3629
Tailored Prostate MRI Screening: A Deep Learning Classifier for Intelligent Scanning1Bernard and Irene Schwartz Center for Biomedical Imaging, Department of Radiology, New York University Grossman School of Medicine, NYC, NY, United States, 2Siemens Healthineers, Digital Technology & Innovation, Princeton, NJ, United States, 3Center for Advanced Imaging Innovation and Research (CAI2R), Department of Radiology, New York University Grossman School of Medicine, NYC, NY, United States, 4Courant Institute of Mathematical Sciences, New York University, NYC, NY, United States
Synopsis
Keywords: Prostate, Prostate
Motivation: Multiparametric prostate MRI is lengthy and costly, presenting a challenge for widespread implementation.
Goal(s): To develop an automated triage protocol using a deep learning classifier to discern, based on an abbreviated biparametric MR examination, between high-risk patients who would benefit from additional sequences and low-risk patients who would not.
Approach: A double-branched ResNet50 with 3D convolutions was trained on biparametric scans to predict the presence of clinically significant prostate cancer.
Results: The classifier achieved a sensitivity of 0.93 with 88% negative predictive value, indicating potential to reduce comprehensive MRI exams for those without clinically significant disease by 40%.
Impact: Our triage protocol has the potential to streamline prostate cancer screening by reducing the number of full mpMRI exams, thereby lowering healthcare costs. The classifier could pave the way for personalized, risk-adaptive screening protocols, allowing more precise and resource-efficient diagnostics.
Introduction
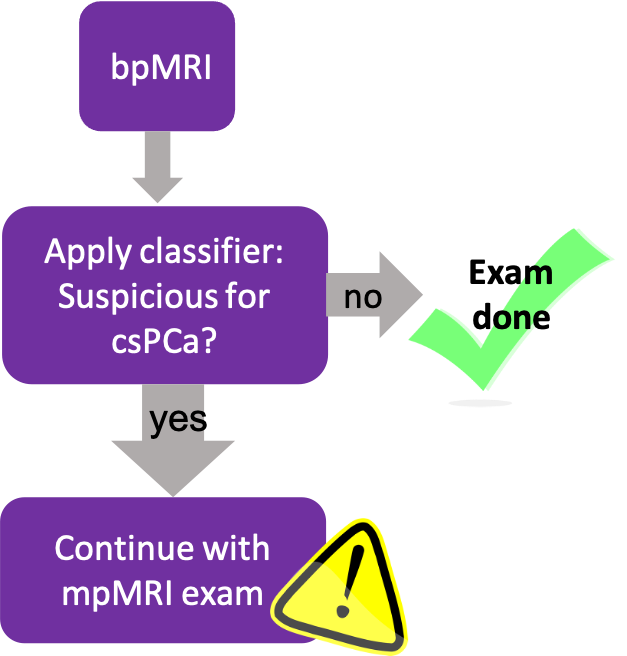
Prostate cancer (PCa) is the most prevalent cancer among men in the US, presenting a significant disease burden[1]. In the last decade, MRI's role in detecting and localizing clinically significant PCa (csPCa) has expanded considerably[2,3]. A direct comparison study between MRI and the prostate specific antigen (PSA) blood test for population-level screening demonstrated that MRI identified more csPCa and fewer non-clinically significant cases[4]. This underscores MRI's potential as a superior primary screening tool. However, its broader adoption faces challenges related to cost and accessibility. Current prostate MRI exams use a 'one-size-fits-all' approach, involving numerous sequences for PCa detection, staging, and biopsy guidance. A considerable portion of the MRI exam only proves valuable (for localization and staging) when a clinically significant lesion is present. We propose an abbreviated protocol for patients in whom initial sequences indicate a low risk of csPCa. By training a deep learning (DL) classifier on bi-parametric prostate MRI (bpMRI), which includes only T2-weighted (T2WI) and diffusion-weighted imaging (DWI) and excludes dynamic contrast-enhanced (DCE) imaging, we aim to predict positive (PIRADS ≥ 3) or negative results. Once trained, this classifier can be incorporated into a bpMRI screening protocol, as illustrated in Figure 1. Our novel dual-tiered strategy tailors the MRI protocol to individual patient risk in real-time, ensuring that those without significant lesions bypass lengthy exams and potential risks of gadolinium contrast administration. Such an approach will become increasingly important as prostate MRI becomes more prevalent for screening and both the volume of exams and the rate of negative cases increases.Methods
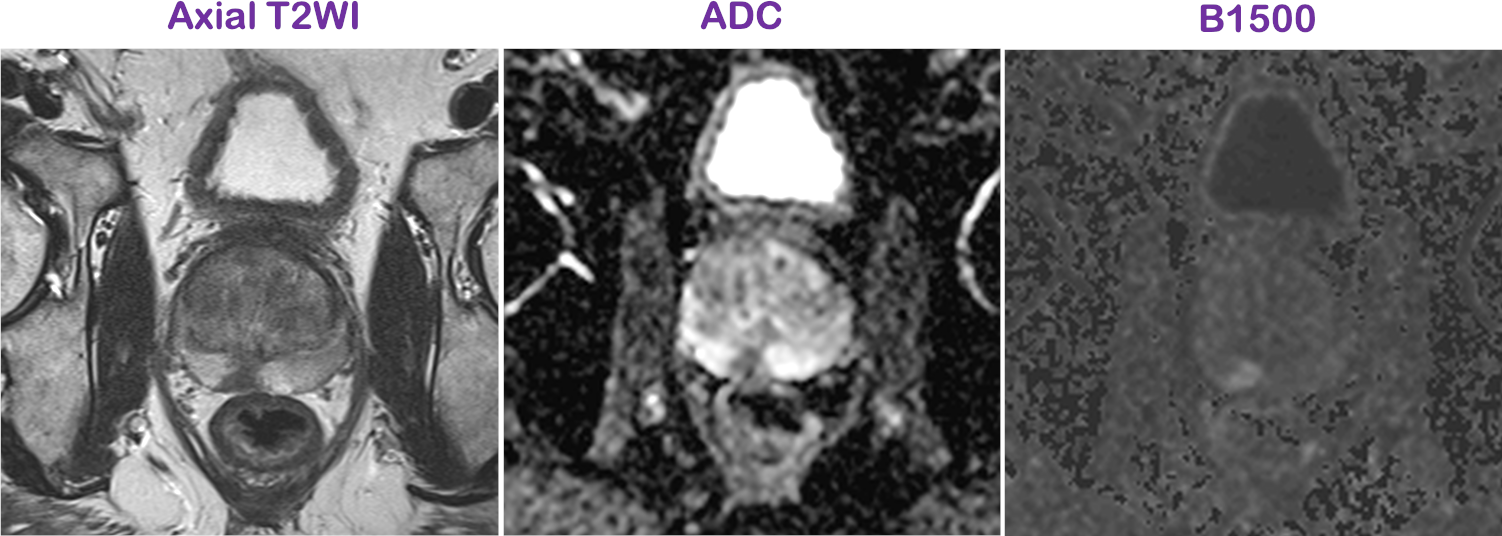
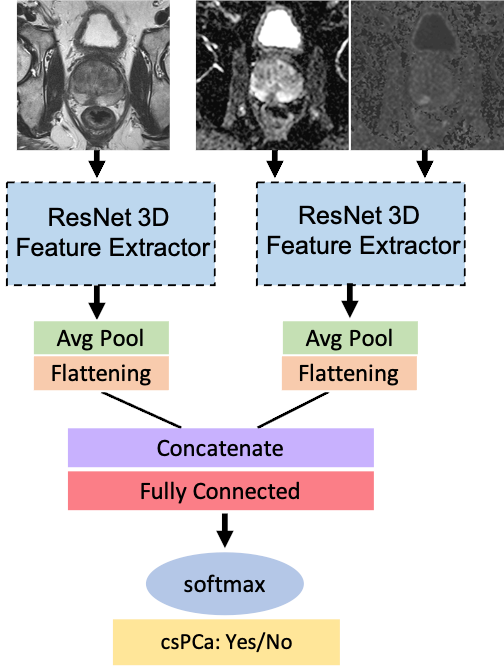
Data: This retrospective study utilized a dataset of bpMRI, consisting of T2WI and DWI. The training dataset comprised images from 6924 patients scanned between January 2019 and February 2021, the validation set 363 patients from March 1st to March 30th 2021, and the test set 343 patients between April 1st and April 30th 2021. These patients were referred for clinical prostate MRI due to known or suspected PCa. Binary labels for csPCa were derived from PIRADS scores assigned to each exam by one of five experienced radiologists who have interpreted over 3000 Prostate MRI exams. The PIRADS scoring system is shown in Table 1. Suspicious csPCa is defined as PIRADS ≥ 3. Two computed images were derived from the primary DWI protocol: Apparent Diffusion Coefficient (ADC) and B1500. These images, along with the axial T2WI, serve as the input to the classifier. An example set of images is shown in Figure 2.DL model architecture and training: The model architecture is a double-branched ResNet50 with 3D convolutions to accommodate multiple image resolutions and fields of view [5]. Features are learned from T2WI and separately from ADC and B1500. The learned features are concatenated prior to the classification head (fully-connected layer). This architecture is illustrated in Figure 3. It has ~92 million learnable parameters and was trained with the ADAM optimizer and cross entropy loss. This model predicts a radiologist’s binary interpretation of Prostate MRI exams. The operating point was manually determined on the validation set.
Evaluation: On our test set of 343 cases, we evaluated the model using an AUC-ROC analysis. The confusion matrix was calculated at the pre-determined operating point.
Results
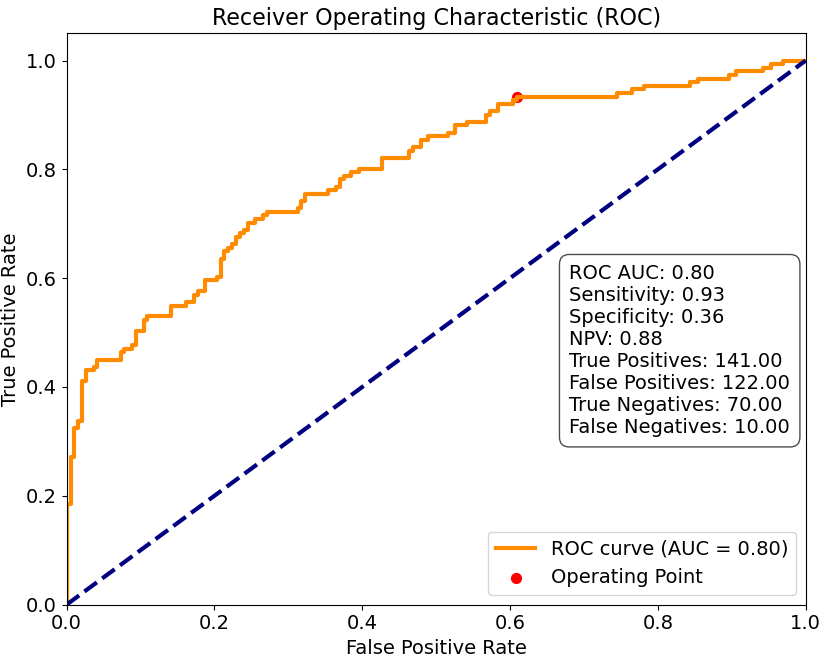
The ROC curve is shown in Figure 4, along with the classification performance at the selected operating point. The operating point was selected to prioritize negative predictive value (NPV), with sensitivity of 0.93 and specificity of 0.36. The calculated AUC on the test set was 0.80 (with validation AUC of 0.75). The NPV is 88% and the fraction of total patients classified as negative is 23.3% (i.e., 23.3 of 100 subjects would not need the full mpMRI exam).Discussion/Conclusion
Our study's findings are promising in the context of screening efficiency. They also indicate a need for further refinement of the classifier. The high sensitivity is encouraging; however, we observe a higher than ideal rate of false negatives and a modest reduction in the total number of comprehensive MRI exams. It is critical to achieve a balance where the NPV is high (e.g., above 95%) to detect most clinically significant prostate cancers, while the number of false positives is substantially reduced. This balance is necessary to enhance the clinical viability of the abbreviated protocol, minimize patient risk, and maximize the utility of MRI as a screening tool. Future efforts will focus on optimizing the NPV of the deep learning model to achieve this goal.Disclaimer
The concepts and information presented in this paper/presentation are based on research results that are not commercially available. Future commercial availability cannot be guaranteed.Acknowledgements
No acknowledgement found.References
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72: 7–33.
- Fascelli M, George AK, Frye T, Turkbey B, Choyke PL, Pinto PA. The role of MRI in active surveillance for prostate cancer. Curr Urol Rep. 2015;16. doi:10.1007/s11934-015-0507-9
- Brown LC, Ahmed HU, Faria R, El-Shater Bosaily A, Gabe R, Kaplan RS, et al. Multiparametric MRI to improve detection of prostate cancer compared with transrectal ultrasound-guided prostate biopsy alone: the PROMIS study. Health Technol Assess . 2018;22. doi:10.3310/hta22390
- Moore CM, Frangou E, McCartan N, Santaolalla A, Kopcke D, Brembilla G, et al. Prevalence of MRI lesions in men responding to a GP-led invitation for a prostate health check: a prospective cohort study. BMJ Oncology. 2023;2: e000057.
- Sihong Chen and Kai Ma and Yefeng Zheng . Med3D: Transfer Learning for 3D Medical Image Analysis. arXiv, 17 July 2019. arXiv.org, doi.org/10.48550/arXiv.1904.00625.
Figures