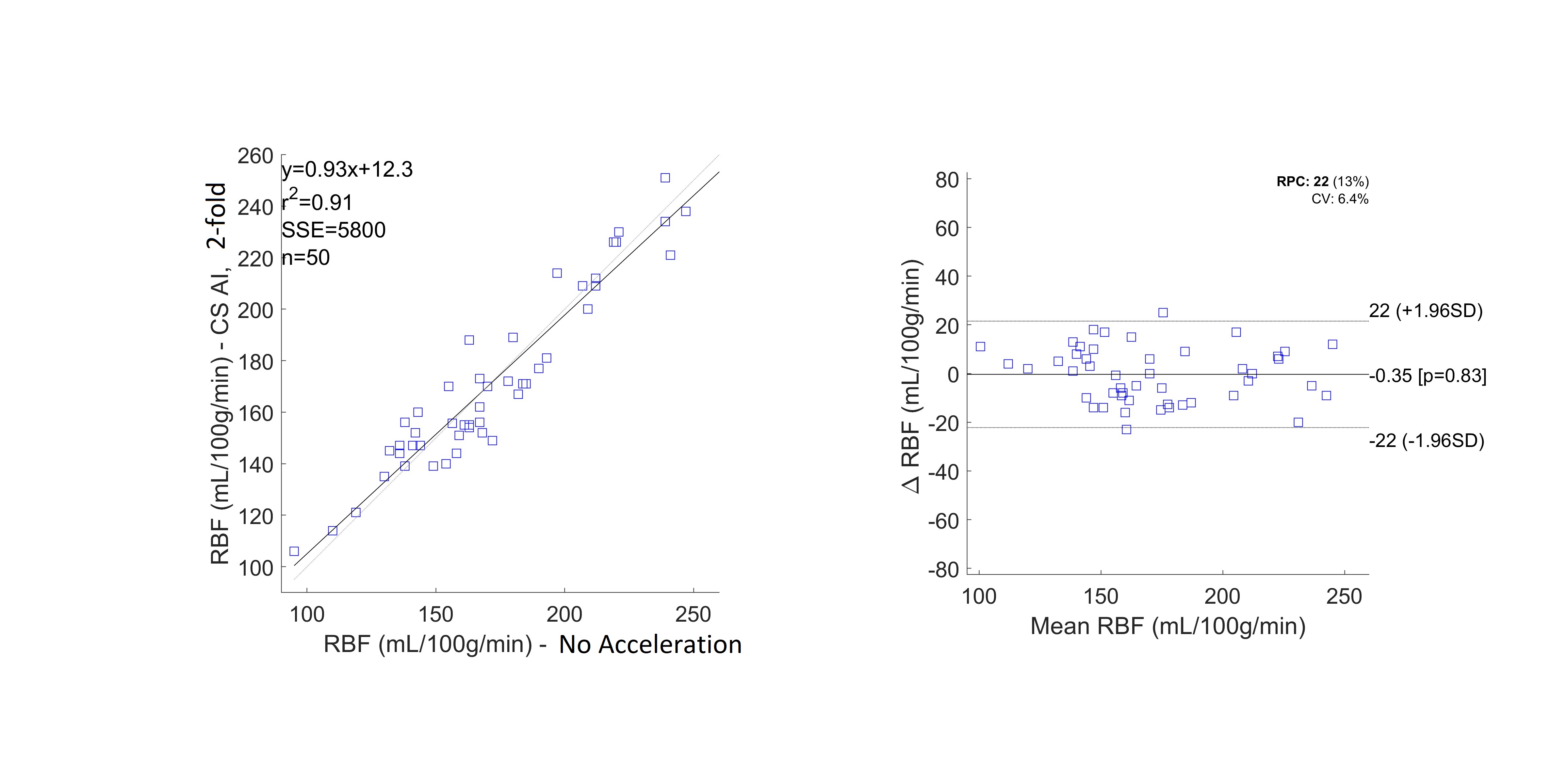
Renal perfusion-weighted images acquired at a spatial resolution of 3x3x6 mm³ using CS-AI exhibited good SNR (fig.1). When employing 2-fold (fig. 1a), 4-fold (fig. 1b), and 6-fold (fig. 1c) accelerations, the images acquired using CS-AI demonstrated markedly higher SNR and reduced background noise compared to those acquired using SENSE with equivalent accelerations. The images acquired with 2-fold accelerated CS-AI demonstrated similar image quality to those acquired without acceleration (fig. 1a & d). The RBF maps derived from ASL/M0 images acquired using CS-AI with 2-fold, 4-fold, and 6-fold accelerations agree well with the RBF map acquired without acceleration (fig. 2a). Moreover, the RBF distributions from CS-AI with varying accelerations closely match the one from the RBF map without acceleration (fig. 2b). This affirms that employing CS-AI with up to 6-fold acceleration does not introduce significant bias in RBF quantification. The RBF values acquired with no acceleration and using CS-AI with 2-fold acceleration exhibited a strong correlation (R² = 0.91, fig. 3a), along with excellent agreement and negligible bias (fig. 3b).Conclusion
We employed a compressed sensing artificial intelligence (CS-AI) framework to accelerate renal ASL MR imaging, using a 3D Cartesian TSE with a spatial resolution of 3x3x6 mm³. The perfusion-weighted images acquired with CS-AI demonstrated excellent SNR and image quality, surpassing those acquired with SENSE. Importantly, the use of CS-AI did not introduce bias in the quantification of RBF. This approach allows for clinically feasible 3D renal ASL MRI. Specifically, with CS-AI, 3D renal ASL/M0 acquisitions can be completed in 4:30 min, 2:23 min, and 1:40 min, with 2-fold, 4-fold, and 6-fold accelerations, respectively, without affecting RBF quantification.Acknowledgements
No acknowledgement found.References
[1] Nery, F et al. MAGMA 2020 Feb;33(1):141-161.
[2] Robson, PM et al. Acad Radiol 2016; 23(2):144-154.
[3] Taso, M et al. MRM 2019; 82(2):680-692.
[4] Greer, JS et al. MRM 2019; 82(5):1713-1724.
[5] Pezzotti N et al. IEEE Access 2020 ; 8:204825–204838.
[6] Forman SC et al. Euro Radiol 2022; 32:8376–8385.
Figures