3625
Automatic detection of Small Hepatocellular Carcinoma (<= 2 cm) in cirrhotic liver based on Gd-EOB-DTPA-enhanced MRI using deep learning1Radiology, First Hospital of LanZhou University, lanzhou, China, 2Philips Healthcare, Xi'an, China, 3Philips Healthcare, Beijing, China
Synopsis
Keywords: Diagnosis/Prediction, Liver, deep learning,small hepatocellular carcinomas,Dysplastic Nodule
Motivation: In light of the overlapping image features between small hepatocellular carcinoma (sHCC) and benign precancerous nodules, the detection of sHCC from cirrhosis liver is deemed difficult and challenging.
Goal(s): To develop a fully automatic deep learning approach for the detection of sHCC in cirrhotic livers, utilizing Gd-EOB-DTPA-enhanced MRI.
Approach: A 3D nnU-Net deep learning network was trained to perform automatic segmentation and detection of sHCC lesions.
Results: 120 patients were included. The AUCs for discriminating between sHCC lesions and non-sHCC lesions were 0.967 and 0.864 in the training and test cohorts,, with both P<0.001.
Impact: Deep learning holds promise for the noninvasive detection of sHCC, offering the potential to alleviate the workload of radiologists and mitigate the necessity for biopsies along with their associated complications.
Introduction
Hepatocellular carcinoma (HCC) accounts for 75%–85% of primary liver cancers, making it a global health concern [1,2]. Cirrhosis is a crucial risk factor for HCC [3, 4]. HCC is commonly believed to emerge from cirrhosis or cirrhosis-associated nodules, such as regenerative nodules (RNs), and dysplastic nodules (DNs). However, due to the extensive overlapping image features between sHCC and benign precancerous nodules, the detection of sHCC from cirrhosis liver is considered difficult and challenging [5,6].Recently, the application of artificial intelligence methods in image screening eased the process for the detection of sHCC. Nonetheless, traditional machine learning methods rely heavily on the hand-crafted features [7], making it laborious and time-consuming. Futhermore, manual segmentation often suffers from large inter-operator variability, which directly influences the accuracy of diagnosis. Deep learning (DL) has attracted attention in the interpretation of the radiology field, due to its ability to automatically extract predefined features, thereby reducinge the need for manual preprocessing steps and the workload of radiologists[8]. In particular, DL showed potential benefits for liver-related tasks, such as liver segmentation, liver tumor classification, and liver microvascular invasion prediction [9-14]. It is noted that previous studies are devoted to detecting large hepatocellular carcinoma. However, there has been limited research studying on the segmentation and detection of sHCC. Automated sHCC lesion segmentation remains difficult due to imaging quality, lesion size, and inconsistent variations between liver and lesion tissue. Consequently, detecting sHCC patients among cirrhotic patients is challenging.
This study had two aims: 1) utilize deep learning to segment liver and sHCC lesions automatically in cirrhotic livers; 2) identify sHCC patients among the cirrhotic patients using the lesion features on Gd-EOB-DTPA-enhanced MRI.
Methods
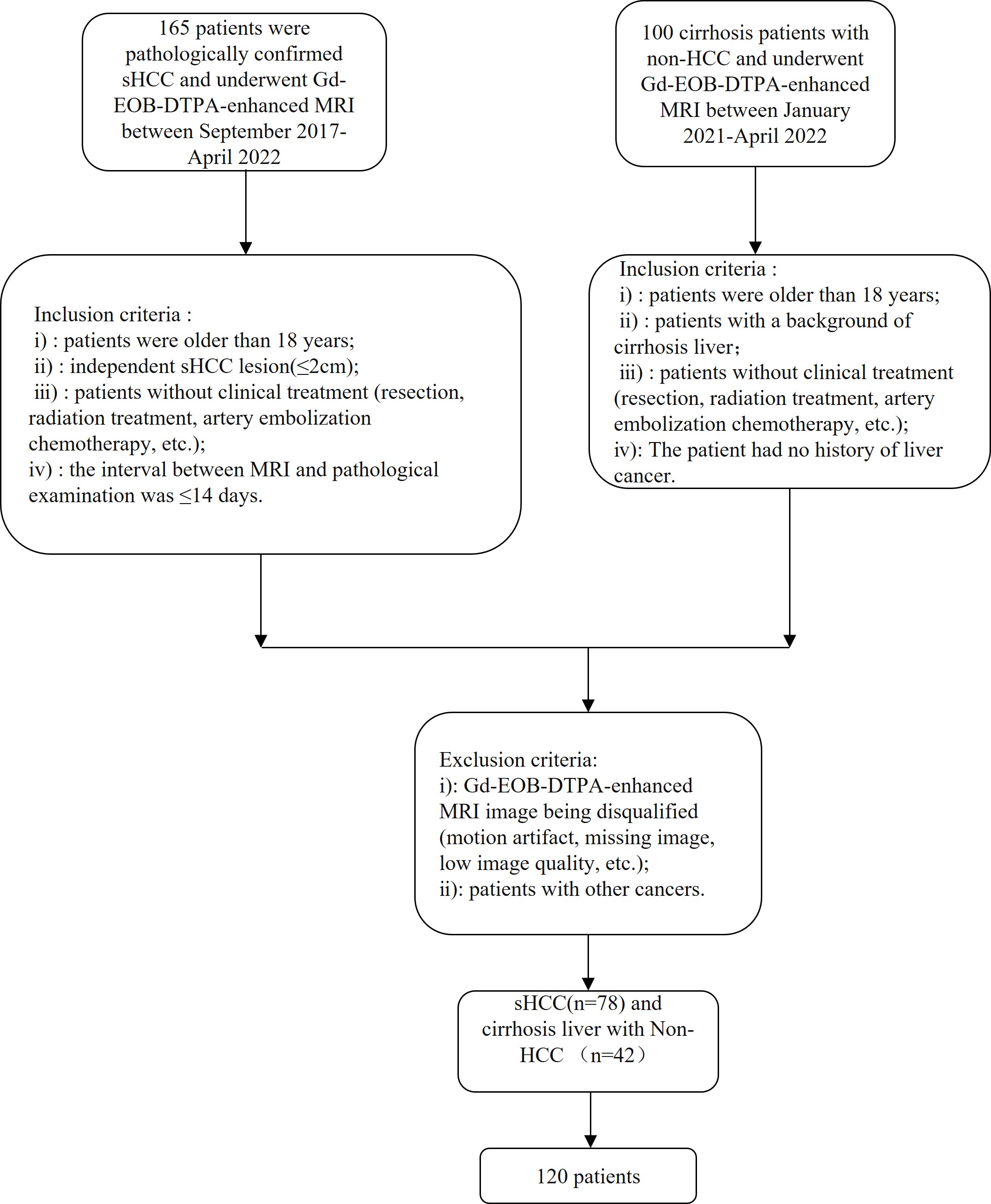
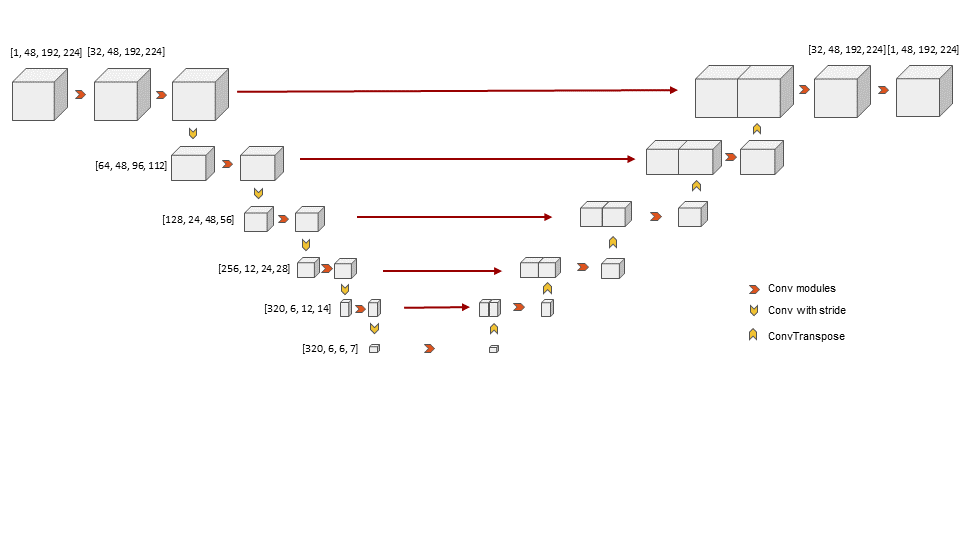
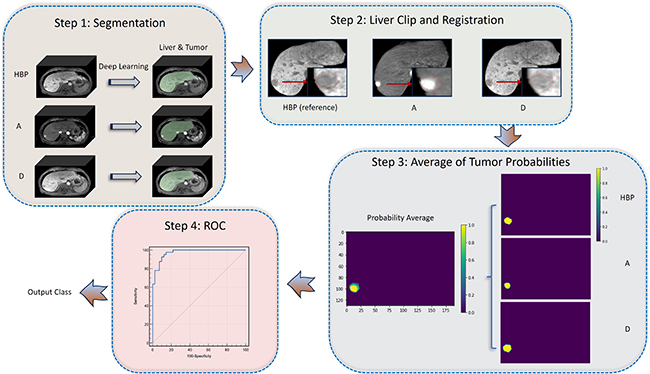
This retrospective study included cirrhotic patients with sHCC who underwent surgical resection and cirrhotic patients who were confirmed to be non-HCC by follow-up. Gd-EOB-DTPA-enhanced MRI data was acquired from September 2017 to April 2022. Figure 1 shows the patient selection process. The data was divided into training and test sets with an 8:2 ratio. A 3D nnU-Net deep learning network (Fig. 2) was trained to perform automatic segmentation of both liver and lesions. The average predicted probability for each lesion was calculated, and was utilized to generate a ROC curve for sHCC and non-sHCC lesion classification. Figure 3 shows the entire workflow for the detection method. The performance was evaluated at both lesion level and case levels. Lesion level assessment utilized the area under the receiver operating characteristic (AUC). Case level assessment utilized accuracy, sensitivity and specificity. The ROC curve and other metrics were calculated using MedCalc version 20.019 (MedCalc Software Ltd).Results
Finally, 120 patients (78 sHCC and 42 non-sHCC) were included in this retrospective study. The AUCs in distinguishing sHCC from non-sHCC at the lesion level were 0.967 and 0.864 in the training and test cohorts, with both P<0.001. At the case level, distinguishing patients with sHCC from cirrhotic patients yielded accuracies of 92.5% and 81.5%, sensitivities of 95.1% and 88.2%, and specificities of 87.5% and 70% for the training and test sets, respectively.Discussion
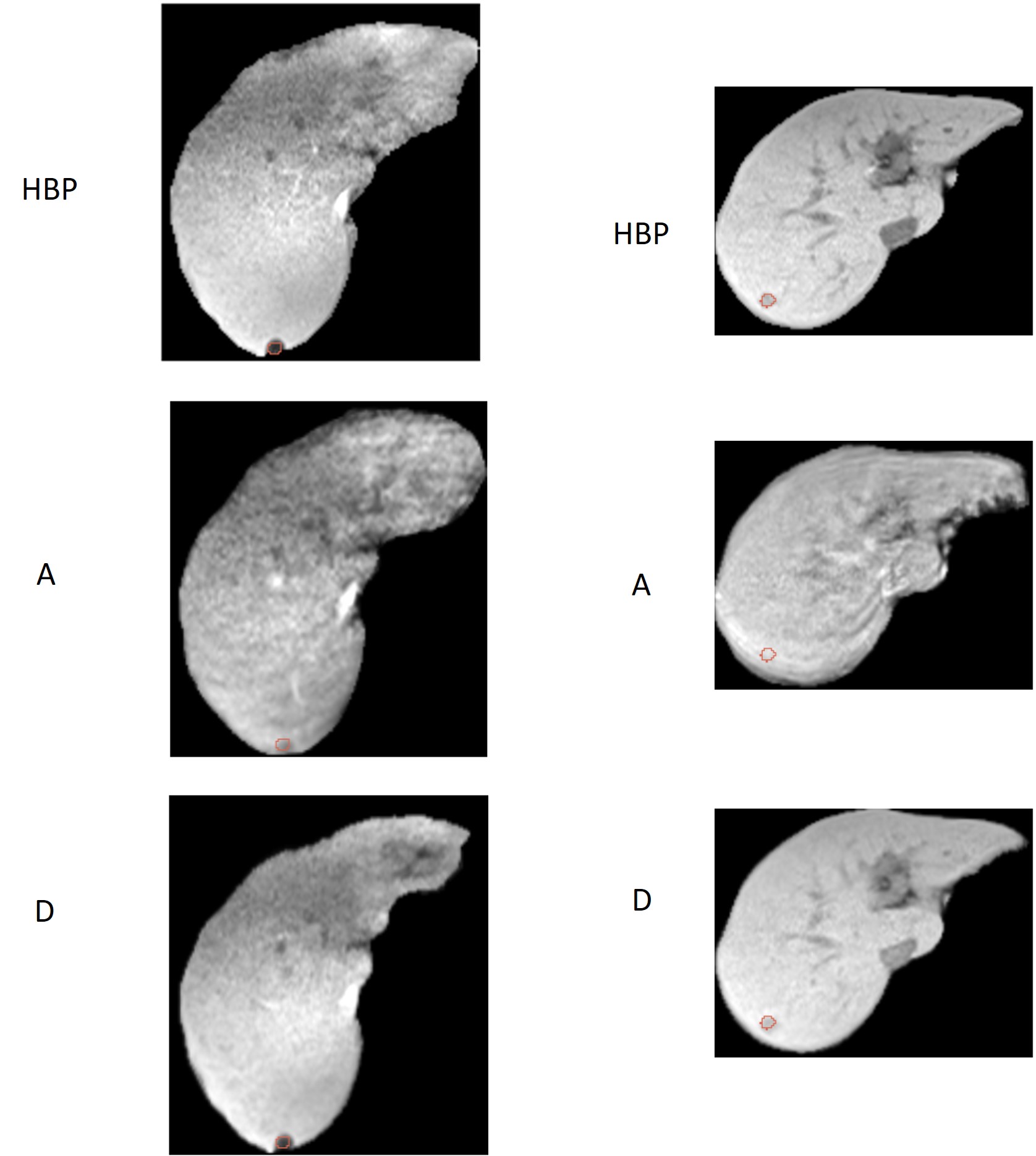
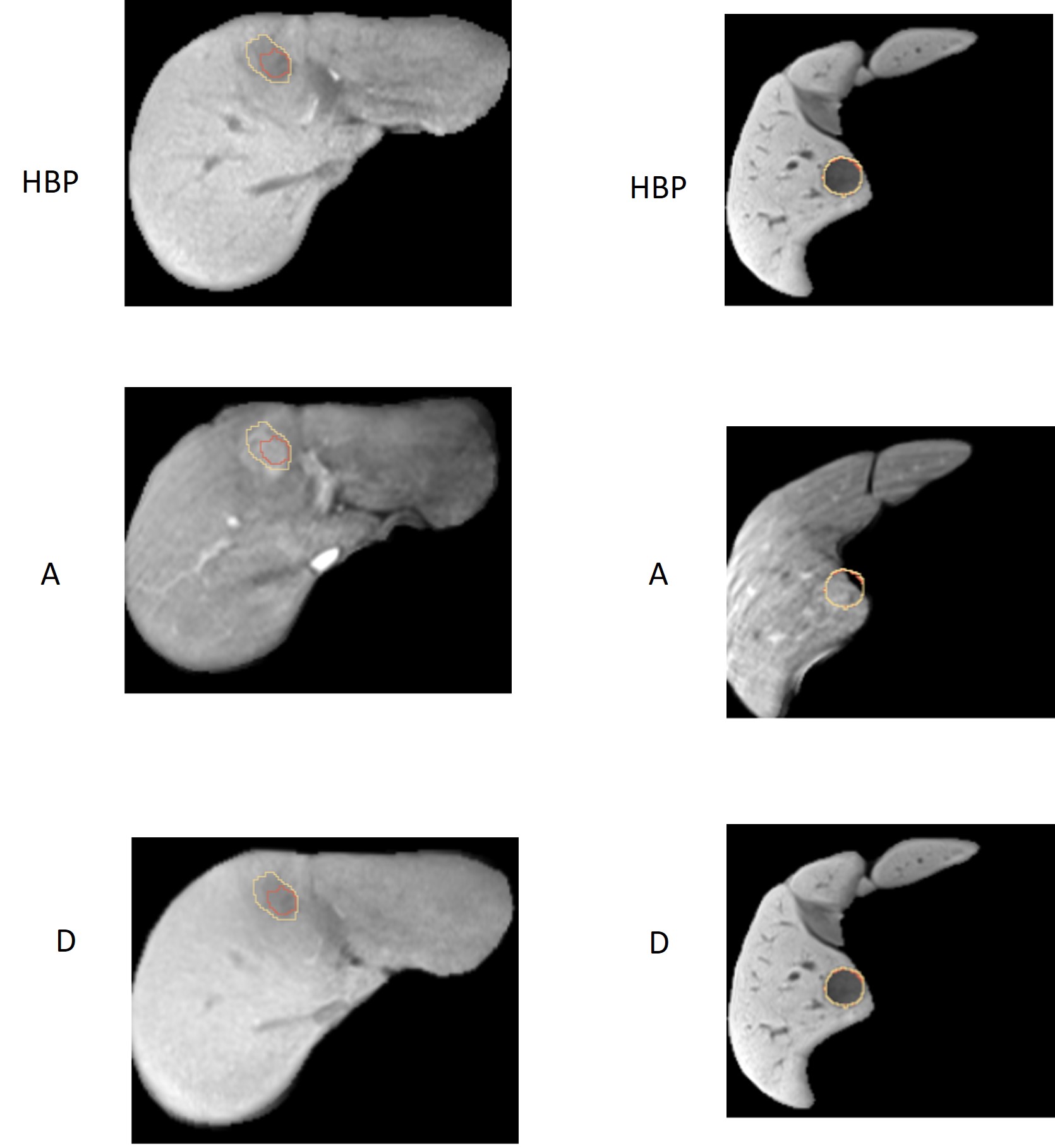
The most important innovation of this study is to fully automate the sHCC detection based on multiphase Gd-EOB-DTPA-enhanced MRI utilizing the deep learning method. The AUCs in distinguishing sHCC lesions from non-sHCC lesions were 0.967 and 0.864 in the train and test cohorts. Hence, the model demonstrated its proficiency in distinguishing sHCC lesions from nodules. The 81.5% accuracy on test set proved its effectiveness in discriminating sHCC patients in cirrhosis livers. Furthermore, we found that MRI Images acquired at the hepatobiliary phase as deep learning inputs provided a higher Dice coefficient for lesion segmentation (liver dice 0.95, tumor dice 0.58). Thus, the hepatobiliary phase image segmentation results were more suitable to be taken as the candidate sHCC lesions to be checked with other phases for the final sHCC detection. This study suggests that fully automatic deep learning has the potential to be applied to an approach in diagnosing sHCC based on Gd-EOB-DTPA-enhanced MRI. False positive and false negative examples were provided in Fig. 4 and Fig. 5. Some false positives were easy to exclude by experts by checking the multiphase information (Fig. 4 left ) while some were not (Fig. 4 right). The occurrence of false negatives was attributed to discrepancies in volume across multiple phases, necessitating further investigation.Conclusion
The deep learning method showed high performance for detecting sHCC among cirrhotic patients. Additionally, the application of deep learning can greatly reduce radiologists' workload.Acknowledgements
Thanks to the Philips Healthcare research team for their technical support.References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021.
2. Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018;68(2):723-50.
3. Yang JD, Hainaut P, Gores GJ, Amadou A, Plymoth A, Roberts LR. A global view of hepatocellular carcinoma: trends, risk, prevention and management. Nat Rev Gastroenterol Hepatol. 2019;16(10):589-604.
4. Mak LY, Cruz-Ramón V, Chinchilla-López P, et al. Global Epidemiology, Prevention, and Management of Hepatocellular Carcinoma. Am Soc Clin Oncol Educ Book. 2018;38:262-79.
5. Xie DY, Ren ZG, Zhou J, Fan J, Gao Q. 2019 Chinese clinical guidelines for the management of hepatocellular carcinoma: updates and insights. Hepatobiliary Surg Nutr. 2020;9(4):452-63.
6. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358-80.
7. Zhong X, Tang H, Lu B, et al. Differentiation of Small Hepatocellular Carcinoma From Dysplastic Nodules in Cirrhotic Liver: Texture Analysis Based on MRI Improved Performance in Comparison Over Gadoxetic Acid-Enhanced MR and Diffusion-Weighted Imaging. Front Oncol. 2019;9:1382.
8. Tran KA, Kondrashova O, Bradley A, Williams ED, Pearson JV, Waddell N. Deep learning in cancer diagnosis, prognosis and treatment selection. Genome Med. 2021;13(1):152.
9. Araújo JDL, da Cruz LB, Diniz JOB, et al. Liver segmentation from computed tomography images using cascade deep learning. Comput Biol Med. 2021;140:105095.
10. Budak Ü, Guo Y, Tanyildizi E, Şengür A. Cascaded deep convolutional encoder-decoder neural networks for efficient liver tumor segmentation. Med Hypotheses. 2020;134:109431.
11. Koichiro Y, Hiroyuki A, Osamu A, Shigeru K. Deep Learning with Convolutional Neural Network for Differentiation of Liver Masses at Dynamic Contrast-enhanced CT: A Preliminary Study. Radiology. 2018;286(3).
12. Hamm CA, Wang CJ, Savic LJ, et al. Deep learning for liver tumor diagnosis part I: development of a convolutional neural network classifier for multi-phasic MRI. European Radiology. 2019;29(7):3338-47. 13. Bousabarah K, Letzen B, Tefera J, et al. Automated detection and delineation of hepatocellular carcinoma on multiphasic contrast-enhanced MRI using deep learning. Abdominal Radiology. 2021;46(1):216-25.
14. Zhang Y, Lv X, Qiu J, et al. Deep Learning With 3D Convolutional Neural Network for Noninvasive Prediction of Microvascular Invasion in Hepatocellular Carcinoma. J Magn Reson Imaging. 2021;54(1):134-43.
Figures