3623
A machine learning approach based on multiparametric MRI to identify the risk of non-sentinel lymph node metastasis in patients with breast cancer1Weifang Medical University, Weifang, China, 2WeiFang Traditional Chinese Hospital, Weifang, China, 3GE Healthcare, Taiwan, China
Synopsis
Keywords: Diagnosis/Prediction, Breast
Motivation: ALN status is crucial for clinical staging, prognosis assessment, and treatment decision for breast cancer patients.
Goal(s): We aimed to assess feasibility of ML based on mpMRI for predicting the risk of NSLN metastasis in breast cancer patients.
Approach: mpMRI including T1WI, T2WI, DWI, and DCE-MRI was acquired, and four ML models were constructed.
Results: ML model incorporating mpMRI features and clinical factors can predict NSLN metastasis with fair accuracy for breast cancer, with an AUC of 0.781 in test dataset. Five factors for NSLN metastasis were found, including histological grade, cortical thickness, fatty hilum, short axis of lymph node, and age.
Impact: The proposed ML model may benefit for breast cancer patients with 1-2 positive SLN but consistently negative NSLN to avoid overtreatment and improve individualized axillary management.
Introduction
Axillary lymph node (ALN) status is crucial for clinical staging, prognosis assessment, and treatment decision for breast cancer patients (1). Sentinel lymph node (SLN) is the first organ where metastatic cancer cells reach (2,3). Currently, sentinel lymph node biopsy (SLNB) procedure is routinely employed to assess regional lymph node involvement of patient with breast cancer. The standard treatment for breast cancer patients with SLN metastasis is a thorough axillary lymph node dissection (ALND) (4,5). However, ALND are accompanied with complications such as lymphedema, limited arm motion, and neuropathic pain (6). International Breast Cancer Study Group (IBCSG) 23-01 had revealed that ALND for 1-2 SLN metastases in early breast cancer did not confer a survival benefit (7,8), which was further confirmed by a long-term follow-up study of the Z0011 trial (9). Therefore, it is controversial whether complete ALND is required for patients with SLN metastasis and local recurrence (LR) of lymph node metastasis. Machine learning (ML) has emerged as a new type of artificial intelligence, and has been widely used for classification, prediction, and decision-making in biomedicine (10-12). Multiparametric MRI (mpMRI) has been widely applied for breast imaging. By combining morphological and functional sequences, it not only provides morphological characteristics of the tumor, but also reflect pathological alterations associated with the lesion. However, the potential of ML based on features extracted from mpMRI has not been fully explored (13-15). Therefore, we aimed to assess the feasibility of ML based on mpMRI including T1WI, T2WI, DWI, and DCE-MRI, for predicting the risk of non-SLN (NSLN) metastasis in breast cancer patients, which may benefit for breast cancer patients with 1-2 positive SLN but consistently negative NSLN, to avoid overtreatment and improve individualized axillary management.
Materials and Methods
All patients were randomly divided into training dataset (100 cases) and test dataset (44 cases) at a ratio of 7:3. A total of 24 features were extracted from mpMRI images, and were rescaled to range [0, 1] to reduce the excessive reliance on a certain feature. To avoid model overfitting, reduce the redundancy, and find the optimal feature subset, feature selection was conducted using ANOVA and Pearson correlation analysis. Four types of ML algorithms were applied in this study, including logistic regression (LR), extreme gradient boosting (XGBoost), random forest (RF), and support vector classification (SVC). Model confusion matrix, including true positive (TP), true negative (TN), false positive (FP), false negative (FN), was obtained. Accuracy, sensitivity, specificity, F1 score, and area under the ROC curve (AUC) were used to evaluate the performance of ML models. Cohen’s Kappa was used to assess interrater reliability between two readers. All data analysis was performed using Python (3.7.4) and Jupyter lab software (3.0) with Scikit-learn library (1.0.2). A p-value less than 0.05 was considered statistically significant.Results
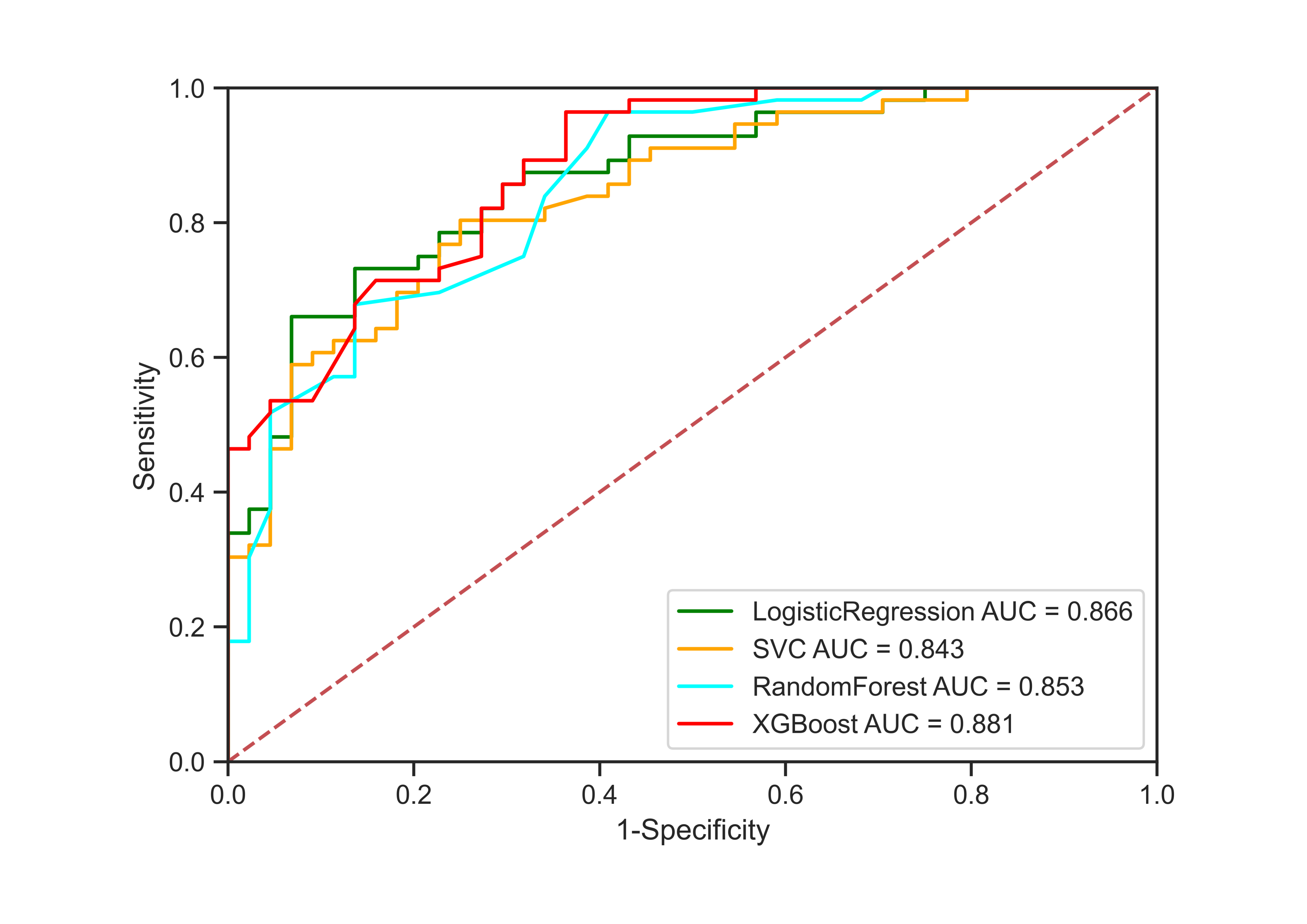
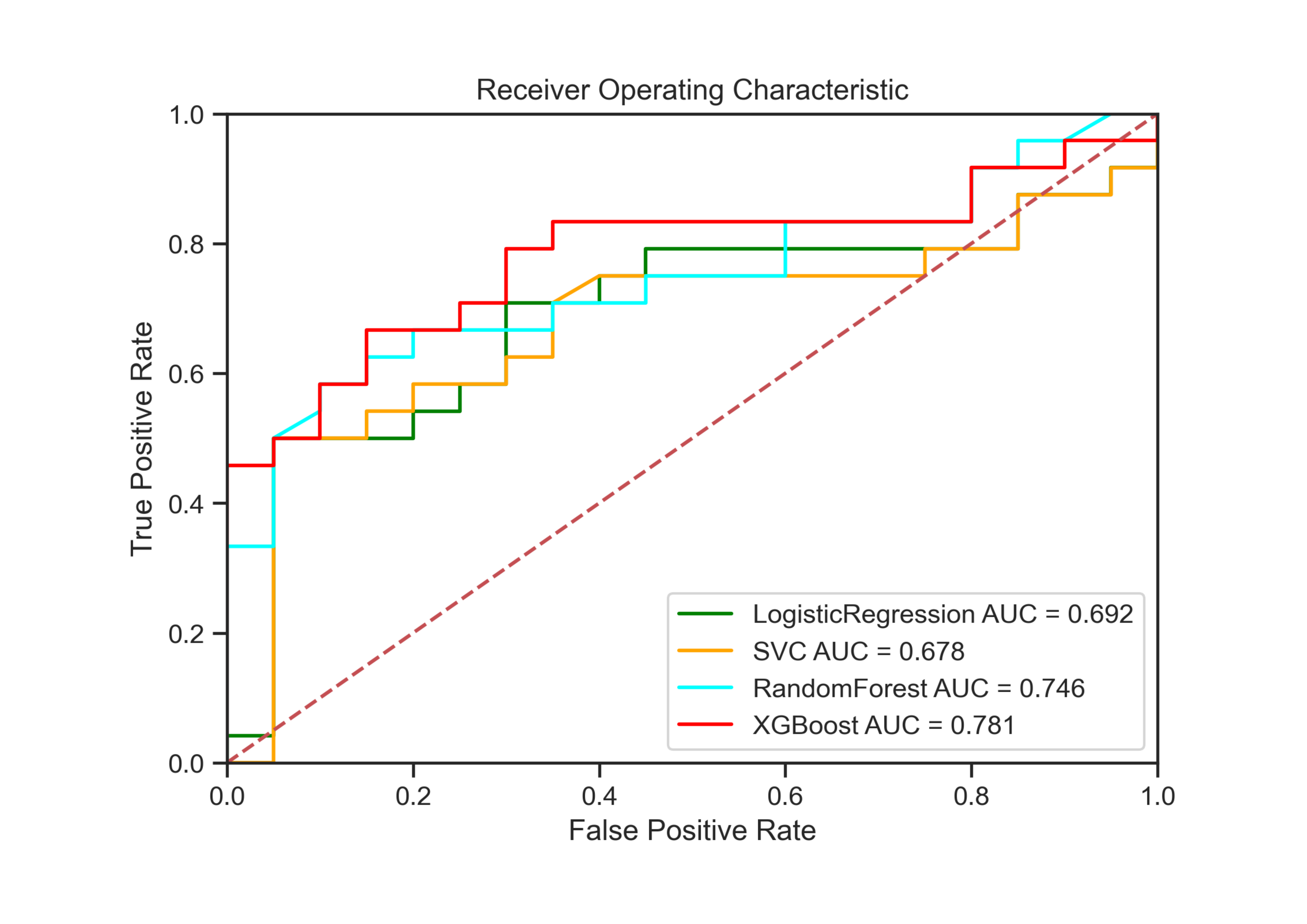
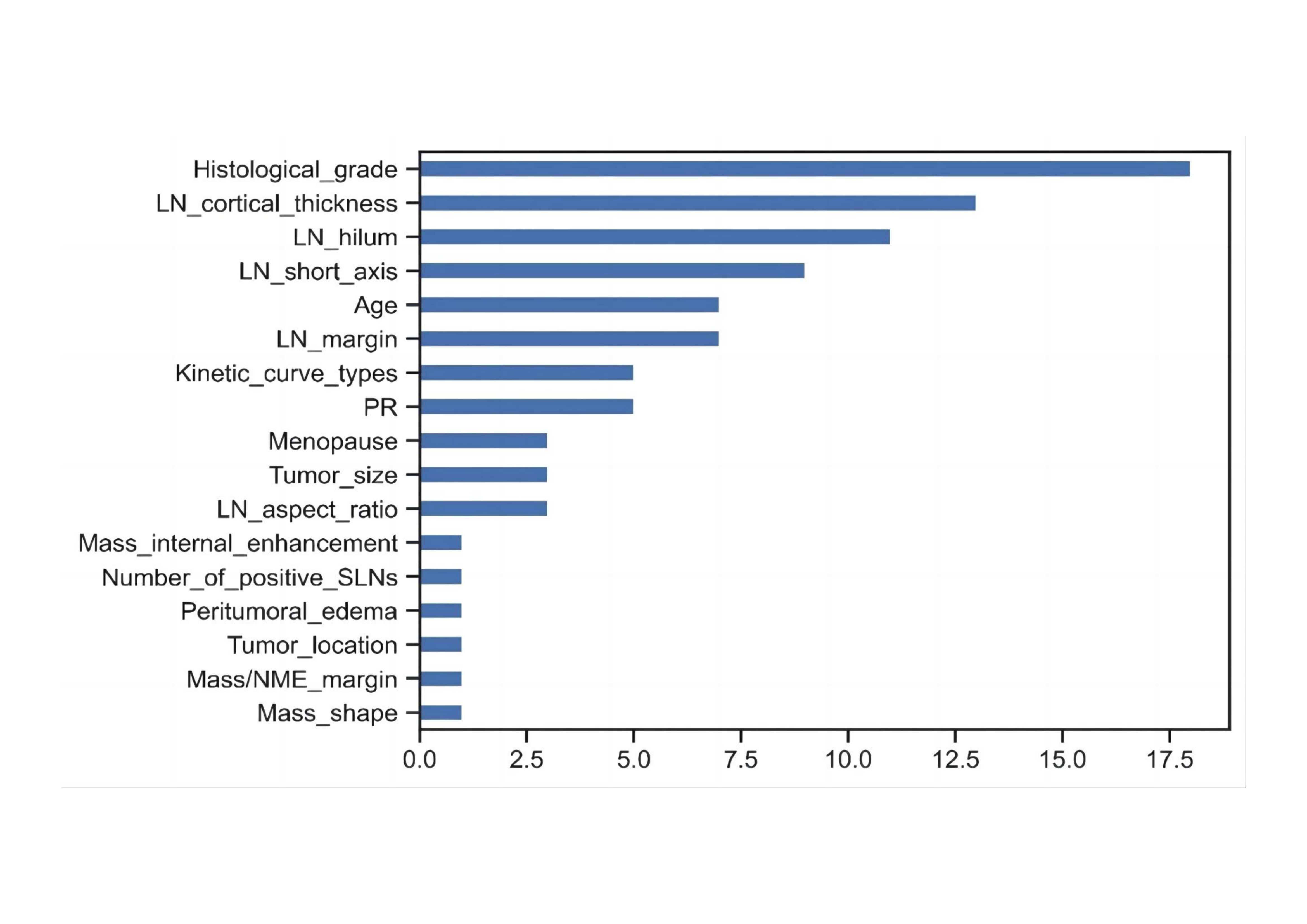
Figure 1 displays that for the training dataset, AUC values of the XGBoost, LR, SVC, and RF models for NSLN metastasis prediction were 0.881, 0.866,0.843, and 0.853, respectively. In the test dataset, AUC values of the XGBoost, LR, SVC, and RF models were 0.781, 0.692,0.680, and 0.705, respectively. We then applied the optimal model from the training dataset to the test dataset to obtain the performance evaluation metrics. The evaluation results of feature importance obtained by using the optimal model XGBoost in this experiment are shown in Figure 2. The most important feature in predicting NSLN metastasis was histological grade, followed by morphological features of lymph nodes, including cortical thickness, fatty hilum, short axis, and margin.Discussion
Previous studies have adopted ML model for differentiating benign and malignant breast nodules. However, few studies used ML methods combined with imaging features to predict NSLN metastasis in breast cancer patients. In this study, four ML models based on clinical features and features extracted from mpMRI were constructed to predict NSLN metastasis, achieving an optimal AUC value of 0.781 in the test dataset. Compared to results reported in previous studies, our proposed XGBoost model performed better than most clinical models, while not as well as some radiomics models. In conclusion, ML model based on mpMRI enables early prediction of the risk of NSLN metastasis in 1-2 SLN-positive breast cancer patients with fair accuracy. These findings may shed light on the realization of precision medicine in breast cancer.Acknowledgements
No acknowledgement found.References
1. Kim MY. Breast Cancer Metastasis. Advances In Experimental Medicine and Biology. 2021;1187:183-204.
2. Berg JW. The significance of axillary node levels in the study of breast carcinoma. Cancer. 1955;8:776-778.
3. Okur O, Sagiroglu J, Kir G, et al. Diagnostic accuracy of sentinel lymph node biopsy in determining the axillary lymph node metastasis. J Cancer Res Ther. 2020;16:1265-1268.
4. Veronesi U, Paganelli G, Viale G, et al. A randomized comparison of sentinel-node biopsy with routine axillary dissection in breast cancer. The New England Journal of Medicine. 2003;349:546-553. 5. Rao R, Euhus D, Mayo HG, et al. Axillary node interventions in breast cancer: a systematic review. JAMA. 2013;310:1385-1394.
6. Brackstone M, Baldassarre FG, Perera FE, et al. Management of the Axilla in Early-Stage Breast Cancer: Ontario Health (Cancer Care Ontario) and ASCO Guideline. J Clin Oncol. 2021;39:3056-3082. 7. Lucci A, McCall LM, Beitsch PD, et al. Surgical complications associated with sentinel lymph node dissection (SLND) plus axillary lymph node dissection compared with SLND alone in the American College of Surgeons Oncology Group Trial Z0011. J Clin Oncol. 2007;25:3657-3663.
8. Galimberti V, Cole BF, Zurrida S, et al. Axillary dissection versus no axillary dissection in patients with sentinel-node micrometastases (IBCSG 23-01): a phase 3 randomised controlled trial. Lancet Oncol. 2013;14:297-305.
9. Giuliano AE, Ballman KV, McCall L, et al. Effect of Axillary Dissection vs No Axillary Dissection on 10-Year Overall Survival Among Women With Invasive Breast Cancer and Sentinel Node Metastasis: The ACOSOG Z0011 (Alliance) Randomized Clinical Trial. JAMA. 2017;318:918-926.
10. Nattkemper TW, Arnrich B, Lichte O, et al. Evaluation of radiological features for breast tumour classification in clinical screening with machine learning methods. Artif Intell Med. 2005;34:129-139. 11. Tahmassebi A, Wengert GJ, Helbich TH, et al. Impact of Machine Learning With Multiparametric Magnetic Resonance Imaging of the Breast for Early Prediction of Response to Neoadjuvant Chemotherapy and Survival Outcomes in Breast Cancer Patients. Invest Radiol. 2019;54:110-117.
12. Madekivi V, Bostrom P, Karlsson A, et al. Can a machine-learning model improve the prediction of nodal stage after a positive sentinel lymph node biopsy in breast cancer? Acta Oncol. 2020;59:689-695. 13. Liu C, Ding J, Spuhler K, et al. Preoperative prediction of sentinel lymph node metastasis in breast cancer by radiomic signatures from dynamic contrast-enhanced MRI. J Magn Reson Imaging. 2019;49:131-140.
14. Choi EJ, Youk JH, Choi H, et al. Dynamic contrast-enhanced and diffusion-weighted MRI of invasive breast cancer for the prediction of sentinel lymph node status. J Magn Reson Imaging. 2020;51:615-626.
15. Liu Z, Feng B, Li C, et al. Preoperative prediction of lymphovascular invasion in invasive breast cancer with dynamic contrast-enhanced-MRI-based radiomics. J Magn Reson Imaging. 2019;50:847-857.
Figures