3614
Prediction of intra-tumoural tertiary lymphoid structures in intrahepatic cholangiocarcinoma using MRI-based radiomics1Department of Diagnostic Radiology, Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2Department of Hepatobiliary Surgery, Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 3Magnetic Resonance Imaging Research, General Electric Healthcare, Beijing, China, Beijing, China, 4Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
Synopsis
Keywords: Diagnosis/Prediction, Biliary, Biomarkers; Intrahepatic cholangiocarcinoma; Magnetic resonance imaging; Tertiary lymphoid structures; Radiomics
Motivation: Tertiary lymphoid structures (TLSs) can only be assessed by postoperative specimen and a non-invasive tool to preoperatively evaluate TLSs is still lacking.
Goal(s): To explore the association between TLSs status of patients with ICC and preoperative magnetic resonance imaging (MRI) radiomics analysis.
Approach: Radiomics features were subjected to LASSO regression to select the most associated features of TLSs and construct the radiomics model.
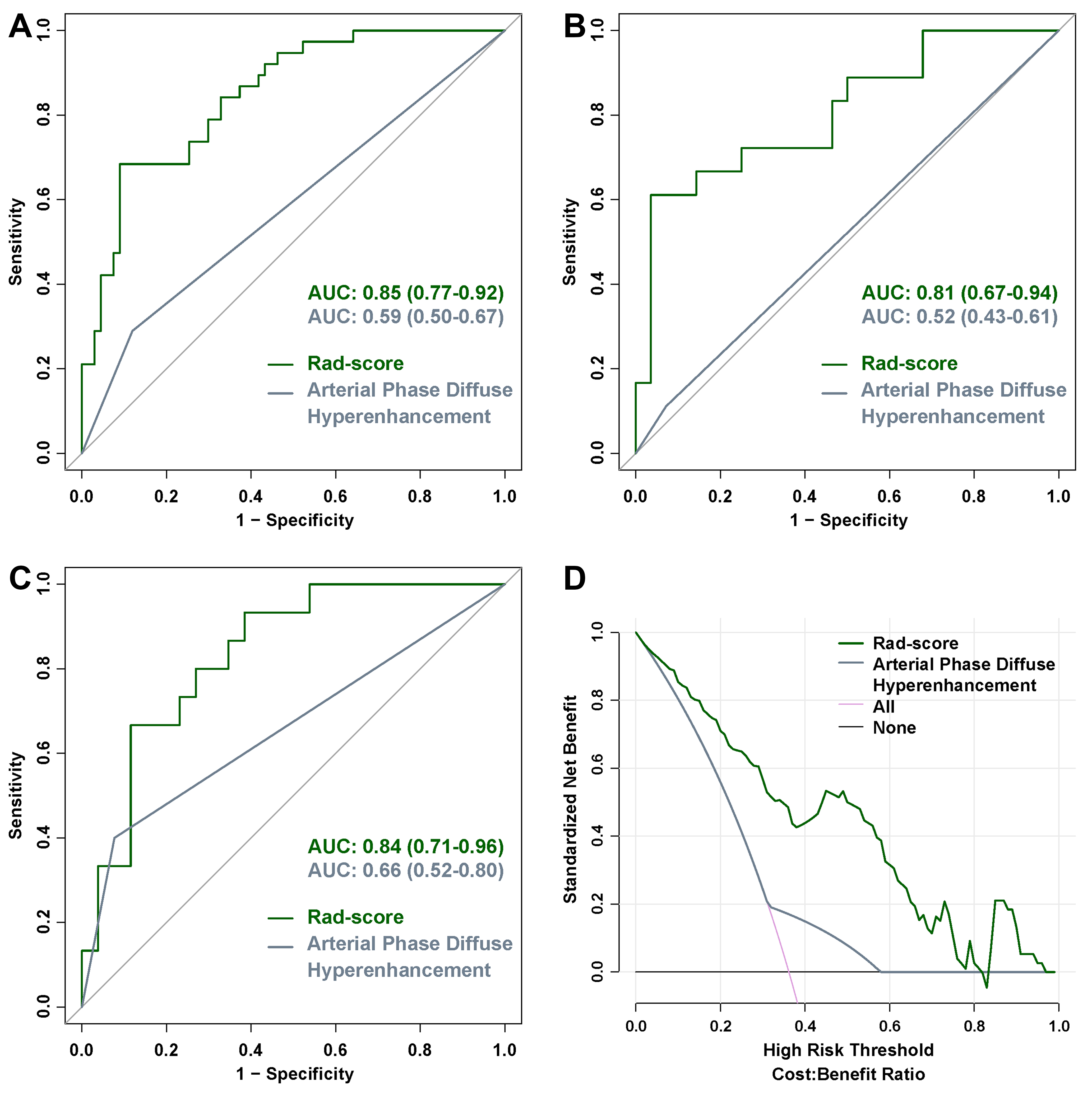
Results: The AUCs of Rad-score were 0.85, 0.81, and 0.84 in the T, V1, and V2 cohorts, respectively. Low-risk group showed significantly better median RFS than that of the high-risk group, which was also confirmed in cohort V1 and V2.
Impact: TLSs have been reported to have prognostic value and guiding significance to immunotherapy in ICC patients. The MRI radiomics signature could serve as a non-invasive tool to preoperatively predict intra-tumoural TLSs status of ICC patients and correlate significantly with prognosis.
Objective
To predict the tertiary lymphoid structures (TLSs) status and recurrence-free survival (RFS) of patients with intrahepatic cholangiocarcinoma (ICC) using preoperative magnetic resonance imaging (MRI) texture analysis.Methods
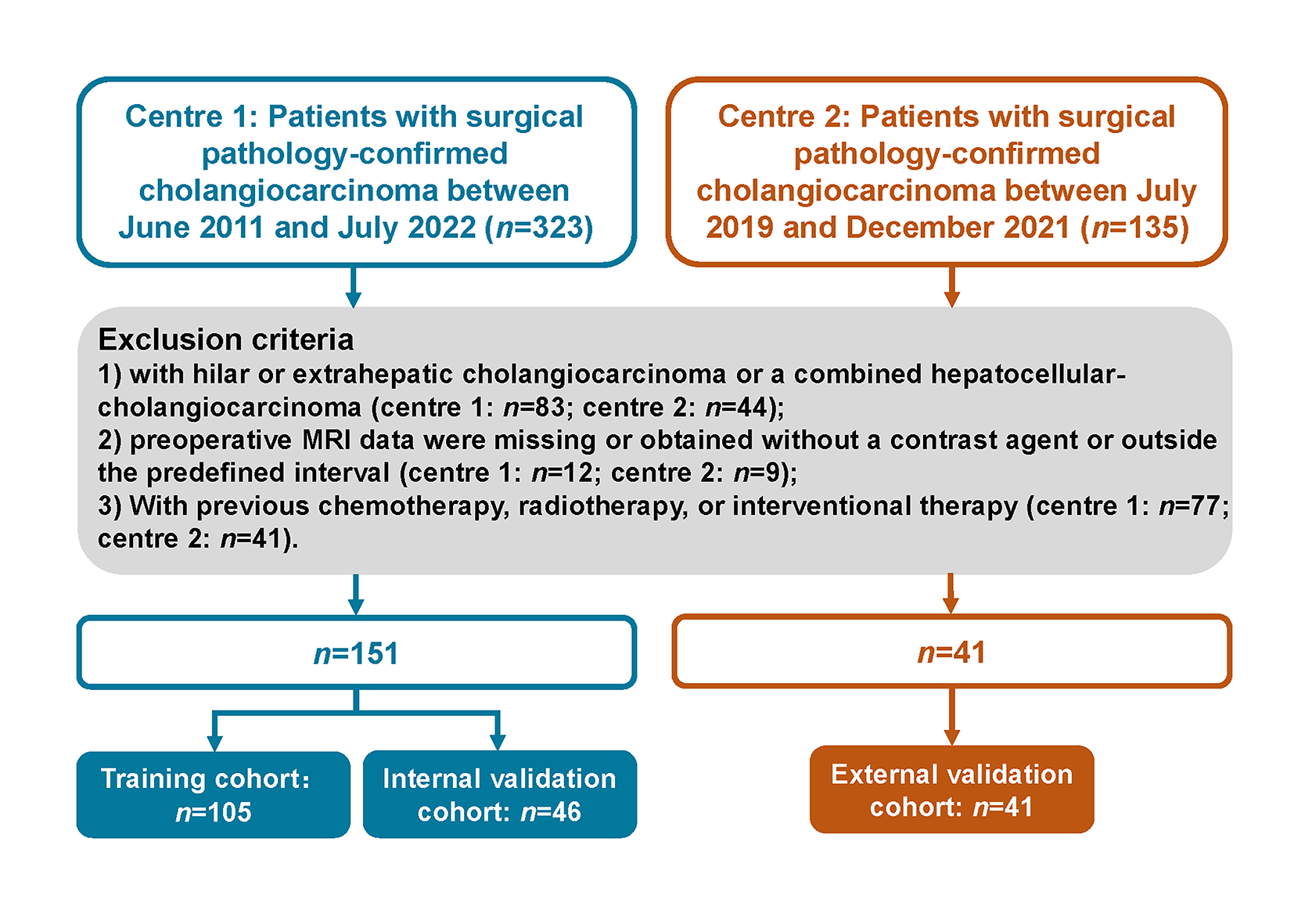
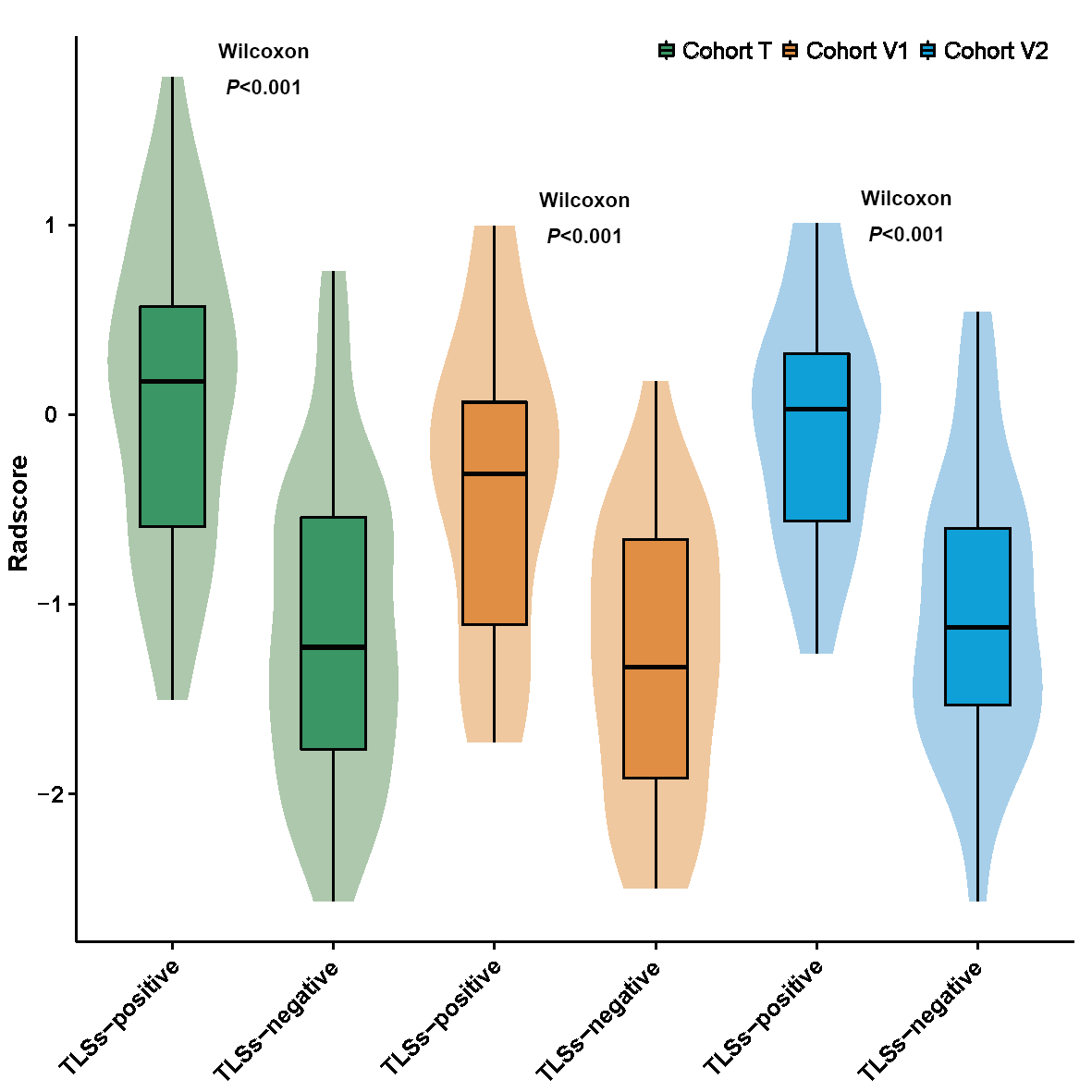
A total of 192 ICC patients were divided into training (T = 105), internal validation (V1 = 46), and external validation groups (V2 = 41). Three MRI sequences were performed with texture analysis. Radiomics score was calculated to predict the TLSs status and stratify ICC into high- and low-risk groups. Logistic regression was applied to select the significant clinico-radiological features related to TLS status. The performance was compared with receiver operating characteristic curve (ROC).Results
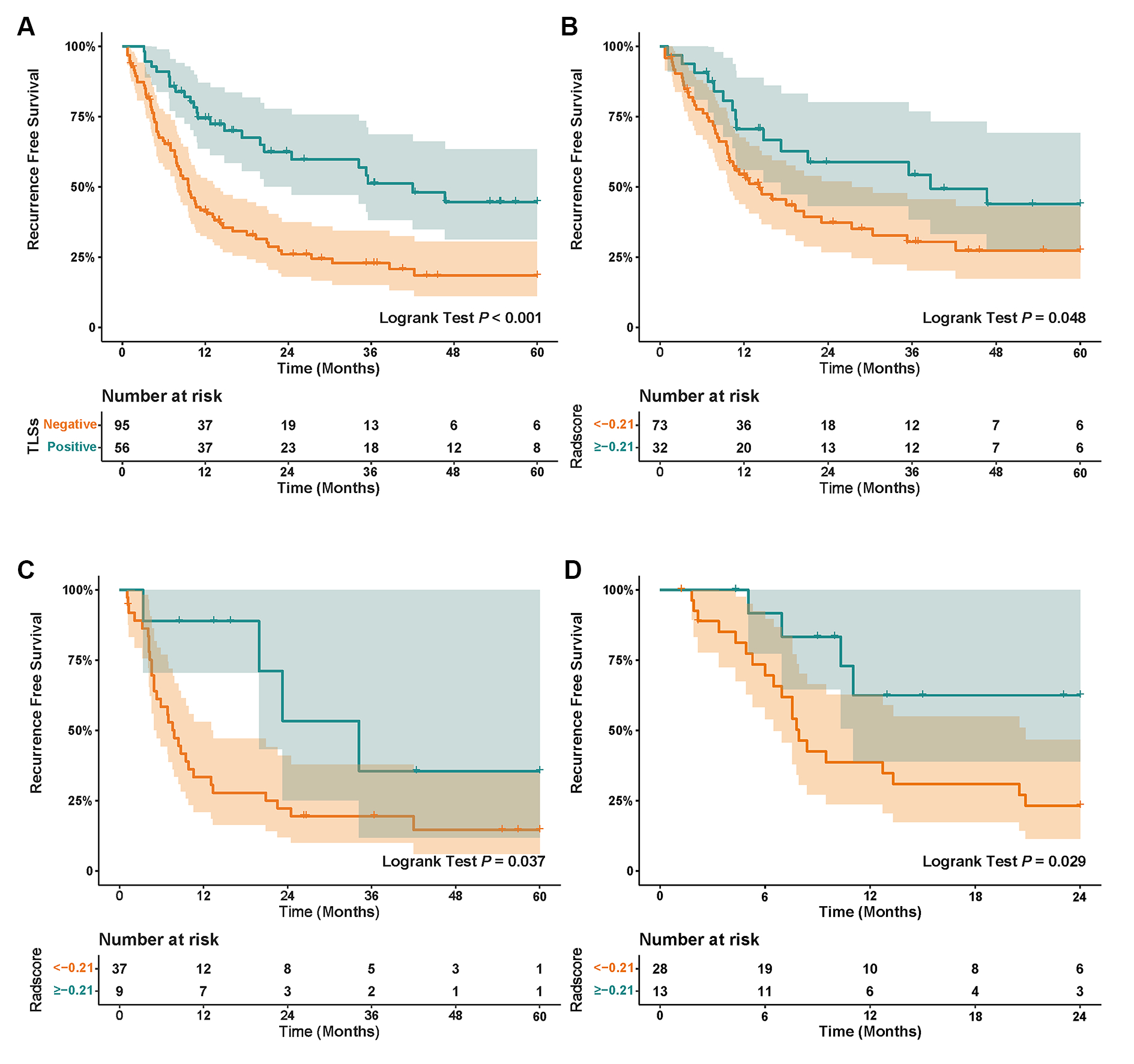
The AUCs of arterial phase diffuse hyperenhancement were 0.59 (95% CIs, 0.50–0.67), 0.52 (95% CIs, 0.43–0.61), and 0.66 (95% CIs, 0.52–0.80) in the T, V1, and V2 cohorts. Eleven features were combined to establish the Rad-score with an AUC of 0.85 (95% CIs, 0.77–0.92), 0.81 (95% CIs, 0.67–0.94), and 0.84 (95% CIs, 0.71–0.96) in the T, V1, and V2 cohorts, respectively. The median RFS of the low-risk group with a Rad-score cut-off less than −0.21 was 38.7 months (95% CIs, 5.4–71.9 months), which was better than that of the high-risk group (median RFS: 14.1 months; 95% CIs, 7.0–21.2 months) (p = 0.048). This was also confirmed in cohort V1 and cohort V2.Conclusion
The MRI radiomics signature could serve as a better preoperatively predictive biomarker of the intra-tumoural TLSs status and survival of ICC patients than MRI imaging features.Acknowledgements
None.References
[1] Bertuccio P, Malvezzi M, Carioli G et al (2019) Global trends in mortality from intrahepatic and extrahepatic cholangiocarcinoma. J Hepatol 71:104-114 2
[2] Forner A, Vidili G, Rengo M, Bujanda L, Ponz-Sarvise M, Lamarca A (2019) Clinical presentation, diagnosis and staging of cholangiocarcinoma. Liver Int 39 Suppl 1:98-107 3
[3] Banales JM, Cardinale V, Carpino G et al (2016) Expert consensus document: Cholangiocarcinoma: current knowledge and future perspectives consensus statement from the European Network for the Study of Cholangiocarcinoma (ENS-CCA). Nat Rev Gastroenterol Hepatol 13:261-280 4
[4] Lin J, Dai Y, Sang C et al (2022) Multimodule characterization of immune subgroups in intrahepatic cholangiocarcinoma reveals distinct therapeutic vulnerabilities. J Immunother Cancer 10 5 Doussot A, Groot-Koerkamp B, Wiggers JK et al (2015) Outcomes after Resection of Intrahepatic Cholangiocarcinoma: External Validation and Comparison of Prognostic Models. J Am Coll Surg 221:452-461 6
[5] Lang H, Sotiropoulos GC, Fruhauf NR et al (2005) Extended hepatectomy for intrahepatic cholangiocellular carcinoma (ICC): when is it worthwhile? Single center experience with 27 resections in 50 patients over a 5-year period. Ann Surg 241:134-143 7
Figures