3603
MRI-based Radiomics Nomogram in Preoperative Prediction of Lymph Node Metastasis of Endometrial Cance1Women's Hospital of Nanjing Medical University, Nanjing Maternity and Child Health Care Hospital, Nanjing, China, 2GE Healthcare, MR Research China, Beijing, China
Synopsis
Keywords: Diagnosis/Prediction, Uterus, endometrial cancer; lymph node; nomogram
Motivation: Routinely MRI can’t assess lymph node metastasis (LNM) status in endometrial cancer (EC) accurately.
Goal(s): This study aimed to investigate whether the MRI radiomics model can predict LNM status in EC.
Approach: 313 EC patients who underwent preoperative MRI were recruited with the status of LNM confirmed by pathology. 2880 radiomic features were extracted and three models including a clinical model, a radiomics model and a combined model were built.
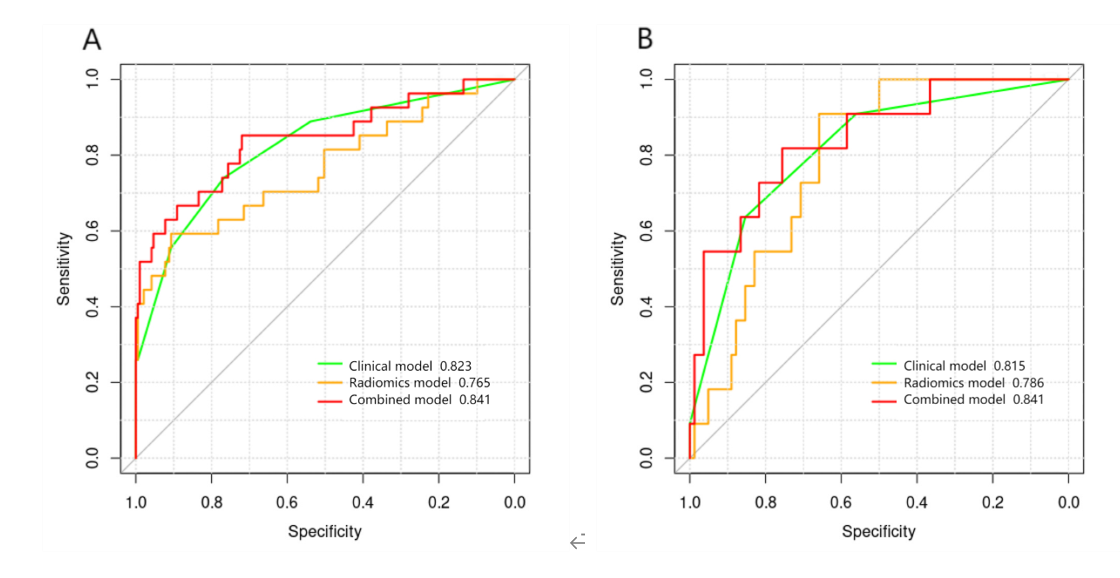
Results: Area under the receiver operating characteristic curves showed all of the three models can predict LNM and the combined model showed the best discrimination ability on the training set and test set.
Impact: This study built an accurate preoperative and non-invasive model to assess lymph node metastasis status in endometrial cancer. It could help doctors to determine the extent of lymphadenectomy and provide useful information for prognosis prediction and treatment decision.
Introduction
Lymph node metastasis (LNM) is an important adverse prognostic factor affecting treatment strategy and prognosis for endometrial cancer (EC) patients[1]. Lymphadenectomy, which can help in surgical staging and guide adjuvant therapy decisions[2], is controversial in the clinic[3]. Therefore, preoperative non-invasive assessment of lymph node status is crucial for EC patients to receive accurate medical treatment.Routinely, MR images have low accuracy[4]. Radiomics can extract high-dimensional quantitative features from images and select reliable features to establish predictive models that could be used in computer-assisted decision support[5]. Some studies have shown that radiomics has the potential to predict recurrence, metastasis, and survival time[6].Therefore, the main goal of this study was to investigate if MRI-based radiomics was feasible for predicting LNM of EC preoperatively and to build a model combining clinical factors and MRI-based radiomic factors to assess lymph node status for assisting lymphadenectomy decisions preoperatively.Materials and Methods
SubjectsA total of 313 patients were recruited for the study, including LNM-positive patients (n=38, mean age 54 years, ranging from 44-76 years) and LNM-negative patients (n=275, mean age 57 years, ranging from 30-74 years). All patients were confirmed by pathological analyses after surgery.
MRI acquisition
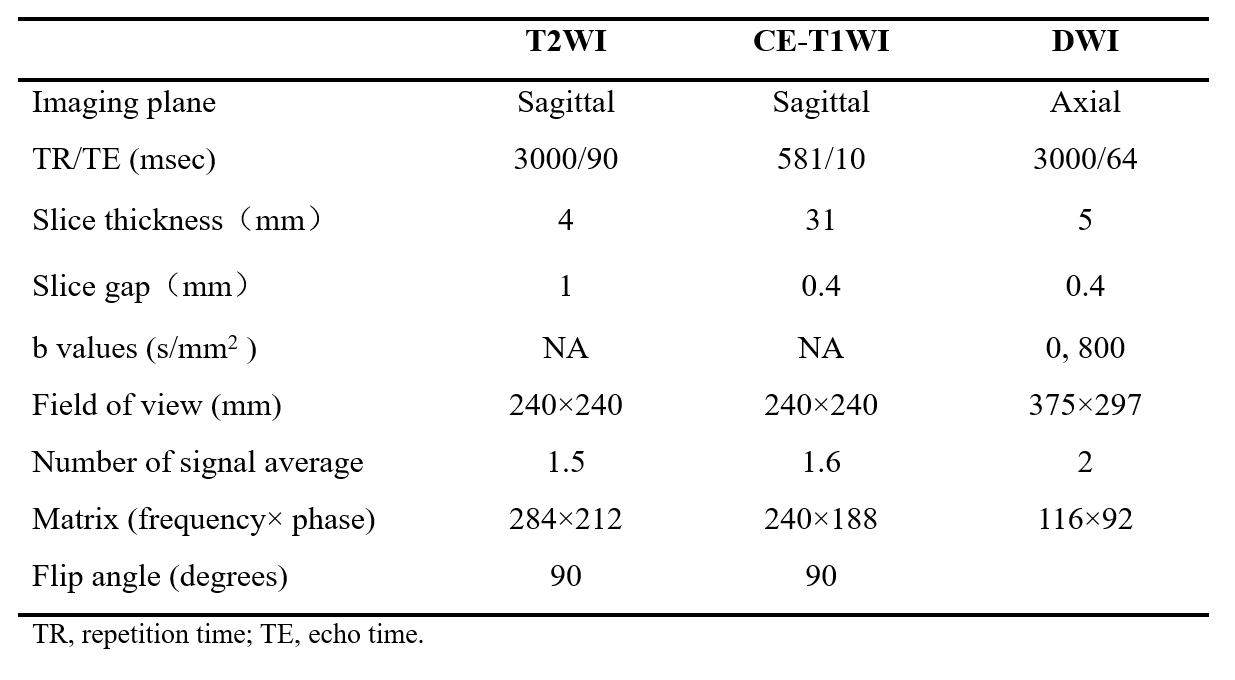
All MRI experiments were performed on a 1.5T MR scanner (Achieva 1.5 T, Philips Healthcare, Netherlands) using a 16-channel phased-array surface coil. T2-weighted imaging (T2WI), DW imaging (b values of 0 and 800 s/mm²), and delayed contrast-enhanced T1-weighted imaging (CE-T1WI) were obtained. The parameters of some MRI sequences are showed in Table 1.
Image and data analysis
Clinical parameters were collected, including age, menopause, CA125 level, HE4 level, depth of myometrial invasion (DMI), and lymph node (LN) status. Tumor size, myometrial invasion, and size of lymph nodes were measured retrospectively on MRI by two doctors independently.The 313 patients were randomly divided into a training set and a test set in a 7:3 ratio. Using ITK-SNAP (open source software; www.itk-snap.org), tumor volume of interest (VOI) was manually delineated layer by layer, avoiding normal endometrial tissue, focal bleeding, and cystic changes. Two months later, 20 patient images were randomly selected for redrawing, and another doctor was invited to do the same redraw. Features were selected by the inter-correlation coefficient (ICC) and Pearson test in the training set for stable models. Then, a binary least absolute shrinkage and selection operator (LASSO) logistic regression analysis with 10-fold cross-validation was finally used to select the radiomics features and generate a radiomics signature. A nomogram model was established by combining the significant clinical indicators with radiomics. The models were verified in the test set.
Statistical analysis
In this study, statistical analysis programs were completed using SPSS (version 23.0) and R software (version 4.05, http://www.Rproject.org). All statistical hypothesis tests were two-sided, and p-values < 0.05 were considered significant.
Results
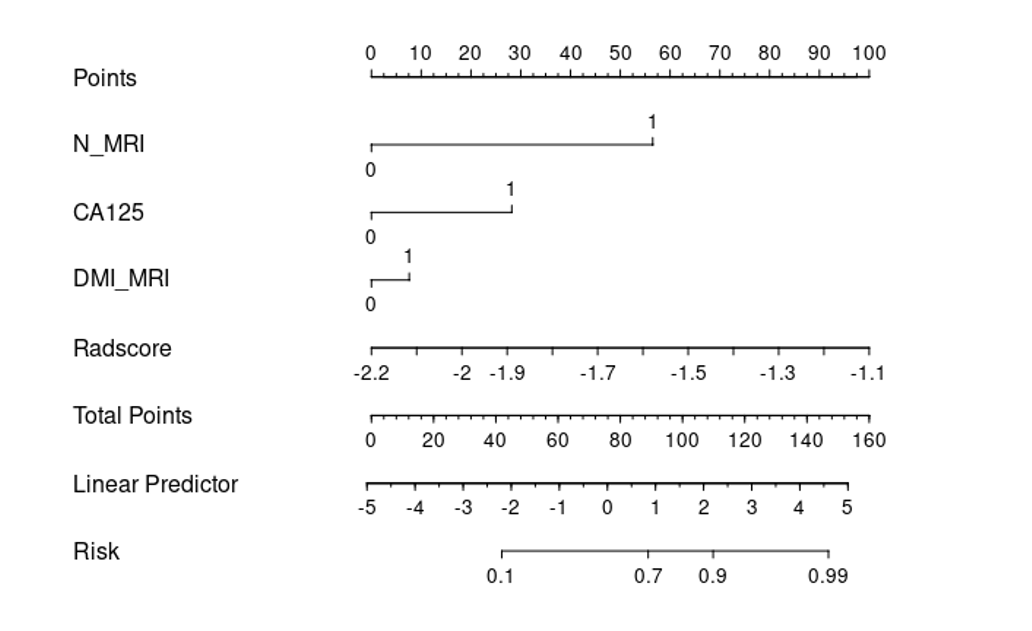
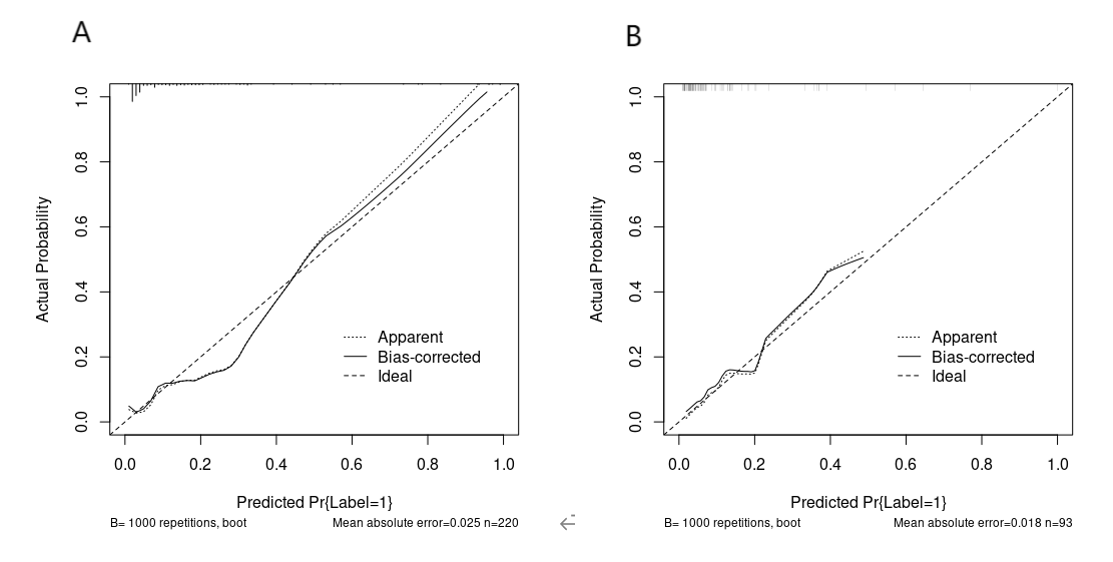
In the radiomics model, three radiomic features were used to build the prediction model. In the clinical model, clinical parameters (CA125, LN size, and DMI) were used to build the prediction model. In the combined model, five risk factors, including three clinical parameters (CA125, LN size, and DMI), and three radiomic features were used to build the prediction model. Performances of the three models in the training and test set are shown in Figures 1. The AUC of this radiomics signature was 0.765 [95% confidence interval [CI]: 0.651-0.878] in the training set, and that in the test set was 0.786 [95% confidence interval [CI]: 0.677-0.895]. The combined model showed a significant ability in predicting LNM with an AUC of 0.841 [95% confidence interval [CI]: 0.745-0.937] in the training set and an AUC of 0.841 [95% confidence interval [CI]: 0.714-0.969] in the test set. A nomogram (Figure 2) was established for the combined model. The sensitivity of the nomogram model was highest in the training set and test set among the models, with sensitivities of 85.2% and 72.7%, respectively. Calibration curves showed a high accuracy of the radiomics nomogram for predicting lymph node metastasis in the primary group and validation groups (Figure 3).Conclusion
Multi-sequence MRI radiomics models could predict EC lymph node metastasis, and the combined nomogram model, combining CA125 level, MRI lymph node size, and MRI myometrial invasion, can effectively predict EC lymph node metastasis before surgery. The nomogram model provided a more detailed preoperative risk assessment for patients and may enable the clinical implementation of targeted surgery strategies.Acknowledgements
No acknowledgement found.References
[1] Koppikar S, Oaknin A, Babu KG, et al. Pan-Asian adapted ESMO Clinical Practice Guidelines for the diagnosis, treatment and follow-up of patients with endometrial cancer. ESMO Open. 2023. 8(1): 100774.
[2] Marchocki Z, Cusimano MC, Ferguson SE. Sentinel lymph node biopsy in high-grade endometrial cancer. Am J Obstet Gynecol. 2022. 226(6): 867-868.
[3] Pahk K, Ryu KJ, Joung C, et al. Metabolic Activity of Visceral Adipose Tissue Is Associated with Metastatic Status of Lymph Nodes in Endometrial Cancer: A (18)F-FDG PET/CT Study. Int J Environ Res Public Health. 2021. 19(1): 92.
[4] Nougaret S, Horta M, Sala E, et al. Endometrial Cancer MRI staging: Updated Guidelines of the European Society of Urogenital Radiology. Eur Radiol. 2019. 29(2): 792-805.
[5] Mayerhoefer ME, Materka A, Langs G, et al. Introduction to Radiomics. J Nucl Med. 2020;61(4):488-495.
[6] Li G, Li L, Li Y, et al. An MRI radiomics approach to predict survival and tumour-infiltrating macrophages in gliomas. Brain. 2022. 145(3): 1151-1161.
Figures