3618
T2 -Weighted MR Imaging-Based Radiomics Model for Evaluating the Activity of Thyroid-Associated Ophthalmopathy1Peking University People's Hospital, Beijing, China, 2Philips Healthcare, Beijing, China
Synopsis
Keywords: Diagnosis/Prediction, Machine Learning/Artificial Intelligence
Motivation: The assessment of thyroid-associated ophthalmopathy (TAO) activity is crucial for determining the appropriate treatment. However, it was based on clinical activity score(CAS) which relies on subjective symptoms and judgment heavily.
Goal(s): The aim of this study was to establish an objective evaluating model for TAO’s activity based on MR Imaging-Derived Radiomics.
Approach: MR Imaging was performed for different activity status of TAO patients, after that radiomics features were extracted and selected. Radiomics models were constructed.
Results: The radiomics model of T2 weighted SPIR-based extraocular muscles can achieve satisfactory performance than those of optic nerve or interorbital tissue in evaluating the activity of TAO.
Impact: This study constructed the T2 -weighted MR imaging-derived radiomics model to evaluate the activity of thyroid-associated ophthalmopathy, which could be a more objective and consistent evaluating approach than clinical activity score.
Introduction
Thyroid-Associated Ophthalmopathy (TAO) is an inflammatory autoimmune disorder that affects the orbital and periorbital tissues(1,2). It is characterized by orbital inflammation, fibrosis, and adipogenesis, which tends to result in various ocular morbidities, such as photophobia, eyelid retraction, and optic neuropathy(3). The assessment of TAO activity is crucial for determining the appropriate treatment and prognosis(4). However, the widely use of clinical activity score (CAS) heavily relies on subjective symptoms and signs, resulting in low interobserver agreement and reproducibility. Due to its high soft tissue resolution, orbital MRI can provide more objective and comprehensive insights into the internal structure of orbits(5). Radiomics features, derived from medical images, have great potential for predicting, prognosticating, and personalized medicine(6,7). Therefore, the aim of this study was to establish an objective evaluation model for the activity of TAO based on T2-Weighted MR imaging-derived radiomics.Methods
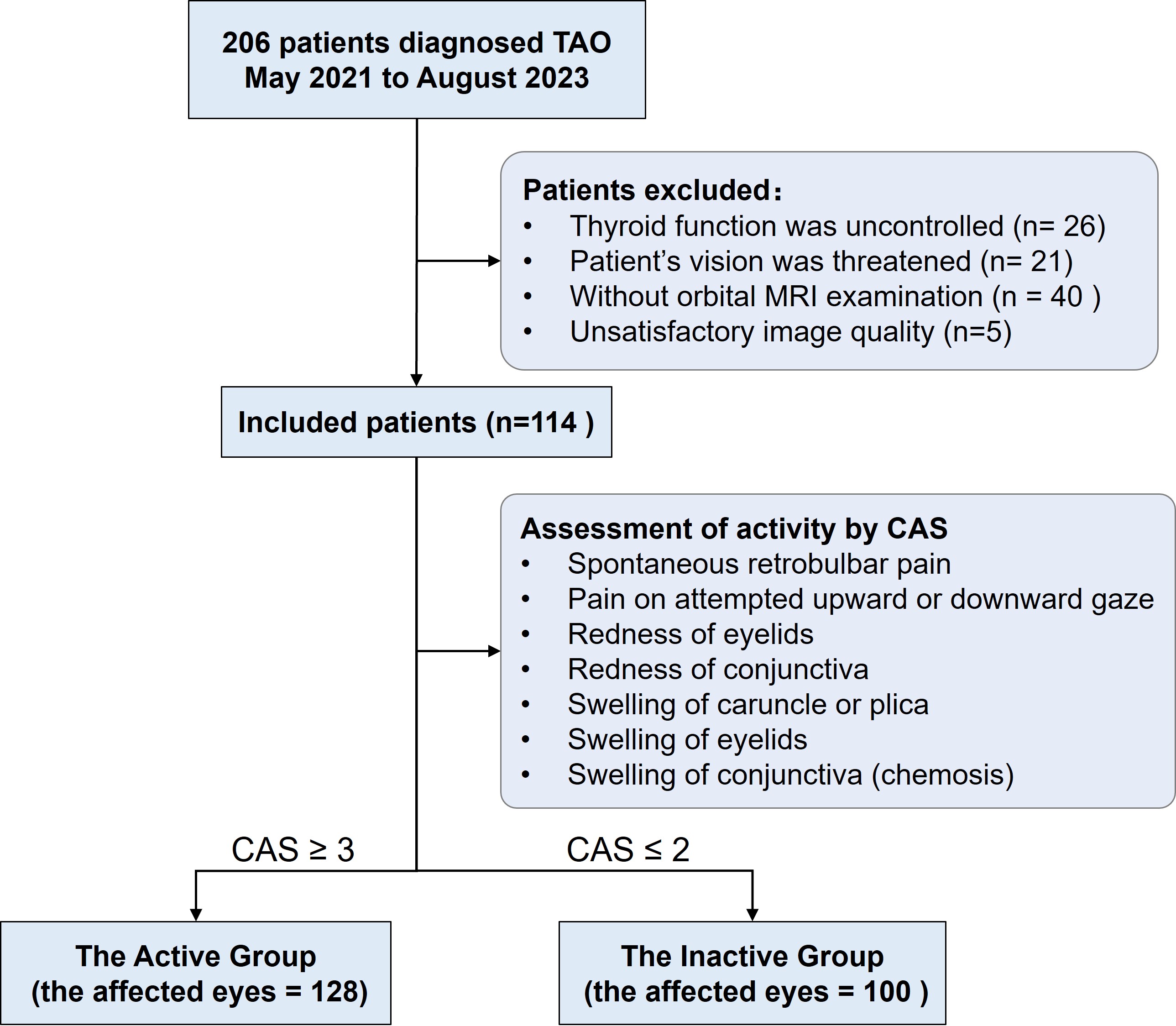
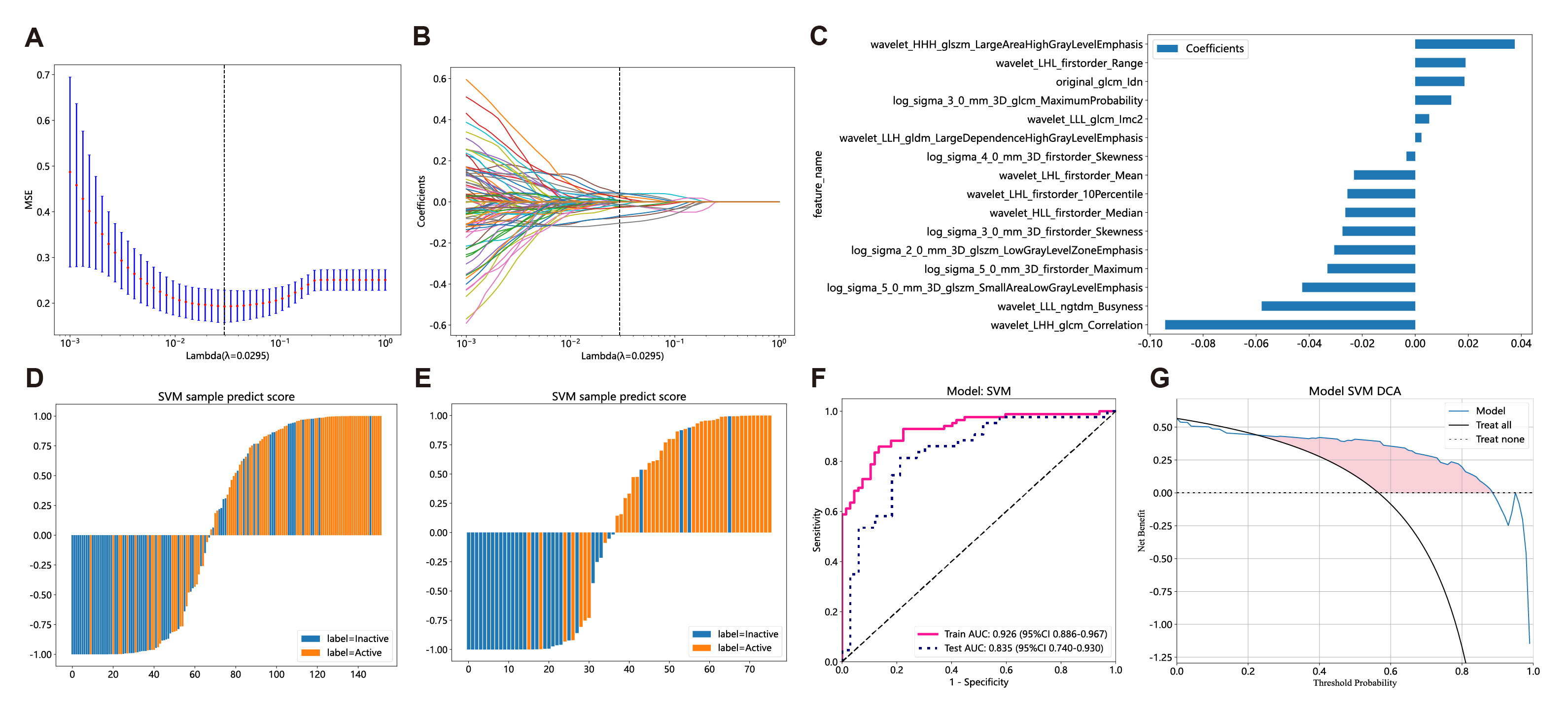
206 TAO patients were enrolled in this study according to the inclusion and exclusion criteria (Figure 1). 228 single eyes were divided into the active group (n= 128) and the inactive group (n= 100) based on CAS(4). The coronal T2-weighted spectral presaturation with inversion recovery (SPIR) sequence of anonymized orbital MR images were resampled (1x1x1 mm3 ) and corrected using N4 bias correction (Figure2). And radiomics features of extraocular muscles, optic nerve and interorbital tissue were extracted separately, including firstorder, shape, gray-level co-occurrence matrix (GLCM), gray-Level run-length matrix (GLRLM), gray-level size zone matrix (GLSZM), gray level difference method (GLDM) and neighborhood gray-tone difference matrix (NGTDM). The dataset was then randomly divided into training (n = 181) and testing cohorts (n = 46). After the z-score standardization, features were selected by t-test (p-value < 0.001), Pearson correlation (threshold = 0.9) and the least absolute shrinkage and selection operator (LASSO) regression. Nine machine learning classifiers were applicated to construct radiomics models, such as Support vector machine (SVM), Light Gradient Boosting Machine (LightGBM) and so on. The models were evaluated and compared by receiver operating characteristic (ROC) curve and Delong test.Results
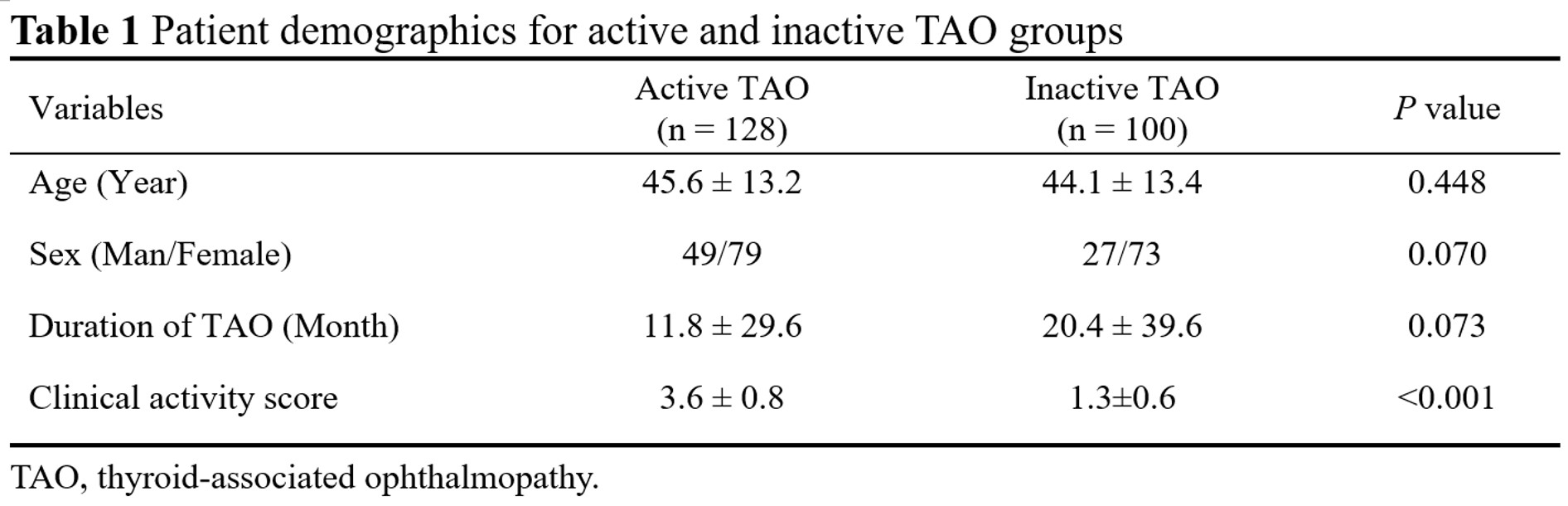
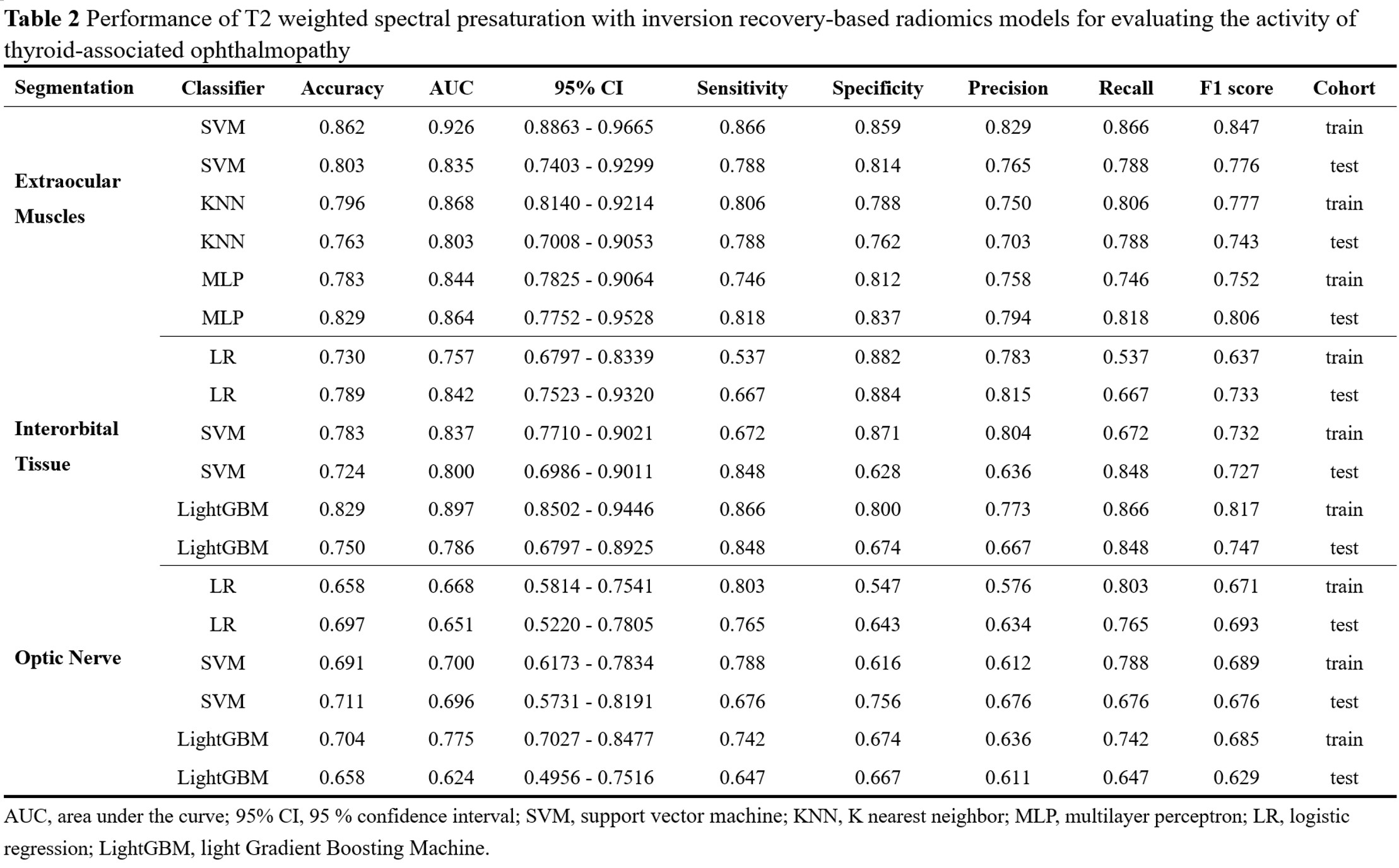
A total of 114 patients (38 men, 76 women; age, 44.9 ± 13.3 years) diagnosed TAO were finally enrolled in this study. The median time between the appearance of symptoms and the MR examination was 8.0 months (range, 1- 240 months). Among these patients, 128 eyes (49 men, 79 women; age, 45.6 ± 13.2 years) exhibited active TAO ,while 100 eyes (27 men, 73 women; age, 44.1 ± 13.4 years) had inactive TAO (Table 1).Performance of T2 weighted SPIR-based radiomics models for evaluating the activity of thyroid-associated ophthalmopathy were shown in Table 2. The area under the ROC curve (AUC) of the best radiomics model of extraocular muscles was 0.926 (95% confidence interval, 0.886 - 0.967; sensitivity: 86.6%; specificity:85.9%) in the training cohort and 0.835 (0.740 - 0.930; 78.8%; 81.4%) in the test cohort by SVM (Figure 3). The AUC of the best radiomics model of interorbital tissue was 0.897 (0.850 - 0.945; 86.6%;80.0%) in the training cohort and 0.746 (0.680 - 0.893; 84.8%; 67.4%) in the test cohort by LightGBM. The AUC of the best radiomics model of optic nerve by SVM was 0.700 (0.6173 - 0.7834; 78.8%; 61.6%) in the training and 0.696 (0.5731 - 0.8191; 67.6%; 75.6%) in the test cohort.
Discussion
TAO patients have orbital soft tissue involvement that causes swelling of the extraocular muscles, adipose tissue, and connective tissue (8). This may compress the optic nerve and lead to visual impairment (9,10). Orbital MRI is a valuable diagnostic tool for TAO, as it can reveal the size and inflammatory changes of the extraocular muscles and other soft tissue(11–13). Previous studies have suggested that T2-weighted imaging is one of the most reliable sequences to estimate the clinical activity score of TAO (11,14). This study demonstrated that the radiomics model based on T2-weighted MR imaging has potential for evaluating the activity of TAO.The main pathological features of active TAO are inflammation and edema in the extraocular muscles, as well as lymphocytic infiltration(15–17). In contrast, the inactive phase is marked by interstitial fibrosis, collagen accumulation, and fatty infiltration(18,19).Furthermore, the T2-weighted radiomics model based on extraocular muscles showed better performance than the models based on optic nerve or interorbital tissue in assessing the activity of TAO patients. This may attribute to the fact that the optic nerve does not exhibit obvious abnormalities during the early stages of active TAO, which reduces the diagnostic accuracy of the radiomics model for this tissue.
Conclusion
The T2 weighted SPIR-based radiomics model of extraocular muscles can achieve satisfactory performance than those of optic nerve or interorbital tissue in evaluating the activity of TAO patients.Acknowledgements
Not applicable.References
1. Bahn RS. Graves’ Ophthalmopathy. N Engl J Med. 2010 Feb 25;362(8):726–38.
2. Diao J, Chen X, Shen Y, Li J, Chen Y, He L, et al. Research progress and application of artificial intelligence in thyroid associated ophthalmopathy. Front Cell Dev Biol. 2023;11:1124775.
3. Genere N, Stan MN. Current and Emerging Treatment Strategies for Graves’ Orbitopathy. Drugs. 2019 Feb;79(2):109–24.
4. Bartalena L, Kahaly GJ, Baldeschi L, Dayan CM, Eckstein A, Marcocci C, et al. The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves’ orbitopathy. Eur J Endocrinol. 2021 Aug 27;185(4):G43–67.
5. Wnuk E, Maj E, Jabłońska-Pawlak A, Jeczeń M, Rowińska-Berman K, Rowiński O. Validation of exophthalmos magnetic resonance imaging measurements in patients with Graves’ orbitopathy, compared to ophthalmometry results. pjr. 2022;87(1):539–44.
6. Rizzo S, Botta F, Raimondi S, Origgi D, Fanciullo C, Morganti AG, et al. Radiomics: the facts and the challenges of image analysis. Eur Radiol Exp. 2018 Nov 14;2(1):36.
7. Guiot J, Vaidyanathan A, Deprez L, Zerka F, Danthine D, Frix AN, et al. A review in radiomics: Making personalized medicine a reality via routine imaging. Med Res Rev. 2022 Jan;42(1):426–40.
8. Bartley GB, Gorman CA. Diagnostic Criteria for Graves’ Ophthalmopathy. American Journal of Ophthalmology. 1995 Jun;119(6):792–5.
9. Bucala RJ. Targeting fibrocytes in autoimmunity. Proc Natl Acad Sci U S A. 2022 Feb 1;119(5):e2121739119.
10. Beden Ü, Kaya S, Yeter V, Erkan D. Contrast sensitivity of thyroid associated ophthalmopathy patients without obvious optic neuropathy. ScientificWorldJournal. 2013;2013:943789.
11. Yokoyama N, Nagataki S, Uetani M, Ashizawa K, Eguchi K. Role of magnetic resonance imaging in the assessment of disease activity in thyroid-associated ophthalmopathy. Thyroid. 2002 Mar;12(3):223–7.
12. Rodríguez-González N, Pérez-Rico C, López-Para Giménez R, Arévalo-Serrano J, Del Amo García B, Calzada Domingo L, et al. Short-tau inversion-recovery (STIR) sequence magnetic resonance imaging evaluation of orbital structures in Graves’ orbitopathy. Arch Soc Esp Oftalmol. 2011 Nov;86(11):351–7.
13. Szucs-Farkas Z, Toth J, Balazs E, Galuska L, Burman KD, Karanyi Z, et al. Using morphologic parameters of extraocular muscles for diagnosis and follow-up of Graves’ ophthalmopathy: diameters, areas, or volumes? AJR Am J Roentgenol. 2002 Oct;179(4):1005–10.
14. Kirsch EC, Kaim AH, De Oliveira MG, von Arx G. Correlation of signal intensity ratio on orbital MRI-TIRM and clinical activity score as a possible predictor of therapy response in Graves’ orbitopathy--a pilot study at 1.5 T. Neuroradiology. 2010 Feb;52(2):91–7.
15. Ma R, Cheng Y, Gan L, Zhou X, Qian J. Histopathologic study of extraocular muscles in thyroid-associated ophthalmopathy coexisting with ocular myasthenia gravis: a case report. BMC Ophthalmol. 2020 Apr 22;20(1):166.
16. Papageorgiou KI, Hwang CJ, Chang SHH, Jarullazada I, Chokron Garneau H, Ang MJ, et al. Thyroid-associated periorbitopathy: eyebrow fat and soft tissue expansion in patients with thyroid-associated orbitopathy. Arch Ophthalmol. 2012 Mar;130(3):319–28.
17. Kaichi Y, Tanitame K, Terada H, Itakura H, Ohno H, Yoneda M, et al. Thyroid-associated Orbitopathy: Quantitative Evaluation of the Orbital Fat Volume and Edema Using IDEAL-FSE. Eur J Radiol Open. 2019;6:182–6.
18. Ludgate M, Baker G. Unlocking the immunological mechanisms of orbital inflammation in thyroid eye disease. Clin Exp Immunol. 2002 Feb;127(2):193–8.
19. Bartalena L, Pinchera A, Marcocci C. Management of Graves’ ophthalmopathy: reality and perspectives. Endocr Rev. 2000 Apr;21(2):168–99.
Figures