3632
T2-weighted image radiomics nomogram to predict pancreatic serous and mucinous cystic neoplasms1Radiology, Changhai Hospital of Shanghai, Shanghai, China
Synopsis
Keywords: Pancreas, Pancreas
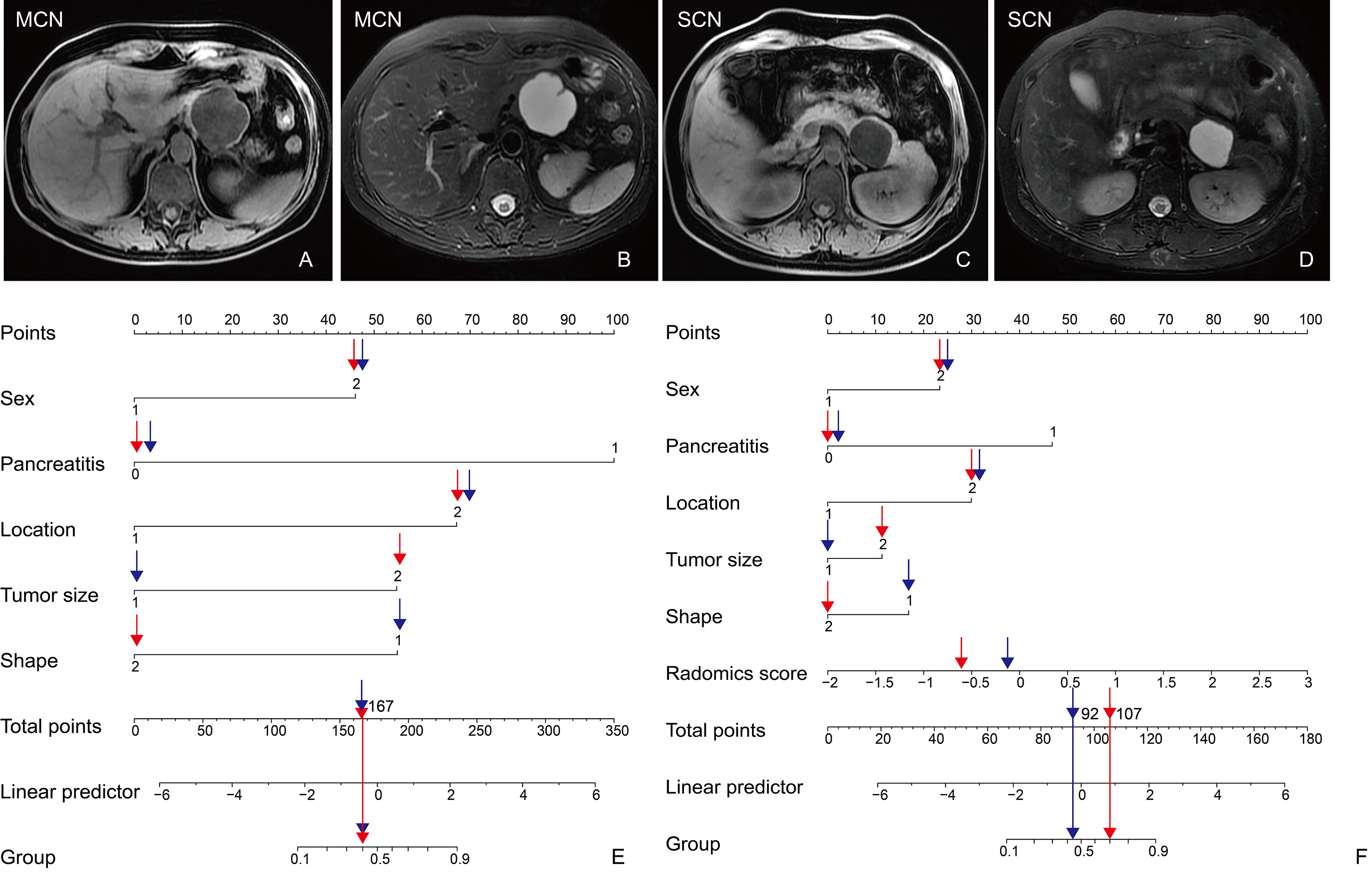
Motivation: Cystic fluid appears hyperintense via T2WI, the most sensitive detection method and T2WI is a conventional sequence. However, distinguishing pancreatic MCNs from SCNs using T2WI is difficult because both neoplasms appear as hyperintense lesions, especially when both are unilocular.
Goal(s): We aimed to develop and validate a T2WI radiomics nomogram for the differentiation of SCNs from MCNs.
Approach: A radiomics model that was included clinical characteristics, MRI characteristics, and T2WI rad-scores for differentiating MCNs from SCN.
Results: We developed and validated a T2WI radiomics nomogram that functions as a non-invasive and convenient tool for preoperatively predicting the presence of SCNs and MCNs.
Impact: The tool has the potential to help clinicians identify patients requiring surveillance or surgery.
Objectives
To develop and validate a T2-weighted image (T2WI) radiomics nomogram for the prediction of pancreatic serous cystic neoplasm (SCN) and mucinous cystic neoplasm (MCN).Methods
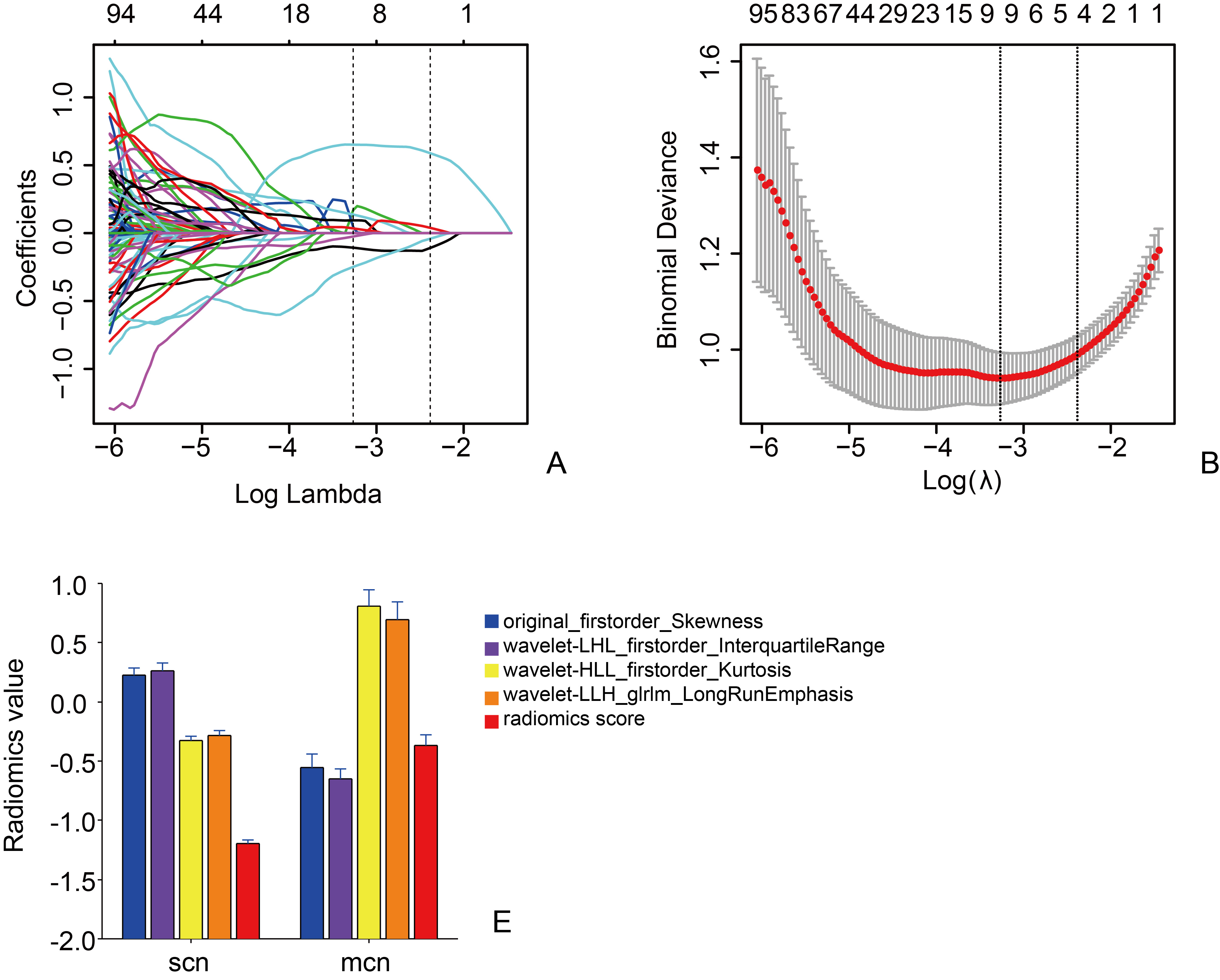
In this retrospective study, a total of 304 patients underwent MRI and surgical resection. Radiomics features were extracted from T2WI. A clinical model was constructed with clinical and imaging characteristics. A radiomics model included T2WI radiomics score, clinical and imaging characteristics. A multivariable logistic regression models were developed basing on a training cohort consisting of 159 patients with SCN and 64 patients with MCN between March 2011 and December 2018. The performance of the nomograms was determined by its’ discrimination, calibration, and clinical usefulness. The models were validated in 81 consecutive patients between January 2019 and December 2021, of which 57 and 24 patients had SCN and MCN, respectively.Results
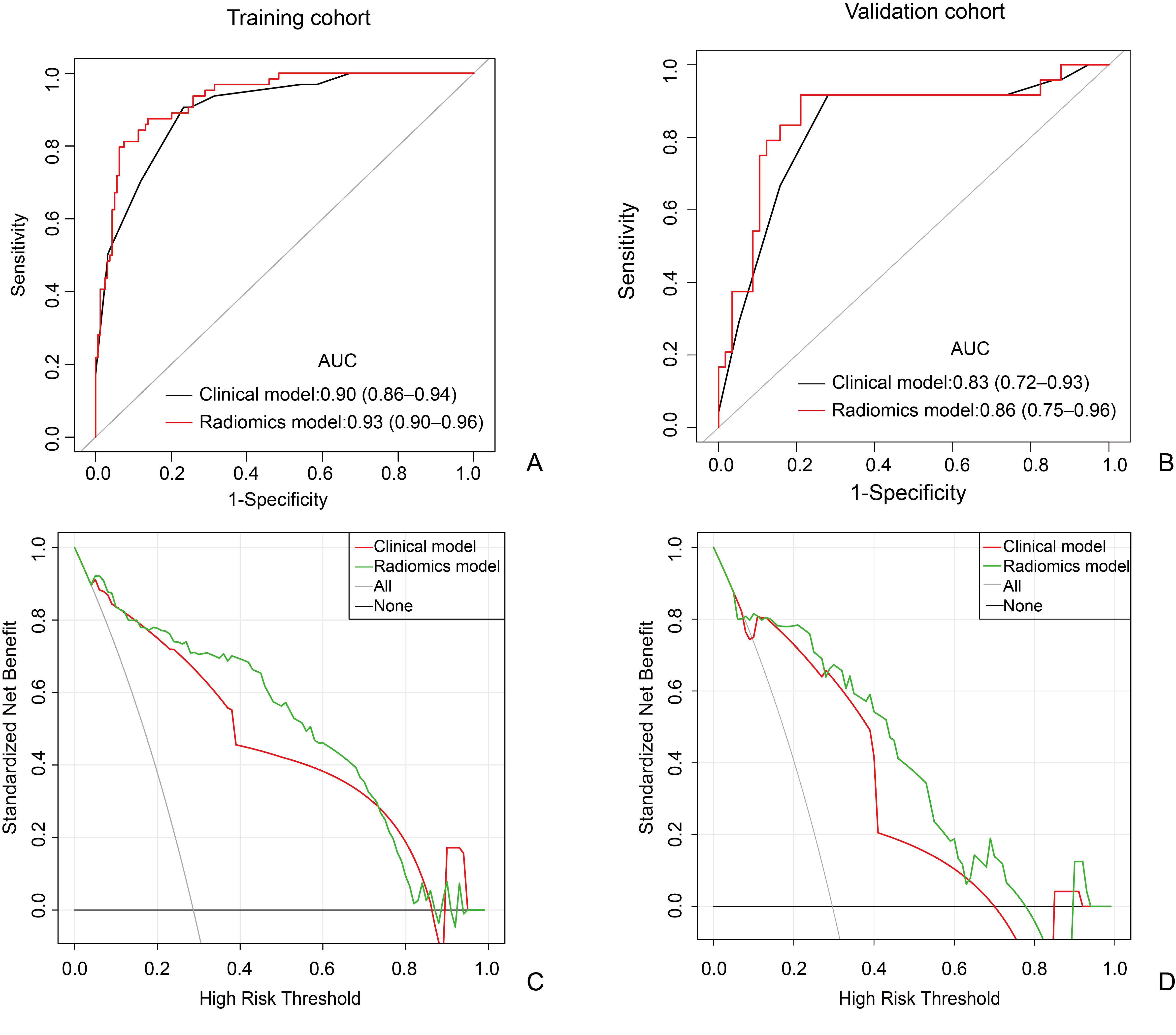
The sex, pancreatitis, location,tumor size, and tumor shape were selected for inclusion in the clinical model. The clinical model achieved an area under the curve (AUC) of 0.90 (95% CI 0.86–0.94) in the training cohort and 0.83 (95% CI 0.72–0.93) in the validation cohort. The sex, pancreatitis, location, tumor size, tumor shape, and T2WI radiomics score were selected for the radiomics model. The radiomics model achieved an AUC of 0.93 (95% CI 0.90–0.96) in the training cohort and 0.87 (95% CI 0.75–0.96) in the validation cohort. The radiomics model outperformed the clinical model. The decision curve analysis demonstrated that the radiomics nomogram was clinically useful.Conclusions
The T2WI radiomics nomogram can be used as a non-invasive and convenient tool for preoperatively predicting the presence of SCNs and MCNs. The tool has the potential to help clinicians identify patients requiring surveillance or surgery.Acknowledgements
NONEReferences
1. van Huijgevoort NCM, Del Chiaro M, Wolfgang CL, van Hooft JE, Besselink MG. Diagnosis and management of pancreatic cystic neoplasms: current evidence and guidelines. Nat Rev Gastroenterol Hepatol. 2019; 16(11):676-89.
2. European Study Group on Cystic Tumours of the P. European evidence-based guidelines on pancreatic cystic neoplasms. Gut. 2018; 67(5):789-804.
3. Tanaka M, Fernandez-Del Castillo C, Kamisawa T, et al. Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology. 2017; 17(5):738-53.
4. Mamone G, Barresi L, Tropea A, Di Piazza A, Miraglia R. MRI of mucinous pancreatic cystic lesions: a new updated morphological approach for the differential diagnosis. Updates Surg. 2020; 72(3):617-37.
5. Leung KK, Ross WA, Evans D, et al. Pancreatic cystic neoplasm: the role of cyst morphology, cyst fluid analysis, and expectant management. Ann Surg Oncol. 2009; 16(10):2818-24.
6. Thornton GD, McPhail MJ, Nayagam S, Hewitt MJ, Vlavianos P, Monahan KJ. Endoscopic ultrasound guided fine needle aspiration for the diagnosis of pancreatic cystic neoplasms: a meta-analysis. Pancreatology. 2013; 13(1):48-57.
7. Miller FH, Lopes Vendrami C, Recht HS, et al. Pancreatic Cystic Lesions and Malignancy: Assessment, Guidelines, and the Field Defect. Radiographics. 2022; 42(1):87-105.
8. Cheng SH, Liu D, Hou B, et al. PET-MR Imaging and MR Texture Analysis in the Diagnosis of Pancreatic Cysts: A Prospective Preliminary Study. Acad Radiol. 2020; 27(7):996-1005.
9. Wang BT, He L, Liu G, Liu MQ, Chen ZY. [Value of Magnetic Resonance Imaging Texture Feature Analysis in the Differential Diagnosis between Pancreatic Serous Cystadenoma and Mucinous Cystadenoma]. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2018; 40(2):187-93.
10. Moons KG, Altman DG, Reitsma JB, et al. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): explanation and elaboration. Ann Intern Med. 2015; 162(1):W1-73.
Figures