3609
Multiparametric MRI based deep learning model for automatic segmentation of tumor and lymph nodes in rectal cancer1Department of Radiology, Ruijin Hospital, Shanghai Jiao Tong University of Medicine, shanghai, China, 2MR Research, GE Healthcare, Beijing, China
Synopsis
Keywords: Diagnosis/Prediction, Segmentation
Motivation: A significant challenge in RC management is the precise delineation of tumor boundaries and the accurate evaluation of LNs. The existing manual processes for this are time-consuming and subject to high variability.
Goal(s): This study aimed to develop a deep learning approach for simultaneous RC tumor and LN segmentation.
Approach: We constructed the model with mpMRI data input, ResUNet architecture, and focal cross entropy loss.
Results: The ResUNet model achieved a mean SEN of 0.824, PRE of 0.619, and DSC of 0.694 in the validation dataset, indicating promising results. However, some false positives and false negatives were observed in LN segmentation.
Impact: We introduced a ResUNet model for RC segmentation and achieved satisfactory results. While our findings are preliminary and may benefit from larger samples, this approach could improve tumor and LN segmentation and ultimately enhance clinical utility in RC management.
Introduction
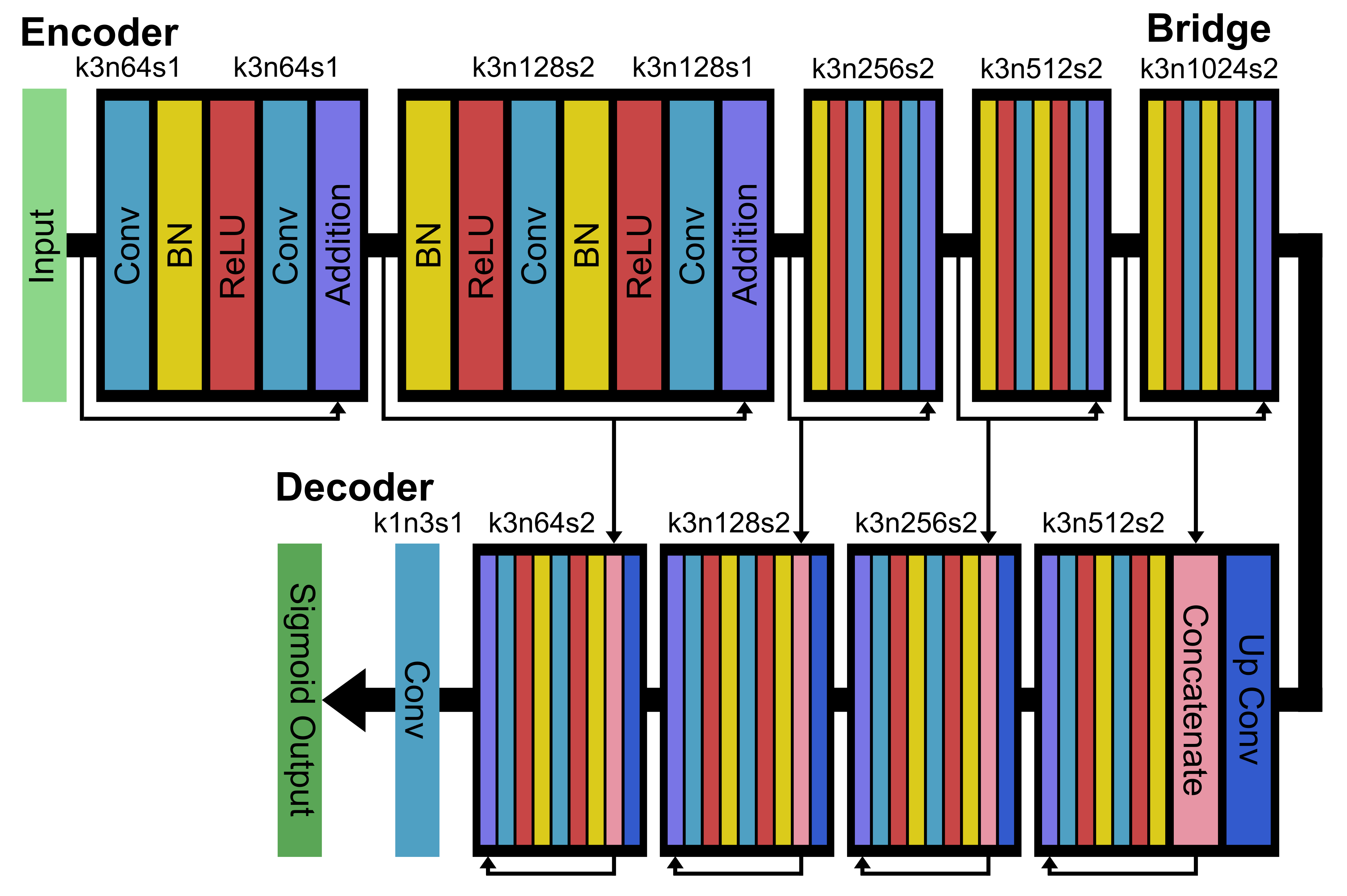
Rectal cancer (RC) ranks among the most prevalent malignancies in the gastrointestinal system. Presently, MRI has emerged as a crucial tool for both the diagnosis and treatment of RC patients1. The determination of tumor volume holds significant importance in various aspects of cancer therapy2,3. The current gold standard for delineating tumor boundaries involves manual processes, which are time-consuming, labor-intensive, and has high interobserver variation4-6. Additionally, lymph nodes (LNs) play a pivotal role in the metastasis of RC, making their accurate evaluation critical for treatment decisions and prognosis assessment7. Multiparametric MRI (mpMRI) has emerged as the primary tool for RC evaluation. Due to the absence of clear distinctions between LNs and neighboring structures and individual anatomy variations, existing studies have highlighted challenges of accurately detecting small LNs8,9. Consequently, automatic and precise pre-surgery identification of the primary tumor and metastatic LNs become crucial. Deep learning techniques have been utilized to performed such tasks, by using UNet with dice loss10 and RCNN with cross entropy loss11 for RC tumor and LN segmentation, respectively. In this study, we used mpMRI including T2WI and high-resolution multi-shot MUSE DWI data as input, and developed a deep ResUNet model with focal cross entropy loss for simultaneous RC tumor and LN segmentation. We hypothesize that by optimizing the input data with high-resolution diffusion, deep learning model with deep UNet architecture with residual block implementation, and loss function with a stable and focal loss calculation, we can improve the performance of automatic segmentation for RC tumor and LNs of varying sizes and locations.Materials and Methods
This retrospective study was approved by the Ethics Committee of our hospital. Data from 45 pathologically confirmed RC patients were included. Rectum MRI examinations were performed on a 3.0T MRI scanner (SIGNA Architect, GE Healthcare, Milwaukee, WI). T2WI and MUSE DWI images were acquired with following parameters: (1) T2WI: TR/TE = 9403/184 ms, FOV = 240 x 240 mm, matrix = 420 x 300, slice thickness = 3 mm, NEX = 2; (2) MUSE DWI: TR/TE = 4930/78 ms, FOV = 280 x 280 mm, matrix = 160 x 96, slice thickness = 3.6 mm, number of shot = 2, NEX = 2, b-value = 0 and 1000 s/mm2. Data were randomly divided into training and validation dataset at an 8:2 ratio. For image preprocessing, we first performed a rigid registration between T2WI and MUSE DWI images, and all images were resampled into the same matrix size. Subsequently, data were augmented by random cropping, flipping, and rotating, resulting in a total of 11325 patches in the training dataset. Architecture of the ResUNet is shown in Figure 1. The input images consisted of 3 channels (T2WI, MUSE DWI b0, and MUSE DWI b1000). For the optimization we used a focal cross entropy as loss function, and adopted Adam optimizer with a learning rate of 10-5. The batch size was set at 16 and the total number of epochs was set at 100. The network was trained and evaluated using TensorFlow with two NVIDIA Quadro GV100 GPUs. The segmentation performance was evaluated by mean sensitivity (SEN), precision (PRE), and dice score (DSC).Results
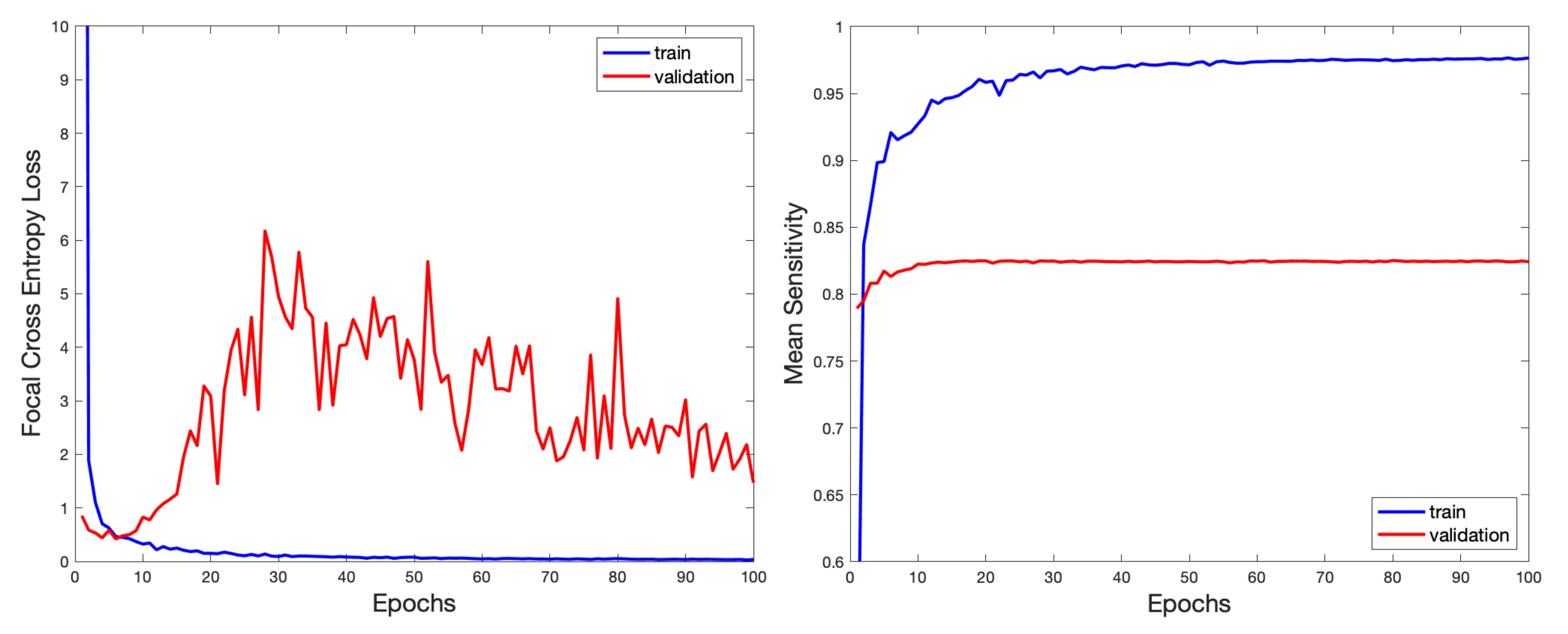
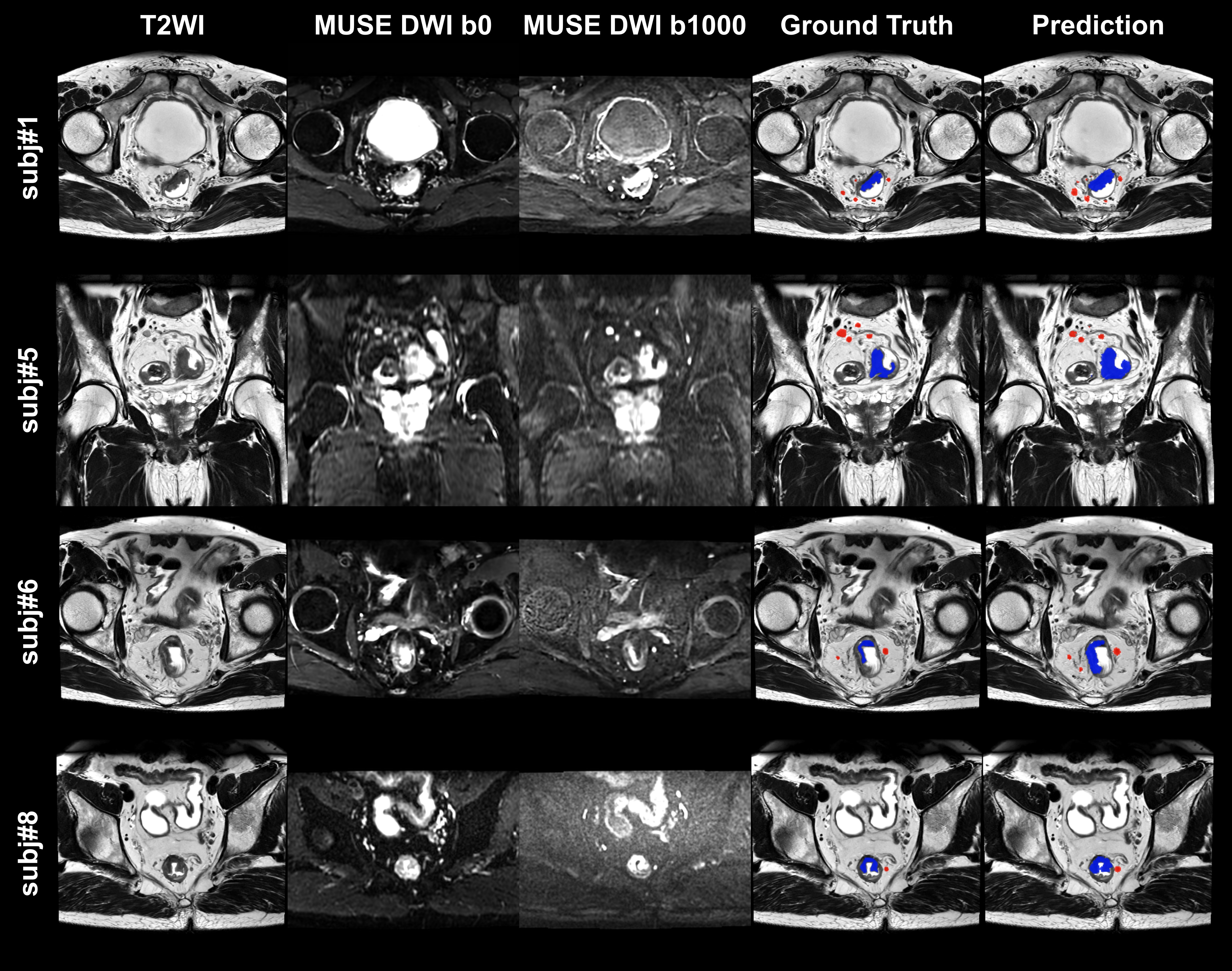
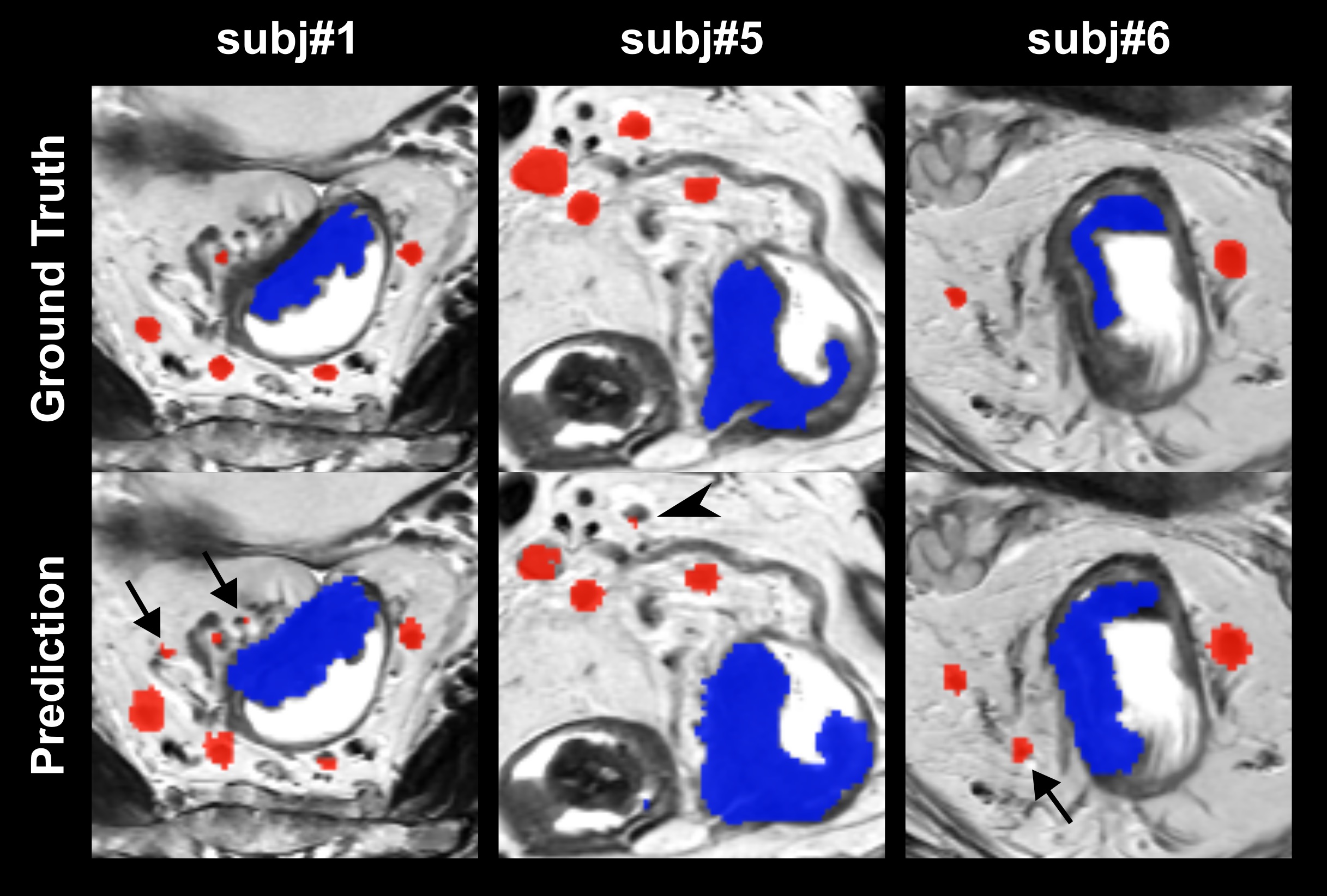
The training took 10 hours, and the inference of validation for single slice took 24 ms. Figure 2 shows the mean focal cross entropy loss and mean SEN of the training and validation dataset during the training process. A reasonable convergence is steadily reached, while certain underfitting is observed. Figure 3 demonstrated the input T2WI, MUSE DWI b0, MUSE DWI b1000 images, ground truth labels, and predicted labels from 4 representative participants in the validation dataset. Overall, the proposed ResUNet achieved SEN, PRE, and DSC of 0.977, 0.700, and 0.800 in the training dataset, and 0.824, 0.619, and 0.694 in the validation dataset, respectively. Figure 4 displays enlarged ground truth labels and predicted labels overlaid on top of T2WI images. The results exhibited that our predicted labels had a generally larger area than ground truth labels. While the segmentation of tumor presented satisfactory results, a number of false positive (arrow) and a few false negative predictions (arrow head) of LN were found.Discussion
In this study, we developed an optimized deep learning model with mpMRI inputs, ResUNet framework, and focal cross entropy loss for simultaneous segmentation of RC tumor and LNs. Our preliminary findings demonstrated that our proposed model achieved a satisfactory segmentation for RC tumor and large LNs. Although results were suboptimal, potentially due to limited samples, further studies with a larger sample size from multicenter might improve model performance and clinical utility.Acknowledgements
NoneReferences
1. Zhang K, Yang X, Cui Y, et al. Automatic segmentation of rectal tumors from MRI using multiscale densely connected convolutional neural networks based on attention mechanisms. Phys Med Biol. 2023; 68(16).2. Gurney-Champion OJ, Mahmood F, van Schie M, et al. Quantitative imaging for radiotherapy purposes. Radiother Oncol. 2020; 146:66-75.
3. de Jong R, Crama KF, Visser J, van Wieringen N, Wiersma J, Geijsen ED, et al. Online adaptive radiotherapy compared to plan selection for rectal cancer: quantifying the benefit. Radiat Oncol. 2020; 15:162.
4. Trebeschi S, van Griethuysen JJM, Lambregts DMJ, et al. Deep learning for fully-automated localization and segmentation of rectal cancer on multiparametric MR. Sci Rep. 2017; 7(1):5301.
5. Irving B, Franklin JM, Papiez BW, et al. Pieces-of-parts for supervoxel segmentation with global context: application to DCE-MRI tumour delineation. Med Image Anal. 2016; 32:69-83.
6. Hearn N, Bugg W, Chan A, et al. Manual and semi-automated delineation of locally advanced rectal cancer subvolumes with diffusion-weighted MRI. Br J Radiol. 2020; 93(1114):20200543.
7. Harisinghani MG and Weissleder R. Sensitive, Noninvasive Detection of Lymph Node Metastases. PLoS Med. 2004; 1:e66.
8. Grone J, Loch FN, Taupitz M, et al. Accuracy of various lymph node staging criteria in rectal cancer with magnetic resonance imaging. J Gastrointest Surg Off J Soc Surg Aliment Tract. 2018; 22:146-53.
9. Langman G, Patel A, Bowley DM. Size and distribution of lymph nodes in rectal cancer resection specimens. Dis Colon Rectum. 2015; 58:406-14.
10. Knuth F, Adde IA, Huynh BN, et al. MRI-based automatic segmentation of rectal cancer using 2D U-Net on two independent cohorts. Acta Oncol. 2021;61(2):255-263.
11. Zhao X, Xie P, Wang M, et al. Deep learning-based fully automated detection and segmentation of lymph nodes on multiparametric mri for rectal cancer: A multicentre study. EBioMedicine. 2020; 56:102780.
Figures