3640
Evaluation of Common Bile Duct (CBD) dilatation by CT data using Synthetic MRCP data by Cycle-GAN and 3D VGG Network1KAIST, Daegeon, Korea, Republic of, 2KAIST, Daejeon, Korea, Republic of, 3Department of Radiology, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea, Republic of
Synopsis
Keywords: Digestive, Biliary
Motivation: Differentiating CBD dilatation with CT alone is challenging, often necessitating MRCP(Magnetic Resonance Cholangiopancreatography). Yet, patients forego MRCP due to cost and time constraints. Hence, predicting CBD dilatation using CT is vital for diagnosis.
Goal(s): Developing deep neural networks to assess CBD dilatation only with CT data.
Approach: Cycle-GAN and 3D VGG Networks predicted CBD dilatation, where Cycle-GAN generated synthetic MRCP from CT and 3D VGG Network predicted dilatation using this synthetic data.
Results: The network trained with synthetic MRCP data predicted CBD dilatation with an AUROC of 0.7231, 30% improvement over using CT data alone, enabling CT-only diagnosis.
Impact: This study introduces a transformative solution for CBD dilatation diagnosis, enabling assessments using Only-CT data from Cycle-GAN and 3D VGG Network. Achieving a 30% improvement in AUROC, it enables reliable CT-only diagnoses, overcoming scarce MRCP data and improve patient care.
Introduction
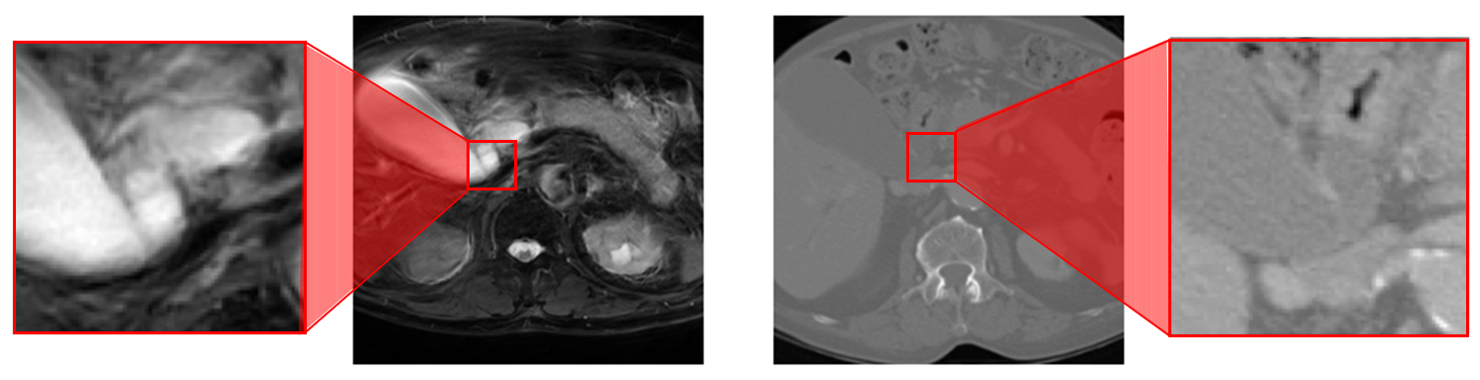
CBD (Common Bile Duct) dilatation is more readily detected on MRCP, which is a unique MRI technique for observing the liver, gallbladder, and bile ducts and the pancreas in patients with suspected hepatic or pancreatic diseases. MRCP data significantly contribute to diagnosis of CBD dilatation, whereas in CT data determining the exact dilatation is challenging. (Fig 1) However, many patients only take CT in the matter of time and/or cost. In this paper, we highlight the synergy of Cycle-GAN and VGG networks, strongly enhancing prediction performance only using CT data.Method
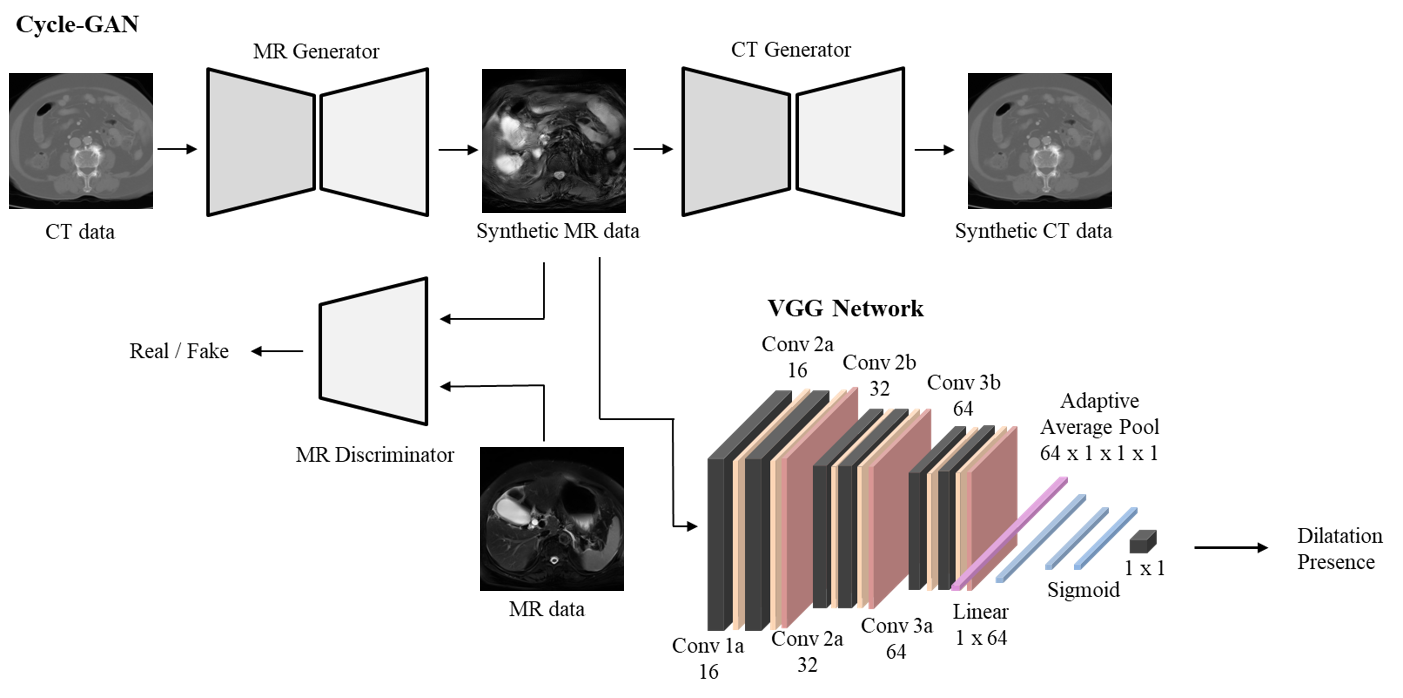
In this study, we identified CBD dilatation through neural networks trained with MRCP and CT data. The network enabled accurate dilatation diagnostics with only CT data. The network consisted of several fragmented networks. Cycle-Consistent Adversarial Network (Cycle-GAN) was trained on unpaired MRCP and CT data, generating synthetic MR images from CT images in test dataset. The Cycle-GAN output was used as an input of the VGG network that predicted the dilatation.
Data Acquisition and Preprocessing
The data were composed of a pair of CT and MRCP datasets of 99 subjects. The spacing of CT and MRCP datasets were both 1 × 6 × 1 mm3 , respectively and centered-cropped to size of 40x256x256, where CBD was focused and the image background was removed but still structural components of CT and MRCP data were included.
Cycle-GAN
In this paper, Cycle-GAN converted CT images into MRCP and then restored them back to their original CT form, ensuring consistency in the transformation process. Two Cycle-GAN generators use backbones, which were composed of 9 Resnet-blocks and two discriminators were composed with sequential Convolution blocks. The Cycle-GAN model was trained with epoch of 200 and learning rate of 2e-4. 66 patient data were used in training and 33 patient data were used to generate synthetic MRCP data.
3D VGG Model
The 3D VGG network was composed of several convolution blocks, batch normalization layer and pooling layers. The input volume passed through 3D-convolution blocks until channel size reached 64 and then passed through fully-connected layers generating evaluation of dilatation presence. Real and synthetic MRCP data of 66 patients were used as training set and 33 patients’ dataset were used to test the evaluation. The model was trained with 150 epochs, learning rate of 1e-4 with Adam optimizer.
Result
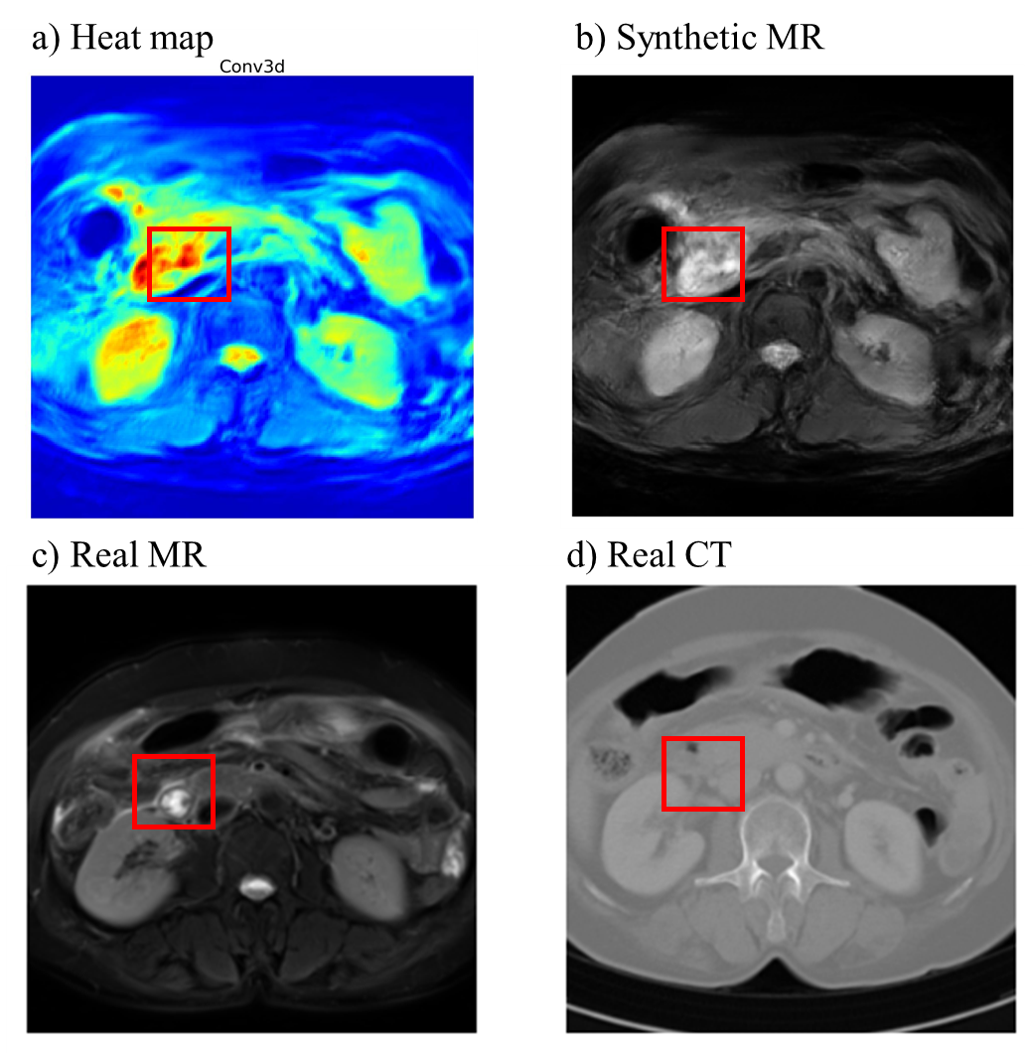
In Fig3.a, the heatmap derived from the last convolution layer of the 3D VGG Network offered qualitative insights into the areas of focus for classification, elucidating that the CBD region played a pivotal role in the final classification process.Fig3.b, c provides evidence that Cycle-GAN excels in capturing the CBD region, effectively generating synthetic MRCP images. Notably, Cycle-GAN highly reflected the structure of the CBD region, despite its lower intensity in CT images.
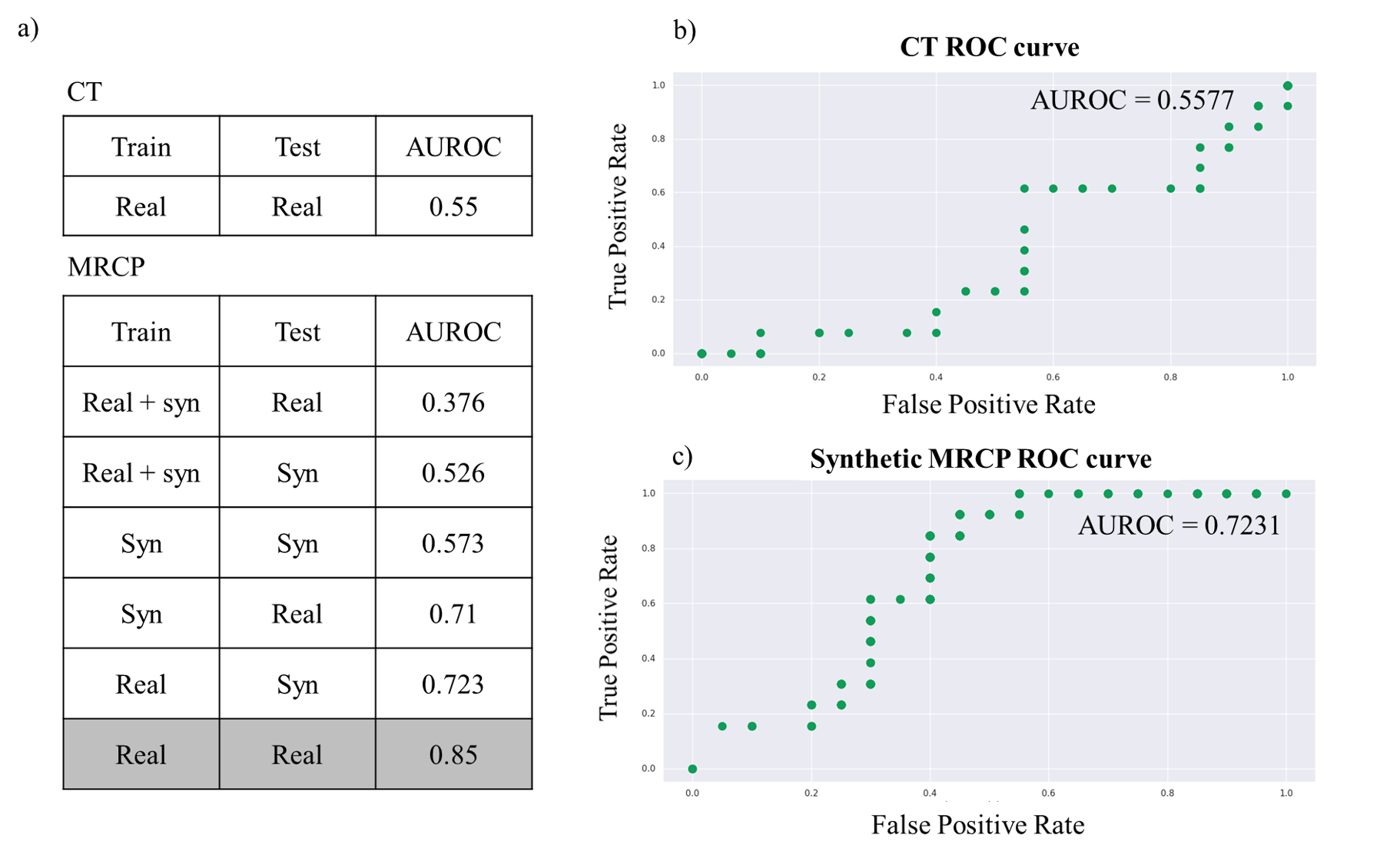
In Fig4, self-ablation study was conducted to evaluate the performance of the 3D VGG Network, presenting ROC curves and AUROC scores. The AUROC score obtained in the training and testing with real data represents an ideal outcome for a neural network and is a challenging goal to reach. The evaluation involving training with synthetic data and testing with real data demonstrates relatively high predictive performance. This suggests that synthetic MRCP data contains the necessary information for CBD dilatation assessment, as indicated by the heatmap in Fig3.a. When training with a mixture of real and synthetic data, it is anticipated that a conflict between the two sources of information may occur, resulting in a lower AUROC. In Fig4.b, when synthetic MRCP images were tested with the 3D VGG Network, an AUROC of 0.7231 was achieved. Conversely, in Fig4.c, when classifying using CT data alone, an AUROC of 0.5577 was attained.
Discussion
CT data often falls short in providing detailed information about the CBD even when used with the naked eye. Additionally, achieving accurate classification, even with neural networks, proves challenging, as shown by the AUROC values in Fig4.b. However, incorporating MRCP data offers a promising solution. By generating synthetic MRCP data closely aligned with authentic MRCP images, we achieve a significant nearly 30% improvement in AUROC, a noteworthy accomplishment. This approach overcomes the limitations of scarce MRCP data, enabling CBD dilatation detection even when using CT data alone, enhancing accessibility. Moreover, CBD is a specific abdominal area with limited research on diagnosis, making this study pivotal for future research. Furthermore, this approach offers substantial benefits to patients facing physical and financial constraints, as it allows for the assessment of the presence or absence of diseases, particularly in cases where obtaining MRCP images proves challenging.Acknowledgements
No acknowledgement found.References
[1] SIMONYAN, Karen; ZISSERMAN, Andrew. Very deep convolutional networks for large-scale image recognition. arXiv preprint arXiv:1409.1556, 2014.
[2] FARRELL, James J.; FERNÁNDEZ-DEL CASTILLO, Carlos. Pancreatic cystic neoplasms: management and unanswered questions. Gastroenterology, 2013, 144.6: 1303-1315.
[3] TSOUMAKAS, Grigorios; KATAKIS, Ioannis. Multi-label classification: An overview. International Journal of Data Warehousing and Mining (IJDWM), 2007, 3.3: 1-13.
[4] ZHU, Jun-Yan, et al. Unpaired image-to-image translation using cycle-consistent adversarial networks. In: Proceedings of the IEEE international conference on computer vision. 2017. p. 2223-2232.
Figures