3628
Deep learning reconstructed fast non-Gaussian DWI for predicting microsatellite instability in esophagogastric junction adenocarcinoma1Department of Diagnostic Radiology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2GE Healthcare, MR Research China, Beijing, China
Synopsis
Keywords: Digestive, Diffusion/other diffusion imaging techniques
Motivation: Microsatellite instability (MSI) in esophagogastric junction adenocarcinoma (EGA) can serve as a predictor of sensitivity to immunotherapy and affect the prognosis. Predicting MSI preoperatively can enable personalized and precise treatment for EGA patients.
Goal(s): This study investigates the use of fast non-Gaussian diffusion-weighted imaging with deep learning-based reconstruction (DLRecon) to assess MSI in EGA.
Approach: We compared image quality between conventional scanning (CS) and DLRecon, calculated diffusion parameters, and assessed their ability to distinguish MSI status.
Results: DLRecon exhibited superior image quality and reduced scan time. Diffusion parameters effectively differentiated MSI status in EGA.
Impact: DLRecon non-Gaussian DWI significantly improved image quality and reduced acquisition time. Multiple diffusion parameters may serve as imaging markers, and their combination provides high diagnostic accuracy for discriminating MSI status in EGA.
Introduction
Microsatellite instability (MSI) is a special subtype of esophagogastric junction adenocarcinoma (EGA) with favorable survival outcomes compared to microsatellite stable (MSS) tumors [1-4]. MSI detection relies on the patient’s pathological specimens [5]. Thus, it is useful to explore a non-invasive method to discriminate MSI status of EGAs. Compared with traditional DWI [6], non-Gaussian DWI models such as intravoxel incoherent motion (IVIM) [7] and diffusion kurtosis imaging (DKI) [8] can more accurately reflect water diffusion restricted by microstructures in living tissue. However, the utilization of non-Gaussian DWI is limited due to its long scanning time. Recently, deep learning-based reconstruction (DLRecon) could potentially improve image quality and reduce acquisition time [9-11]. Therefore, we aim to assess the image quality and investigate the feasibility of fast non-Gaussian diffusion-weighted imaging with DLRecon for predicting MSI status in EGA in comparison with conventional scan (CS).Methods
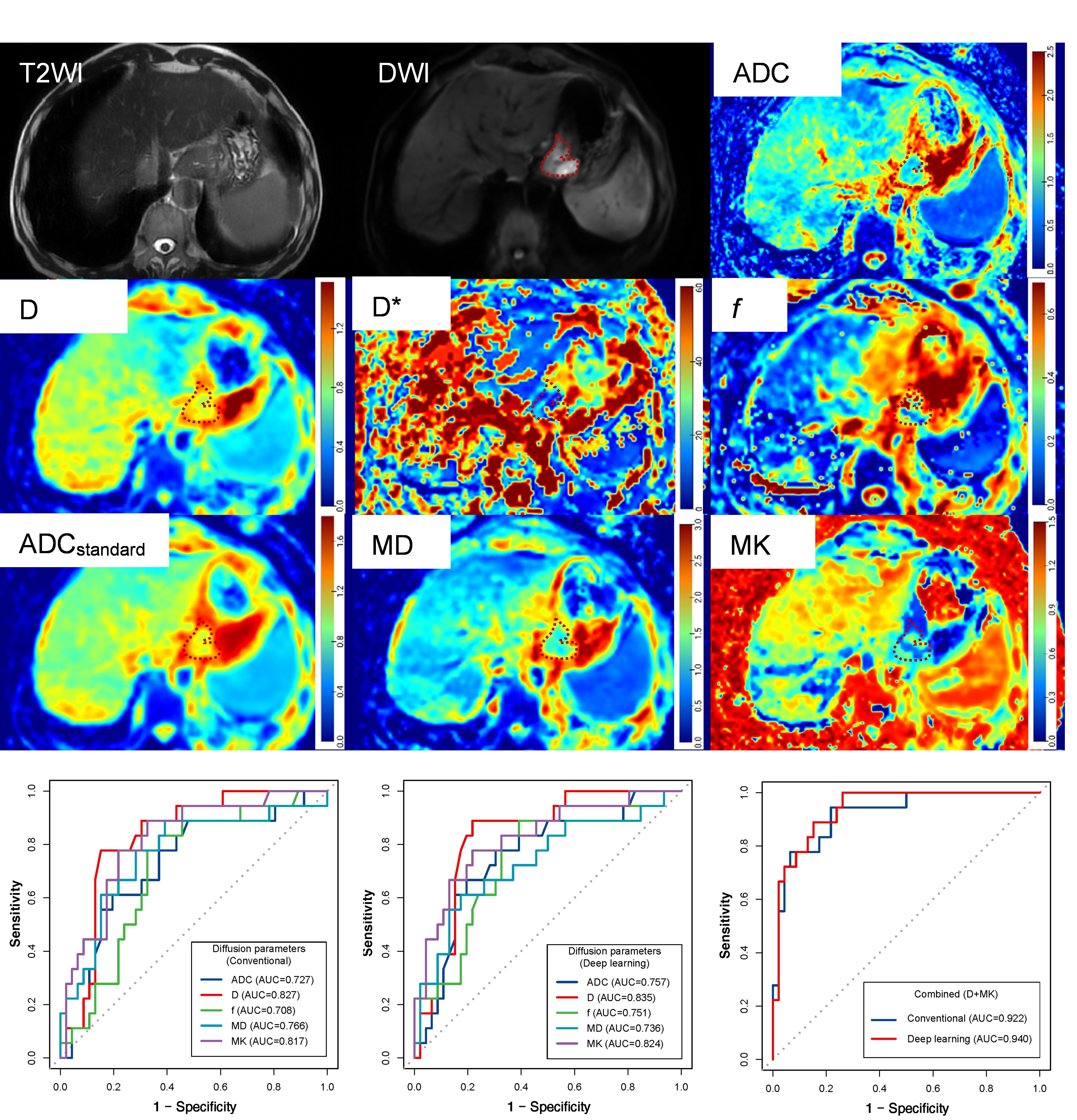
A total of 65 patients with locally advanced EGA were prospectively recruited in this study. All MRI was acquired using a 3.0-Tesla scanner (SIGNATM Architect, GE Healthcare, USA). The DWI of standard CS and DLRecon with a reduced number of excitations (NEX) were acquired using at thirteen different b-values: 0 (2/1), 10 (2/1), 20 (2/1), 50 (2/1),100 (2/1), 150 (2/1), 200 (2/1), 400 (4/2), 600 (4/2), 800 (4/2), 1000 (6/3), 1200 (6/3), 1500 (6/3) s/mm2 (the numbers in parentheses are represented as NEX in CS and DLRecon). Subjective image quality, signal-to-noise ratio (SNR) and contrast to-noise ratio (CNR) were evaluated. Diffusion-derived metrics, including apparent diffusion coefficient (ADC), true diffusion coefficient (D), pseudo-diffusion coefficient (D*), perfusion fraction (f), mean diffusivity (MD) and mean kurtosis (MK) were obtained. Wilcoxon signed-rank tests or Mann-Whitney U test was used as appropriate. The diagnostic efficacy for predicting MSI status of EGA was determined by ROC analysis.Results
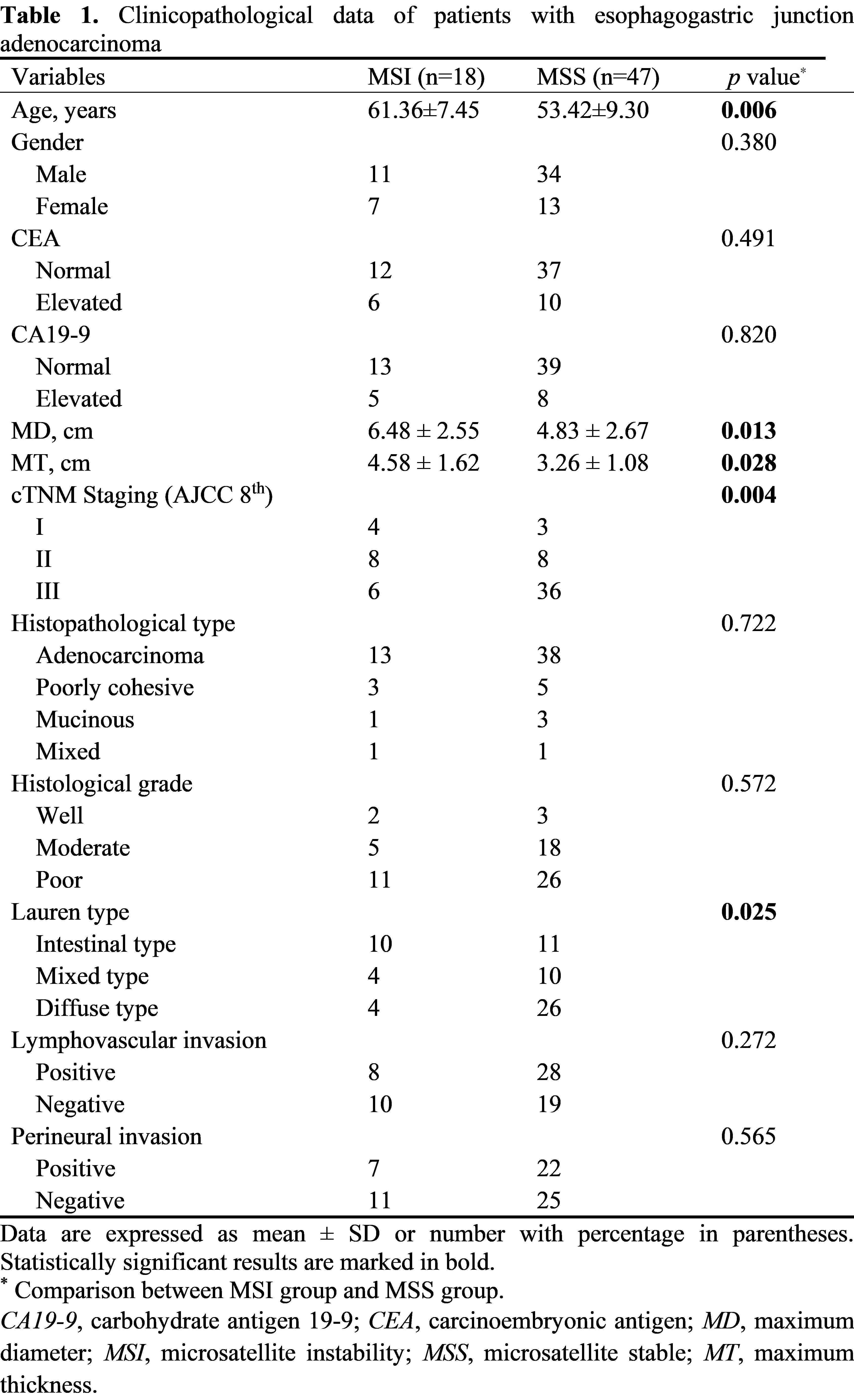
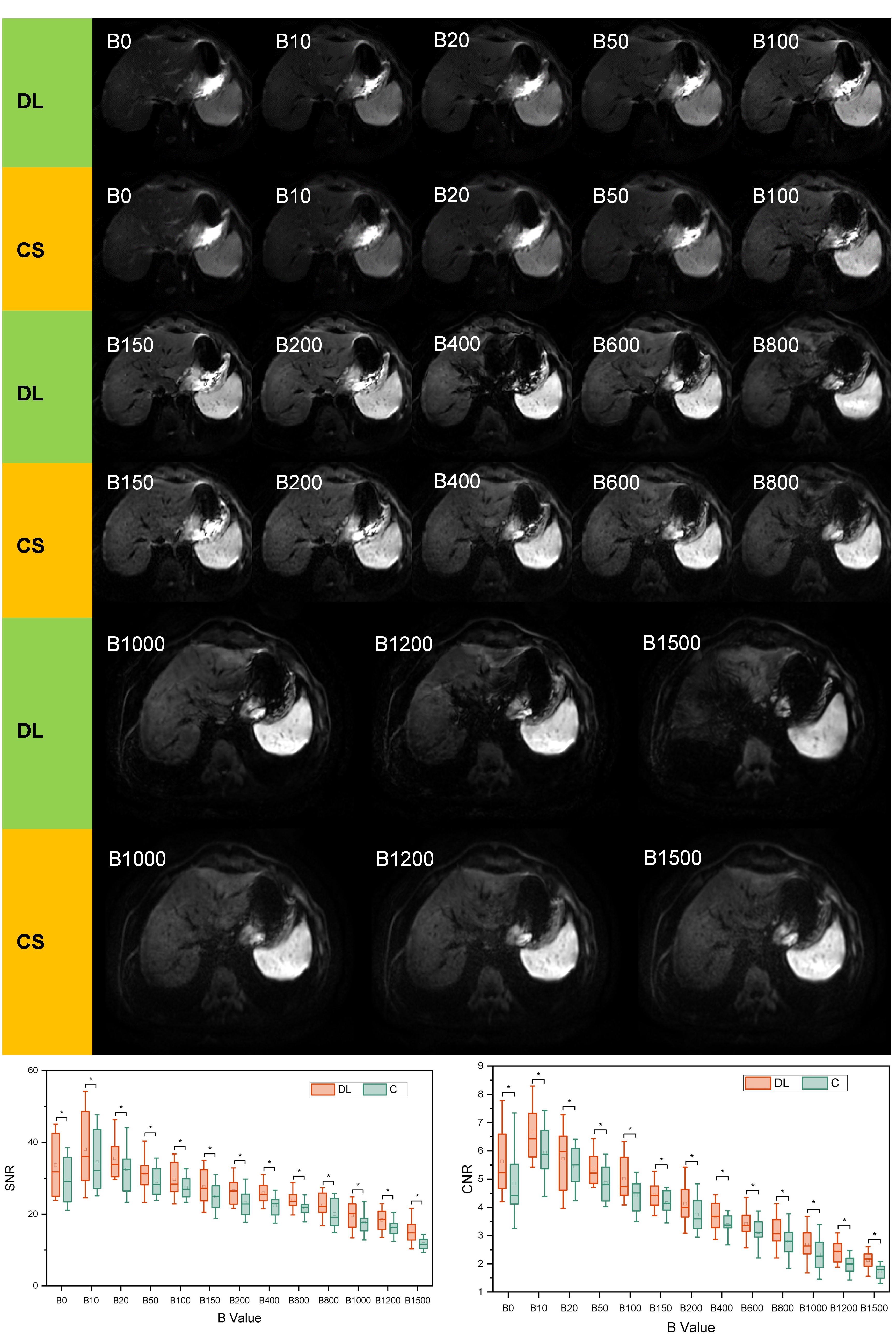
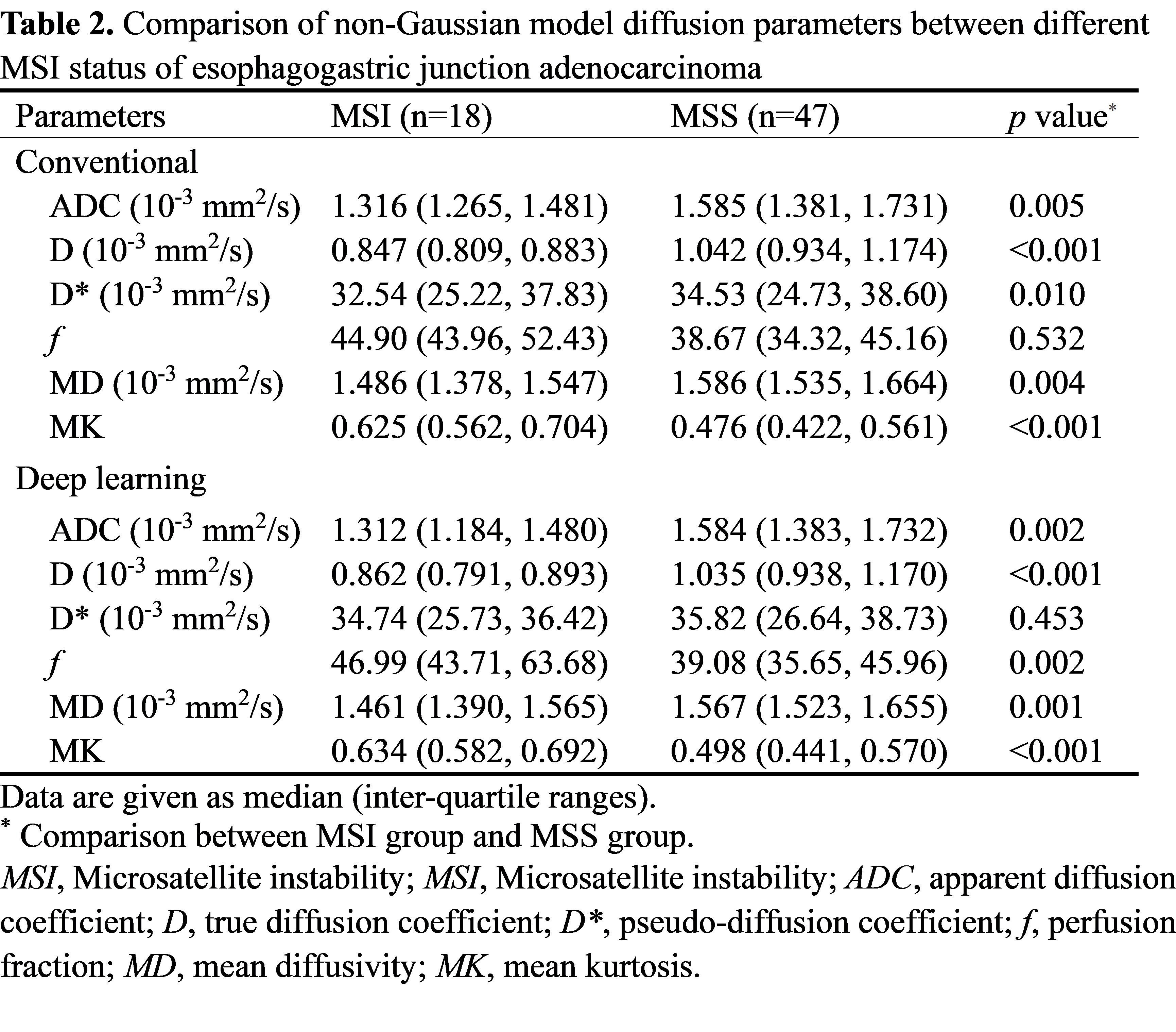
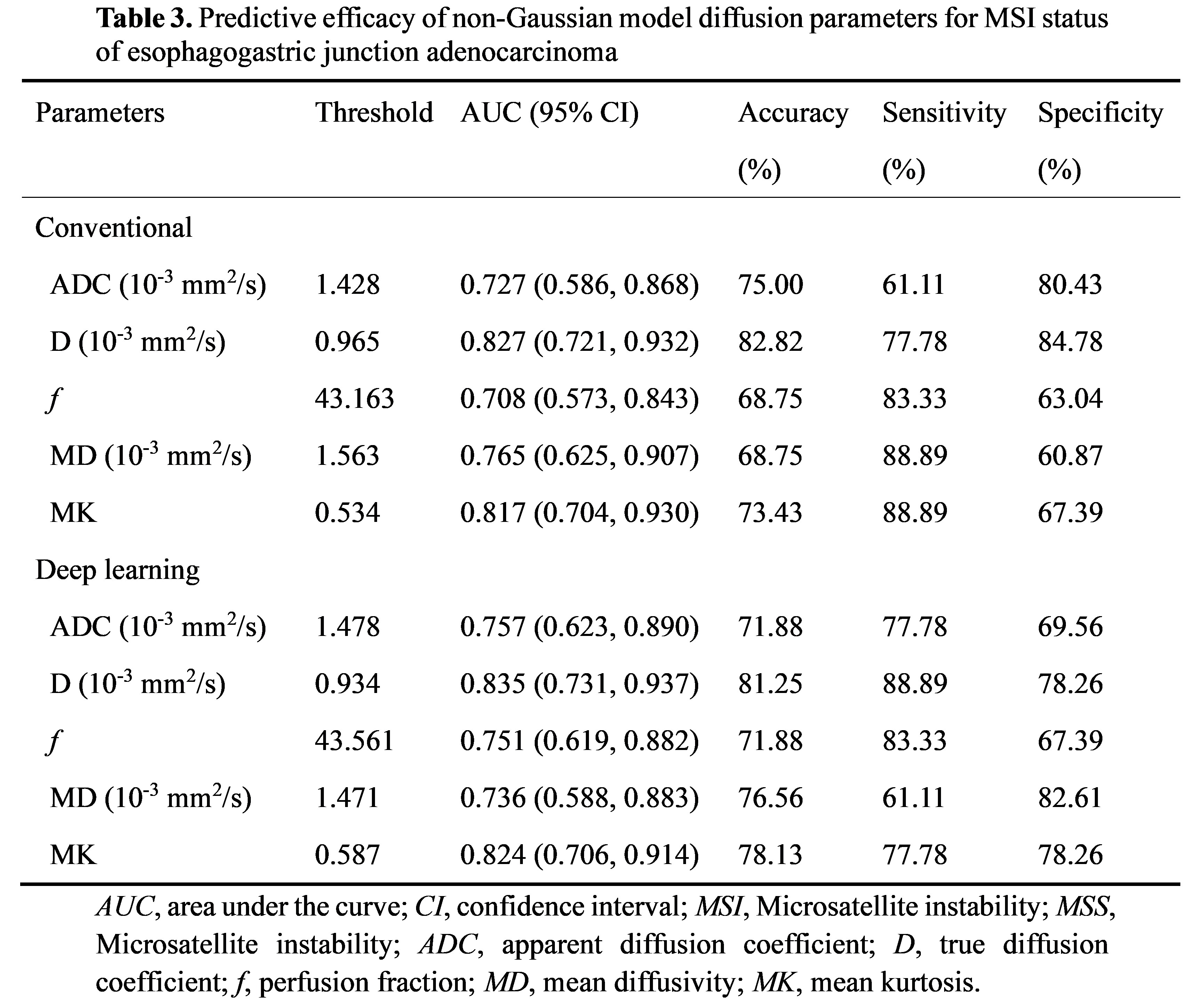
A total of 65 patients were finally enrolled in this study. 18 patients were pathologically confirmed with MSI EGA. The patients’ clinical data are shown in Table 1. Age, maximum diameter, maximum thickness, clinical TNM staging, and Lauren type showed a significant difference between MSI and MSS EGA. The mean acquisition time for the DLRecon (116.25 ± 29.23 sec) was significantly shorter (p < 0.001) than for CS (266.48 ± 45.82 sec). The DLRecon produced higher subjective imaging quality, SNR and CNR in all b values than CS (p < 0.05) (Figure 1). There was no significant difference between DLRecon and CS for all the diffusion parameters. As shown in Table 2, both in DLRecon and CS sequences, the ADC, D, f, MD, and MK values showed significant difference between of MSI group and MSS group (all p < 0.05); and the D* value was not statistically different. Table 3 and Figure 2 show the performance of the parameters ADC, D, f, MD, and MK for differentiating MSI status in EGA. The D value using DLRecon had the highest AUC (0.835) for a single parameter value. Combining D and MK resulted an AUC (0.940) that was statistically significantly greater than any parameters alone (Delong test, p < 0.05).Discussion
DLRecon can improve image quality by both mitigating artifacts and image noise while accelerating acquisition [9-12]. Our study investigated the impact of DLRecon non-Gaussian DWI acquisition method on acquisition time, image quality, and diagnostic performance for MSI in EGA compared with conventional acquisition method. DLRecon acquisition method enabled an approximately 50% reduction in examination time. Our results reveal that the novel DLRecon method produced better overall image quality, higher SNR and CNR than CS method. Furthermore, the diffusion parameters showed no significant difference between two acquisition method. As for discriminating MSI in EGA, we also demonstrated that ADC, D, and MD values of the MSI group were lower than those of the MSS group. This result may be due to the increase in local cell density due to lymphocyte infiltration in MSI EGA and the reduction of intercellular space [13], which restricts the free diffusion of water molecules. In this study, the f value of the MSI group was observed to be higher than those of the MSS group. We speculated that elevated microvessel density and blood flow velocity might contribute to the increase perfusion of MSI tumor. We also found that MK was higher in MSI group. This might be caused by the high mutational burden and tumor heterogeneity [14].Conclusion
DLRecon non-Gaussian DWI provided excellent image quality with a significant reduction in examination time by 50%. Non‑Gaussian diffusion parameters from DLRecon method was shown to be clinically feasible and interchangeable with standard conventional acquisition for discriminating MSI status in EGA.Acknowledgements
None.References
[1] Hölscher AH, Law S. Esophagogastric junction adenocarcinomas: individualization of resection with special considerations for Siewert type II, and Nishi types EG, E=G and GE cancers. Gastric Cancer. 2020;23(1):3-9.
[2] Kumamoto T, Kurahashi Y, Niwa H, Nakanishi Y, Okumura K, Ozawa R, et al. True esophagogastric junction adenocarcinoma: background of its definition and current surgical trends. Surg Today. 2020;50(8):809-814.
[3] Palmeri M, Mehnert J, Silk AW, Jabbour SK, Ganesan S, Popli P, et al. Real-world application of tumor mutational burden-high (TMB-high) and microsatellite instability (MSI) confirms their utility as immunotherapy biomarkers. ESMO Open. 2022;7(1):100336.
[4] van Velzen MJM, Derks S, van Grieken NCT, Haj Mohammad N, van Laarhoven HWM. MSI as a predictive factor for treatment outcome of gastroesophageal adenocarcinoma. Cancer Treat Rev. 2020;86:102024.
[5] Yang G, Zheng RY, Jin ZS. Correlations between microsatellite instability and the biological behaviour of tumours. J Cancer Res Clin Oncol. 2019;145(12):2891-2899.
[6] Ajani JA, D'Amico TA, Bentrem DJ, Chao J, Cooke D, Corvera C, et al. Gastric Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2022;20(2):167-192.
[7] Liu S, Guan W, Wang H, Pan L, Zhou Z, Yu H, et al. Apparent diffusion coefficient value of gastric cancer by diffusion-weighted imaging: correlations with the histological differentiation and Lauren classification. Eur J Radiol. 2014;83(12):2122-2128.
[8] Jiang Y, Chen YL, Chen TW, Wu L, Ou J, Li R, et al. Is there association of gross tumor volume of adenocarcinoma of oesophagogastric junction measured on magnetic resonance imaging with N stage? Eur J Radiol. 2019;110:181-186.
[9] Le Bihan D. Apparent diffusion coefficient and beyond: what diffusion MR imaging can tell us about tissue structure. Radiology. 2013;268(2):318-22.
[10] Li J, Yan LL, Zhang HK, Wang Y, Xu SN, Chen XJ, et al. Application of intravoxel incoherent motion diffusion-weighted imaging for preoperative knowledge of lymphovascular invasion in gastric cancer: a prospective study. Abdom Radiol (NY). 2023;48(7):2207-2218.
[11] Yuan L, Lin X, Zhao P, Ma H, Duan S, Sun S. Correlations between DKI and DWI with Ki-67 in gastric adenocarcinoma. Acta Radiol. 2023;64(5):1792-1798.
[12] Hallinan JTPD. Deep Learning for Spine MRI: Reducing Time Not Quality. Radiology. 2023;306(3):e222410.
[13] Almansour H, Herrmann J, Gassenmaier S, Afat S, Jacoby J, Koerzdoerfer G, et al. Deep Learning Reconstruction for Accelerated Spine MRI: Prospective Analysis of Interchangeability. Radiology. 2023;306(3):e212922.
[14] Chen Q, Fang S, Yuchen Y, Li R, Deng R, Chen Y, Ma D, Lin H, Yan F. Clinical feasibility of deep learning reconstruction in liver diffusion-weighted imaging: Improvement of image quality and impact on apparent diffusion coefficient value. Eur J Radiol. 2023;168:111149.
[15] Afat S, Herrmann J, Almansour H, Benkert T, Weiland E, Hölldobler T, et al. Acquisition time reduction of diffusion-weighted liver imaging using deep learning image reconstruction. Diagn Interv Imaging. 2023;104(4):178-184.
[16] Shin SJ, Kim SY, Choi YY, Son T, Cheong JH, Hyung WJ, et al. Mismatch Repair Status of Gastric Cancer and Its Association with the Local and Systemic Immune Response. Oncologist. 2019 Sep;24(9):e835-e844. [17] Wu H, Ma W, Jiang C, Li N, Xu X, Ding Y, et al. Heterogeneity and Adjuvant Therapeutic Approaches in MSI-H/dMMR Resectable Gastric Cancer: Emerging Trends in Immunotherapy. Ann Surg Oncol. 2023 Sep 4. doi: 10.1245/s10434-023-14103-0. Epub ahead of print.
Figures