3602
Highly Accelerated DCE-MRI Analysis with Deep Learning and Dispersion-applied AIFs1Radiological Sciences, University of California, Los Angeles, Los Angeles, CA, United States
Synopsis
Keywords: Diagnosis/Prediction, DSC & DCE Perfusion, Prostate, DCE
Motivation: Existing techniques for DCE-MRI analysis is time-consuming and often assume a fixed arterial input function (AIF) across various locations and patients, leading to imprecise outcomes.
Goal(s): 1) The development of a Deep learning model for fast DCE-MRI analysis, and 2) the design of location- and patient-specific AIFs.
Approach: We use deep-learning model for fast DCE-MRI analysis, and propose to represent dispersion-applied AIF to allow for location- and subject-specific AIFs by interpolation between constant AIFs.
Results: 1) Reduced per-patient processing time by one-tenth, 2) improved fitting accuracy, and 3) higher-contrast parameteric maps between the lesion and normal tisue.
Impact: Other scientists, clinicians and patients may benefit from the faster processing time, and higher-contrast parametric maps for cancer diagnosis.
Introduction
Dynamic contrast-enhanced (DCE) magnetic resonance imagingMRI (DCE-MRI) allows the estimation of the permeability- and perfusion-related pharmacokinetic (PK) parameters, shown to be useful in various oncology applications.Conventional approaches for PK parameter estimation use time-consuming voxel-wise curve fitting and often assume a constant fixed population-based arterial input function (AIF), e.g., the Weinmann[1] or Parker[2], leading to inaccurate estimation[3]. Accelerating and enabling flexible AIFs are essential in DCE-MRI analysis.
In this study, we first proposed a deep-learning-based model to directly estimate PK parameters from the data without time-consuming curve fitting. Then, we proposed an efficient way of representing dispersion-applied AIFs by simply linear combination of the Weinmann and Parker AIFs. Our method enables patient- and location-specific AIFs and improves the accuracy of PK modeling. Moreover, the combination factor could be used as another indicator of the tumor and improve the distinction between tumor and healthy tissue.
Method
The Tofts model[4] is widely used in DCE-MRI PK modeling. In Tofts model, the tissue enhancement $$$C_t(t)$$$ is represented as the convolution between AIF $$$C_p(t)$$$ and tissue pulse response: $$C_t(t) = \int_0^t C_p(\tau) \cdot K^{trans}e^{-k_{ep} \cdot (t-\tau)} d\tau,$$ where $$$K^{trans}$$$ (volume transfer constant) and $$$k_{ep}$$$ are PK parameters to be determined. The AIF is often assumed to be fixed among different tissue and patients. To allow flexible AIF, we extend the Tofts model through thecharacterization of various AIFs by including a parameter related to intravascular dispersion and permeability. $$C_t(t) = \int_0^t \Big(\beta C_p^1 + (1-\beta) C_p^2\Big) \cdot K^{trans} e^{-k_{ep} (t-\tau)} d\tau, $$Where $$$C_p^1$$$ and $$$C_p^2$$$ are the Weinmann and Parker AIFs and $$$\beta$$$ is the new parameter controlling the linear combination. We combine $$$\beta$$$ and $$$K^{trans}$$$ as the "beta $$$K^{trans}$$$" which is defined as:$$
beta K^{trans} = K^{trans} \cdot e^{\beta}
$$
We trained a Transformer-based neural network to directly estimate $$$K^{trans}$$$, $$$k_{ep}$$$ and $$$\beta$$$ from the enhancement $$$C_t(t)$$$. Our model was trained with synthetic data and no data acquisition and annotation is required in training. Specifically, we randomly sampled $$$K^{trans}$$$, $$$k_{ep}$$$ and $$$\beta$$$ and then synthesize enhancement $$$C_t(t)$$$ with the extended model. Noise is added to the synthetic curves to simulate real acquired data. After training, our model efficiently estimates PK parameters from the data. And the estimations can be further refined with few steps of curve fitting. Fig.1 outlines the overall pipeline of our method.
We tested our method on our in-house clinical prostate DCE-MRI data of 164 cases with pathology-proven prostate cancer.
We calculated the $$$K^{trans}$$$ as well as the new $$$\beta$$$ on these cases and evaluate their values in tumors and healthy tissues. For each patient, we outlined the lesion region and corresponding healthy tissue regions on the $$$K^{trans}$$$ map with the annotations on histopathology and T2-weighted images as reference. Fig.2 illustrates how we annotated on the $$$K^{trans}$$$ maps.
We also tested our method on Digital Reference Objects (DRO) that is synthesized in a similar with the synthetic training data to assess the accuracy of our dispersion-applied AIF and fixed AIFs.
Results
The running time comparisons are summarized in Fig.3. On the same device of a GPU, our method significantly reduced the per-patient processing time from more than half an hour to less than a minute.Some of the $$$K^{trans}$$$ maps and corresponding T2w and histopathology maps are shown in Fig.4. Our "beta $$$K^{trans}$$$" is more clear and has better distinction between csPCa and healthy tissue.
We also quantitatively evaluate the contrast of each annotated lesion and healthy tissue regions. We summarized the statistics of the average $$$K^{trans}$$$ values in each region in Fig.5. In general, the $$$K^{trans}$$$ values are higher in tumor than in healthy tissue, and our new "beta $$$K^{trans}$$$" is able to improve the contrast between tumor and healthy tissue.
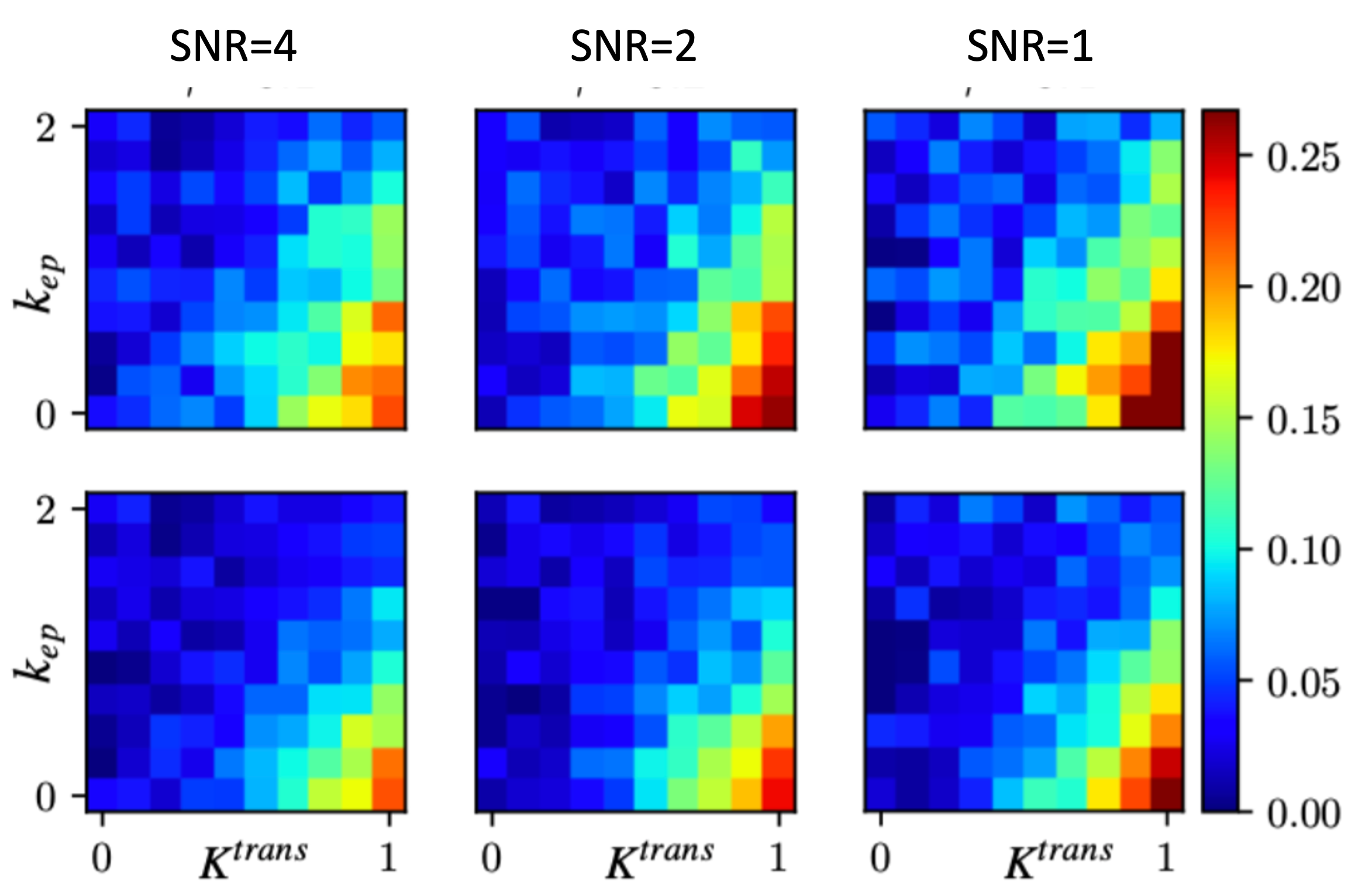
Fig.6 shows the estimation errors with DROs of different $K^{trans}$ and $k_{ep}$ values under different SNRs. Our method reduces the error of estimation at under all SNRs, revealing more accurate PK parameter estimation.
Conclusion
We proposed a deep learning based method for fast PK parameter estimation for DCE-MRI. An efficient dispersion-applied AIF was also proposed for flexible AIF in PK modeling. Experimental results on in-house prostate DCE-MRI of 164 cases demonstrate that the proposed method is sifnificantly faster then conventonal curve fitting methods, and achieves more accurate parameter estimations.Acknowledgements
This work was supported by the National Institutes of Health (NIH) R01-CA248506 and R01-CA272702, and funds from the Integrated Diagnostics Program, Departments of Radiological Sciences & Pathology, David Geffen School of Medicine at UCLA.References
[1] Weinmann, Hanns-Joachim, M. Laniado, and W. Mützel. "Pharmacokinetics of GdDTPA/dimeglumine after intravenous injection into healthy volunteers." Physiological chemistry and physics and medical NMR 16.2 (1984): 167-172.
[2] Parker, Geoff JM, et al. "Experimentally‐derived functional form for a population‐averaged high‐temporal‐resolution arterial input function for dynamic contrast‐enhanced MRI." Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine 56.5 (2006): 993-1000.
[3] Sung, Kyunghyun. "Modified MR dispersion imaging in prostate dynamic contrast‐enhanced MRI." Journal of Magnetic Resonance Imaging 50.4 (2019): 1307-1317.
[4] Tofts, Paul S., et al. "Estimating kinetic parameters from dynamic contrast‐enhanced T1‐weighted MRI of a diffusable tracer: standardized quantities and symbols." Journal of Magnetic Resonance Imaging: An Official Journal of the International Society for Magnetic Resonance in Medicine 10.3 (1999): 223-232.
Figures
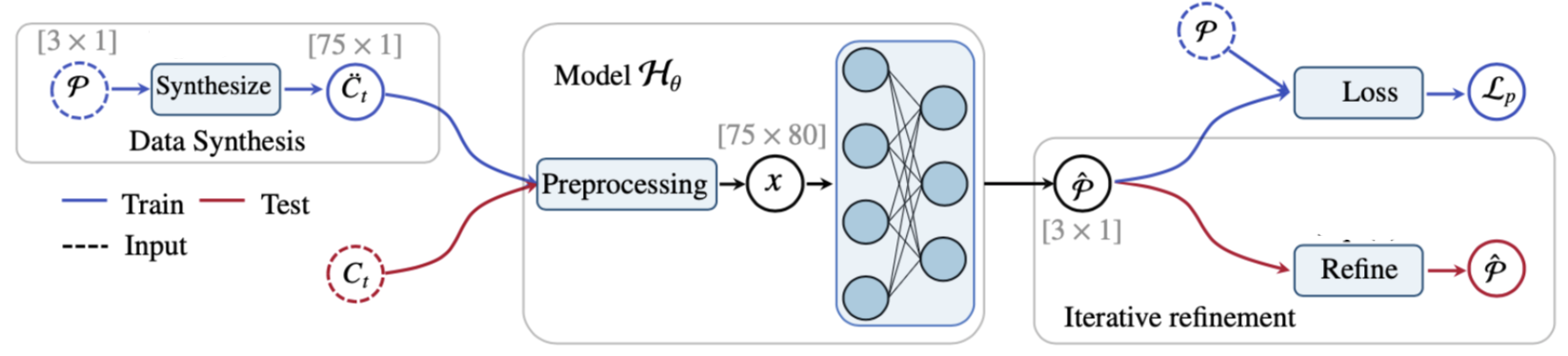
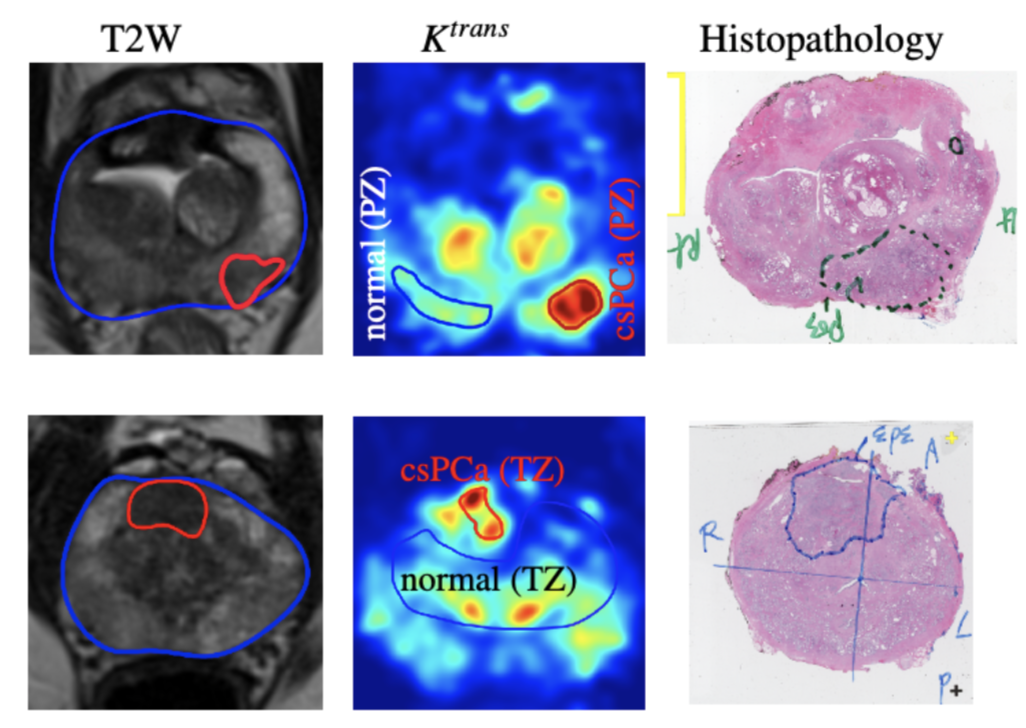
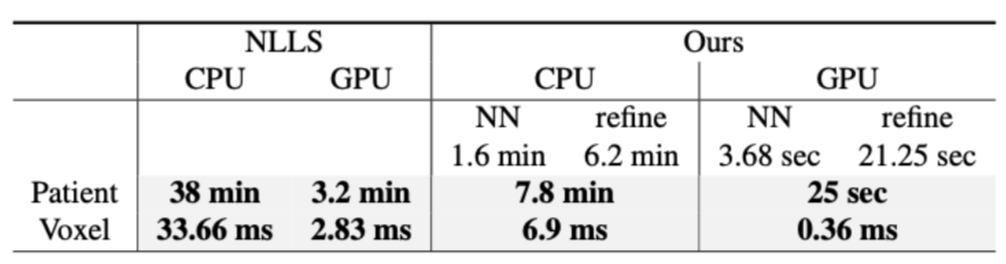
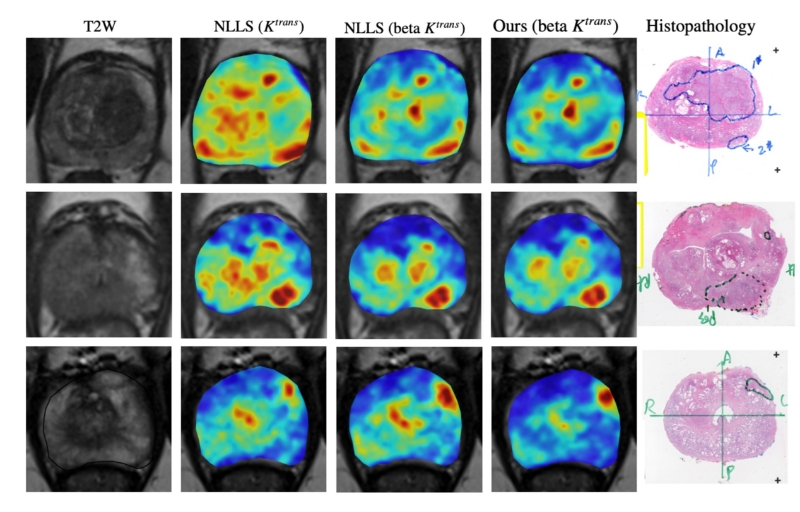
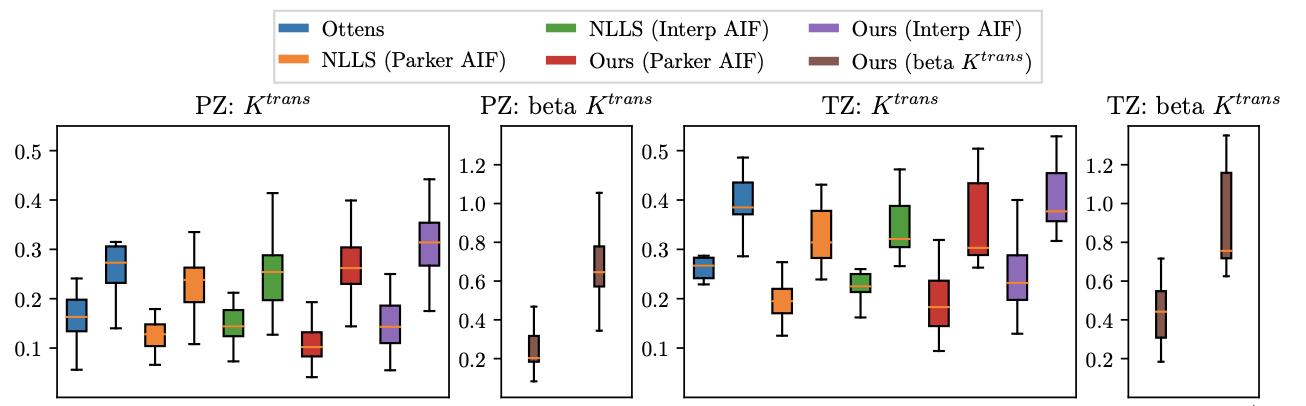
Figure5. Statistic results of $$$K^{trans}$$$ and "beta $$$K^{trans}$$$" of different methods including conventional NLLS and a recent deep learning based method (Ottens). Each pair of bars of the same color represents the lesion and background of the same method. Our "beta $$$K^{trans}$$$" has better distinction between lesions and healthy tissues.