3606
Cervical cancer diagnosis from diffusion weighted imaging using deep convolutional neural networks1Radiation Oncology, National Center for Cancer Care and Research, Doha, Qatar, 2Electrical and Computing Engineering, Texas A&M University at Qatar, Doha, Qatar, 3Brain Mapping Foundation, Los Angeles, CA, United States
Synopsis
Keywords: Diagnosis/Prediction, Cancer, deep learning, diffusion weighted imaging, cervix cancer, grade, stage
Motivation: Conventional grading of cervix cancer (CC) requires biopsy that can lead to potential side-effects. Radiologists typically rely on multi-imaging for CC staging, which can result in patient discomfort, higher costs, and increased workload.
Goal(s): This study aims to introduce noninvasive methods that leverage a single MRI for both grading and staging prediction.
Approach: EfficientNetB0 and EfficientNetB3 were applied for tumor classification (binary and four-class) based on apparent diffusion coefficient maps of 85 patients. They were evaluated using the area under the receiver operating characteristic curve (AUC).
Results: High AUC=0.924 and AUC=0.931 were obtained for grade and stage predictions respectively.
Impact: The results demonstrated the feasibility of noninvasive prediction of cervical cancer grade and stage from diffusion weighted images. This could significantly impact the diagnosis and management of cervical cancer, as it can provide valuable information without biopsy or extensive imaging.
Introduction
Conventional grading of cervix cancer (CC) is an invasive procedure that can lead to potential side-effects and is prone to errors as it doesn’t consider the 3D heterogeneity of the tumor. Radiologists typically rely on multiple MR sequences for CC staging, which can result in patient discomfort, higher costs, and increased workload. This study aims to introduce an innovative noninvasive method that leverages a single image for both grading and staging prediction. The grade and the stage of CC are determined from diffusion-weighted imaging (DWI) in particular apparent diffusion coefficient (ADC) mapping using deep convolutional neural networks (DCNN).Methods
Datasets composed of 85 patients having annotated tumor stage (I, II, III, and IV), out of this, 66 were with grade (II and III) and the remaining patients with no reported grade were retrospectively collected. The study was IRB approved (protocol number MRC-01-19-002). For each patient, sagittal and axial slices containing the gross tumor volume (GTV) were reconstructed from ADC maps. These were computed using the mono exponential model from diffusion weighted images (b-values =0, 100, 1000) that were acquired using GE 1.5T Optima 450w MR scanner prior to external beam radiotherapy treatment. Balanced training sets were created using the Synthetic Minority Oversampling Technique (SMOTE) and fed to the DCNN. EfficientNet methods(1) that scale uniformly each network dimension with a fixed set of scaling coefficients to improve the performance with respect to the available resources were used. EfficientNetB0 and EfficientNetB3 were first pretrained on the ImageNet dataset and then adapted to binary (grade) and four classes (stage) classification tasks using transfer learning. A classification head was appended to the base model (EfficientNetB0/B3). For tumor grading, the classification head included a fully connected layer with a single neuron and a sigmoid activation function whereas, for tumor staging, a dense layer with softmax activation and an output dimensionality of four were used.Five-fold stratified cross validation was performed for the assessment of the networks. Multiple evaluation metrics were computed including the accuracy (ACC), the balanced accuracy (b-ACC), the precision (PR), the recall (RE), the F1-score (F1) and the area under the receiver operating characteristic curve (AUC). The confusion matrix C was, also, computed; each coefficient Cij is equal to the percentage of observations known to be in class i and predicted to be in class j.
Results
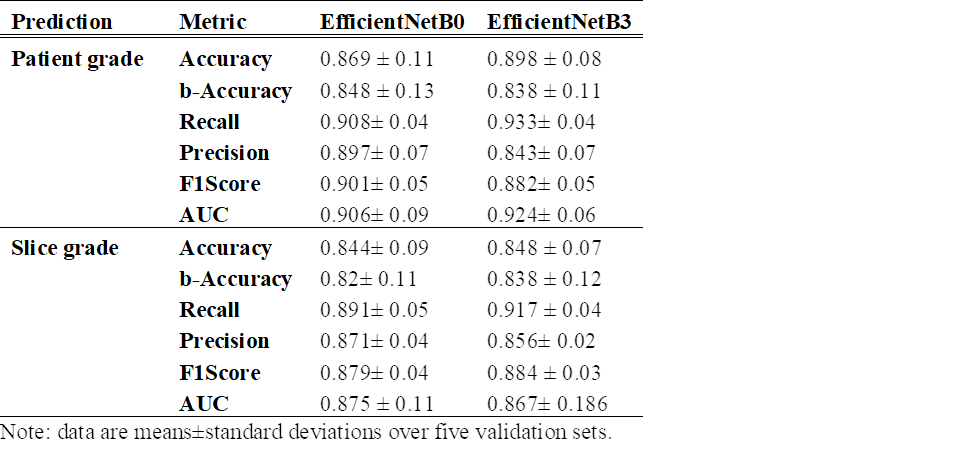
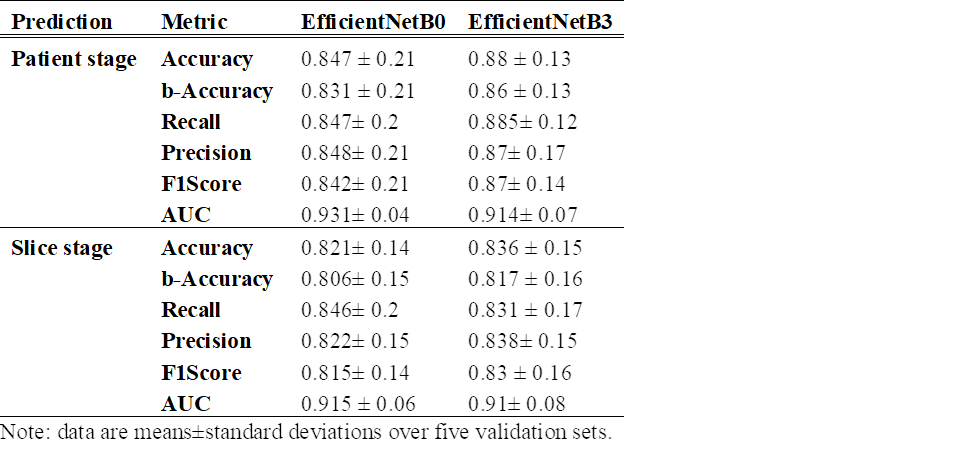
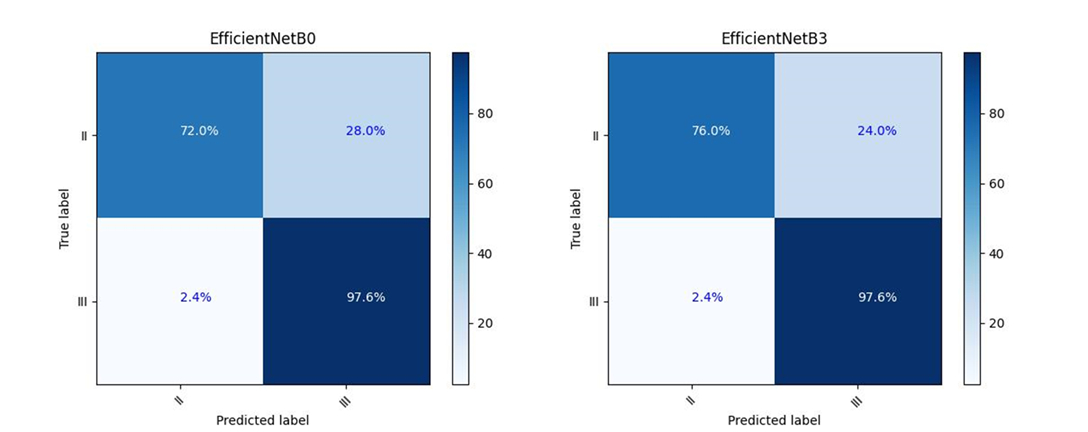
Table 1 and table 2 display the average and standard deviation values of ACC, b-ACC, PR, RE, F1 obtained using transfer learning approaches that are based on EfficientNetB0 and EfficientNetB3 for grade and stage prediction respectively. The metrics were calculated for the prediction of slice grade/stage and patient grade/stage. Both classification approaches gave good results with an accuracy of 89.8% (86.9%) and an AUC of 92.4% (90.6%) with EfficientNetB3 (EfficientNetB0) for grade prediction. For the prediction of the stage, the metrics were above 86% and 83% for EfficientNetB3 and EfficientNetB0 respectively. Figure 1 and figure 2 show the confusion matrices obtained for grade and stage predictions respectively with good discriminative ability (Cii > 72%) by both methods except for stage I (C00 > 50%).Discussion
DCNN gave good results for the prediction of CC grade and stage. In the literature, radiomic analysis was mainly combined with the use of DWI and AUC ranged from 0.71 to 0.95 (2–4). We tested the radiomic analysis approaches described in (5) but the results were not as promising as DCNN; AUC =0.67 and AUC=0.66 for grade and stage prediction respectively were obtained.The main limitation of this work is being a single center study with the small sample size of 85 patients although data augmentation, transfer learning and SMOTE were applied to remedy to this. Further improvement could be a multi-center validation of the methods.
Conclusion
DCNN are promising techniques for the grading and staging of cervix cancer using DWI. Further validation on datasets from different centers will be necessary before clinical implementation.Acknowledgements
The authors are grateful to Texas A&M at Qatar for the use of the supercomputer.References
1. Tan M, Le Q V. EfficientNet: Rethinking Model Scaling for Convolutional Neural Networks. Int Conf Mach Learn [Internet]. 2019 May 28;6105–14. Available from: http://arxiv.org/abs/1905.11946
2. Yamada I, Oshima N, Miyasaka N, Wakana K, Wakabayashi A, Sakamoto J, et al. Texture Analysis of Apparent Diffusion Coefficient Maps in Cervical Carcinoma: Correlation with Histopathologic Findings and Prognosis. Radiol Imaging Cancer [Internet]. 2020 May 1;2(3):e190085. Available from: http://pubs.rsna.org/doi/10.1148/rycan.2020190085
3. Jajodia A, Gupta A, Prosch H, Mayerhoefer M, Mitra S, Pasricha S, et al. Combination of Radiomics and Machine Learning with Diffusion-Weighted MR Imaging for Clinical Outcome Prognostication in Cervical Cancer. Tomography [Internet]. 2021 Aug 5;7(3):344–57. Available from: https://www.mdpi.com/2379-139X/7/3/31
4. Becker AS, Ghafoor S, Marcon M, Perucho JA, Wurnig MC, Wagner MW, et al. MRI texture features may predict differentiation and nodal stage of cervical cancer: a pilot study. Acta Radiol Open [Internet]. 2017 Oct 17;6(10):205846011772957. Available from: http://journals.sagepub.com/doi/10.1177/2058460117729574
5. Aouadi S, Torfeh T, Yoganathan S, Paloor S, Riyas M, Hammoud R, et al. Investigation of radiomics and deep convolutional neural networks approaches for glioma grading. Biomed Phys Eng Express [Internet]. 2023;9(3):35020. Available from: http://dx.doi.org/10.1088/2057-1976/acc33a
Figures