3630
Patients initially diagnosed with MR-visible Gleason 6 prostate cancer: can AI predict upgrade to clinically significant cancer at follow-up?1Body MRI, Stanford University, Palo Alto, CA, United States, 2Body MRI, Radiology, Stanford University, Palo Alto, CA, United States, 3Computational and Mathematical Engineering, Stanford University, Palo Alto, CA, United States, 4Imaging Informatics, Stanford University, Palo Alto, CA, United States, 5Radiology, Stanford University, Palo Alto, CA, United States
Synopsis
Keywords: Cancer, Prostate, rostate cancer diagnosis, Gleason score prediction, Magnetic Resonance Imaging (MRI), Convolutional Neural Networks (CNN), Pathological upgrading detection, Lesion characterization, Clinical significance determination, Artificial Intelligence (AI) in medical imaging, Precision medicine, Patient management, Predictive modeling in oncology, Diagnostic precision, Risk assessment in prostate cancer, Biopsy accuracy, Medical imaging technologies, Machine learning in healthcare
Motivation: Patients with low risk (Gleason 6) MR visible prostate cancer on initial biopsy are frequently upgraded to aggressive higher risk (Gleason 7 or higher) cancer. Identifying this progression early is difficult.
Goal(s): To address this using a neural network trained with radiologist labels and whole mount histology of Gleason ≥7 cases to predict pathological upgrading in our cohort.
Approach: DecNet was applied to the Gleason 6 initial MRIs to assess if the model could retrospectively identify patients with higher grade disease.
Results: Our model had a sensitivity of 84.6% for lesions upgraded to Gleason 7, outperforming PSA density, lesion size and ADC values.
Impact: These results showcase the potential of our model in unveiling higher-grade prostate cancer within lesions initially diagnosed as lower grade on pathology.
Background
Patients with low-risk prostate cancer are increasingly offered active surveillance, yet half of these patients progress to treatment during 10-year follow-up. Identifying those patients who will progress earlier in the course of their disease would allow for earlier treatment, reducing the risk of metastatic disease (1). In our cohort of patients with MR-visible lesions diagnosed after initial biopsy with low-risk Gleason 6, we found that within about two years more than half were upgraded to clinically significant (at least Gleason 7) disease at subsequent biopsy or prostatectomy. Initial PSA density, lesion size, and ADC value did not predict which patients were found to have clinically significant cancer at follow-up histopathology. To address this issue, we employed DecNet (2, 3), an internally developed convolutional neural network (CNN) designed to distinguish between clinically significant (Gleason score ≥7) and insignificant (Gleason score ≤6) cancer or normal tissue. We hypothesized that DecNet applied to the initial MRI could predict the patients from our cohort initially diagnosed with MRI-visible Gleason 6 cancer that were found to have clinically significant prostate cancer at follow-up.Materials and Methods
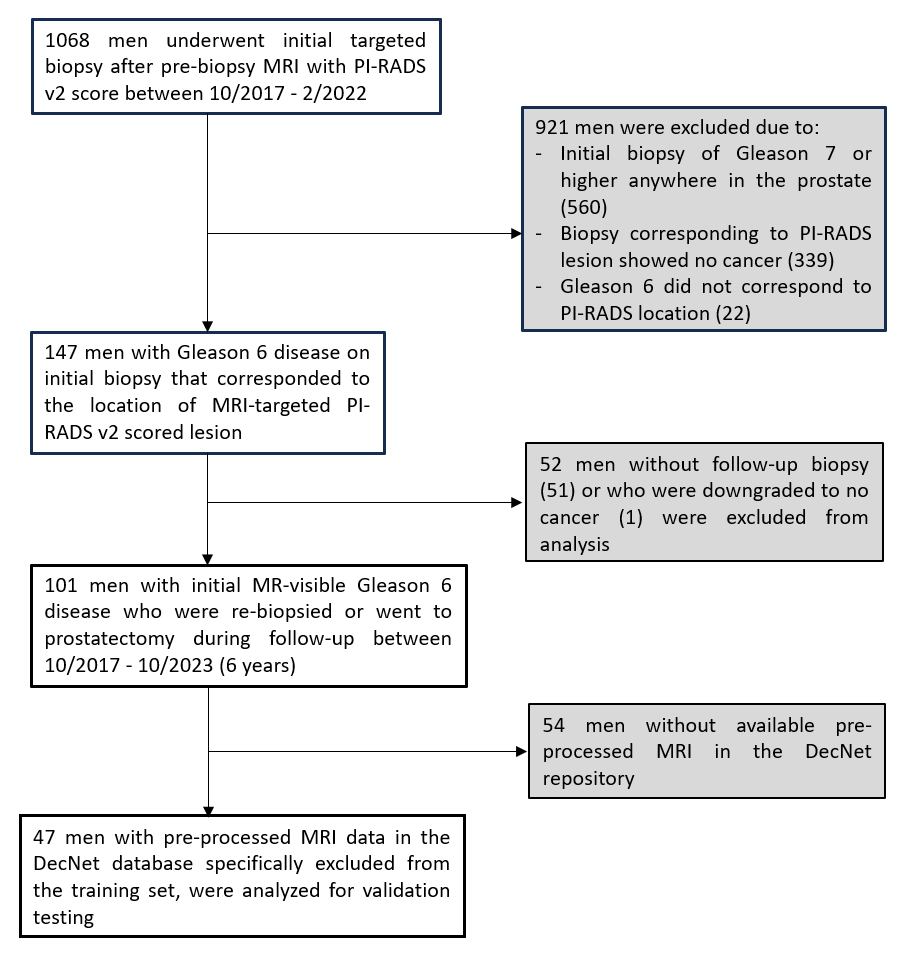
In this single-center study, we retrospectively identified a patient cohort of 101 men between October 2017 and February 2022 who underwent initial MRI-targeted and systematic biopsy utilizing a transrectal MR-US fusion biopsy system. The cohort included men with MRI visible PI-RADS v2 3, 4, 5 lesions originally biopsied as Gleason 6 who then had follow up biopsy or prostatectomy. This was further narrowed to 47 patients for whom we had pre-processed MRI information in our neural network model repository [Decision Network (DecNet)] (Figure 1). DecNet was trained with n= 2060 MRI-US fusion targeted biopsy scans, and was trained and validated with radiologist labels (PIRADS >=3) and biopsy histopathology (2). The study was conducted with institutional review board approval and informed consent waiver, following institutional guidelines for data collection, storage, and analysis.Results
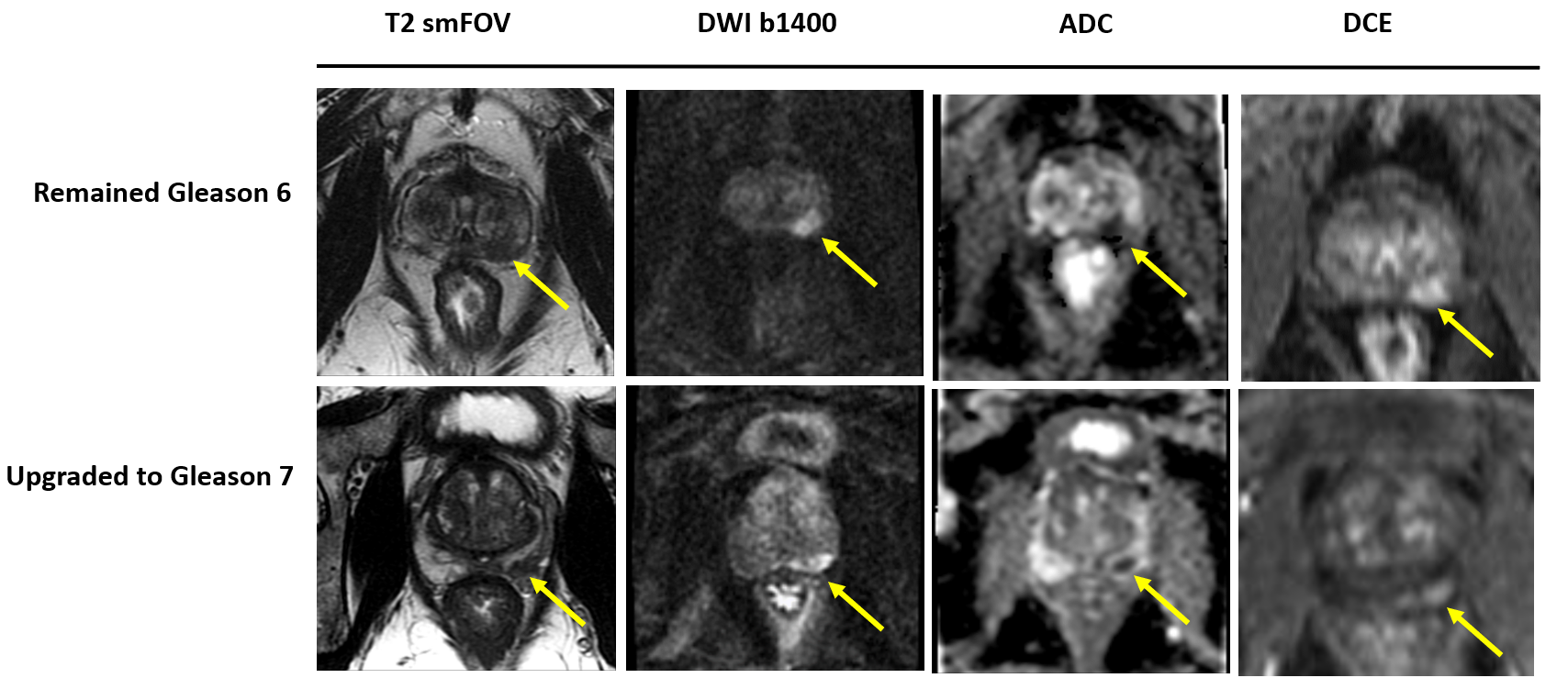
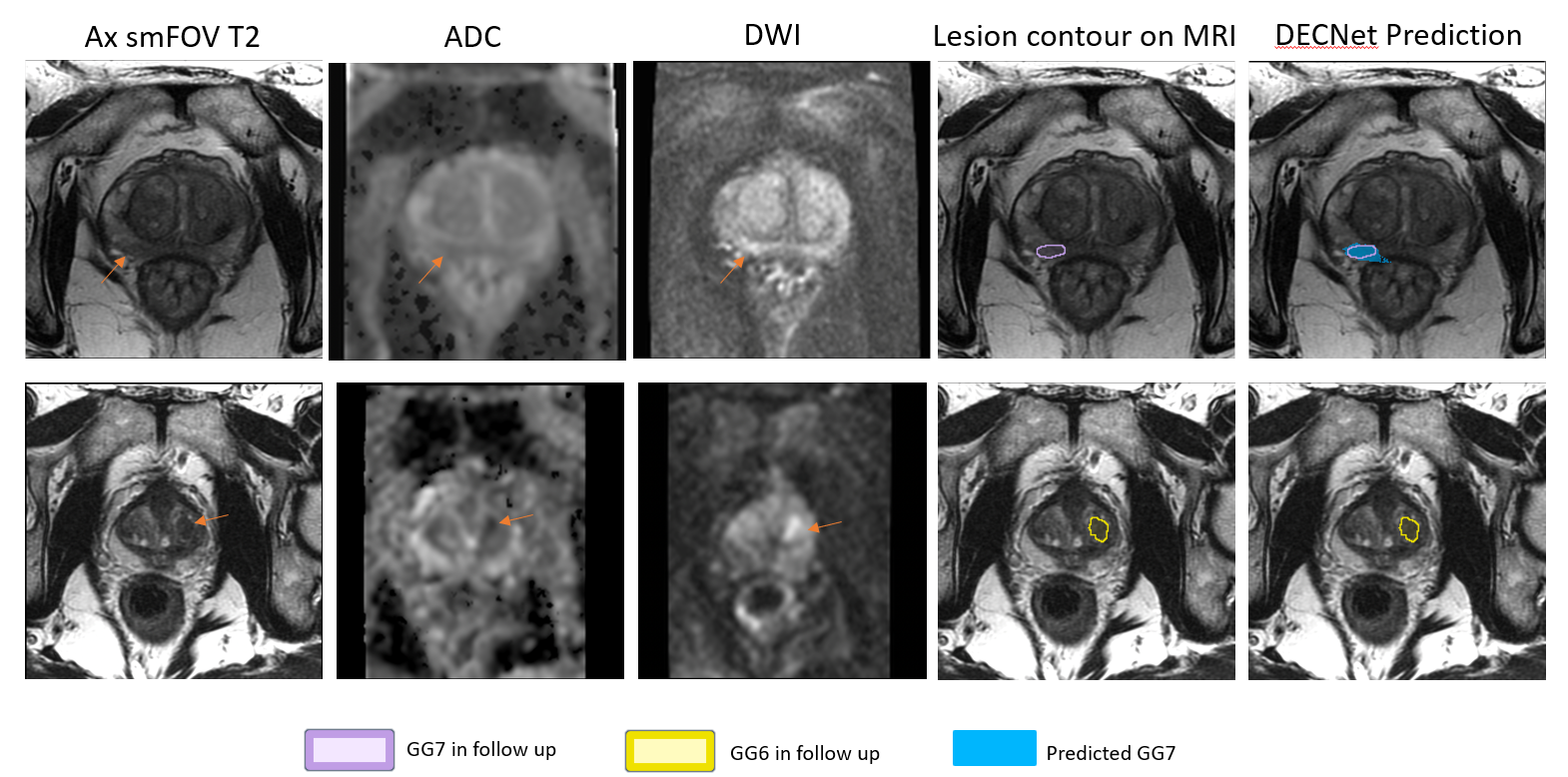
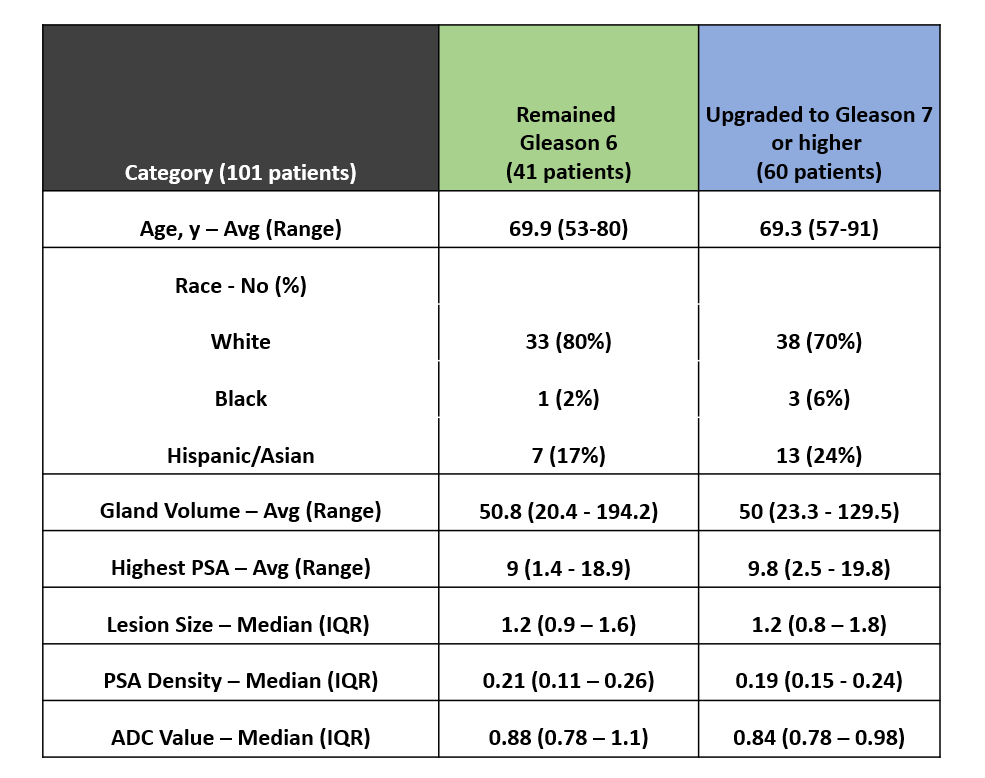
47 patients (median age: 67.5 years, [range 49-91 years]) with 63 PIRADS 3-5 lesions biopsy-proven to be Gleason 6 cancer were included (Figure 2). On a patient-level basis, DecNet had an aggregate sensitivity of 84.6% [95% CI: 0.83-0.94] for all lesions that were upgraded to Gleason 7 on follow up pathology and a combined specificity of 48% [95% CI: 0.28-0.68] for Gleason 6 lesions that remained Gleason 6 (Figure 3). The positive predictive value of our model was calculated at 67% [95% CI: 0.50-0.80]; and the negative predictive value was calculated at 71.4% [95% CI: 0.45-0.88]. This performance surpassed the statistically insignificant differences observed in the PSA density [p=0.704, Wilcoxon rank sum test], lesion size [p =0.962] and ADC value [p = 0.19] between the two sets (Table 1).Discussion
Utilizing the initial prostate MRI, DecNet demonstrated a relatively high sensitivity of 84.6% [95% CI: 0.83-0.94] for detecting clinically significant higher-grade cancer in patients initially diagnosed with Gleason 6 cancer by MR-targeted and systematic biopsy and subsequently confirmed to have at least Gleason 7 cancer during follow-up.Conclusion
Our models show the promise of utilizing CNN in unmasking underlying higher grade prostate cancer (Gleason 7 and above) in MRI visible lesions initially biopsy proven to be Gleason 6 prostate cancer. Additional studies with a more extensive patient cohort should be conducted to confirm these preliminary findings.Once further validated in larger studies, this AI tool could be used to identify patients with clinically significant disease, which would allow for closer monitoring or earlier intervention of patients suspected to harbor higher grade disease.
Acknowledgements
No acknowledgement found.References
- Hamdy, Freddie C., Jenny L. Donovan, J. Athene Lane, Malcolm Mason, Chris Metcalfe, Peter Holding, Michael Davis, et al. “10-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Localized Prostate Cancer.” New England Journal of Medicine 375, no. 15 (October 13, 2016): 1415–24. https://doi.org/10.1056/NEJMoa1606220.
- Li, Cynthia Xinran, Indrani Bhattacharya, Sulaiman Vesal, Sara Saunders, Simon John Christoph Soerensen, Richard E. Fan, Geoffrey A. Sonn, and Mirabela Rusu. “Improving Automated Prostate Cancer Detection and Classification Accuracy with Multi-Scale Cancer Information.” In Machine Learning in Medical Imaging, edited by Xiaohuan Cao, Xuanang Xu, Islem Rekik, Zhiming Cui, and Xi Ouyang, 341–50. Lecture Notes in Computer Science. Cham: Springer Nature Switzerland, 2024. https://doi.org/10.1007/978-3-031-45673-2_34.
- Seetharaman, Arun, Indrani Bhattacharya, Leo C. Chen, Christian A. Kunder, Wei Shao, Simon J. C. Soerensen, Jeffrey B. Wang, et al. “Automated Detection of Aggressive and Indolent Prostate Cancer on Magnetic Resonance Imaging.” Medical Physics 48, no. 6 (June 2021): 2960–72. https://doi.org/10.1002/mp.14855.
Figures