3600
Using intra-and peri-tumoral radiomics features to identify LMN and LVSI in endometrial cancer from MRI images1Shanghai Key Laboratory of Magnetic Resonance, East China Normal University, Shanghai, China, 2Department of Radiology, Obstetrics and Gynecology Hospital, Fudan University, Shanghai, China, 3MR Scientific Marketing, Siemens Healthineers Ltd, Shanghai, China
Synopsis
Keywords: Diagnosis/Prediction, Cancer
Motivation: Preoperational identification of lymph node metastasis (LNM) and lymphatic vascular space invasion (LVSI) of endometrial cancer from MRI is important to treatment planning.
Goal(s): To explore power of intra/peri-tumor radiomic features from DWI, T1CE and T2W images to identify LVSI and LNM.
Approach: We developed radiomics models with intra/peri-tumor features from different MRI images and compared their performance.We developed radiomics models for intra- and peri-tumoral features and compare performance.
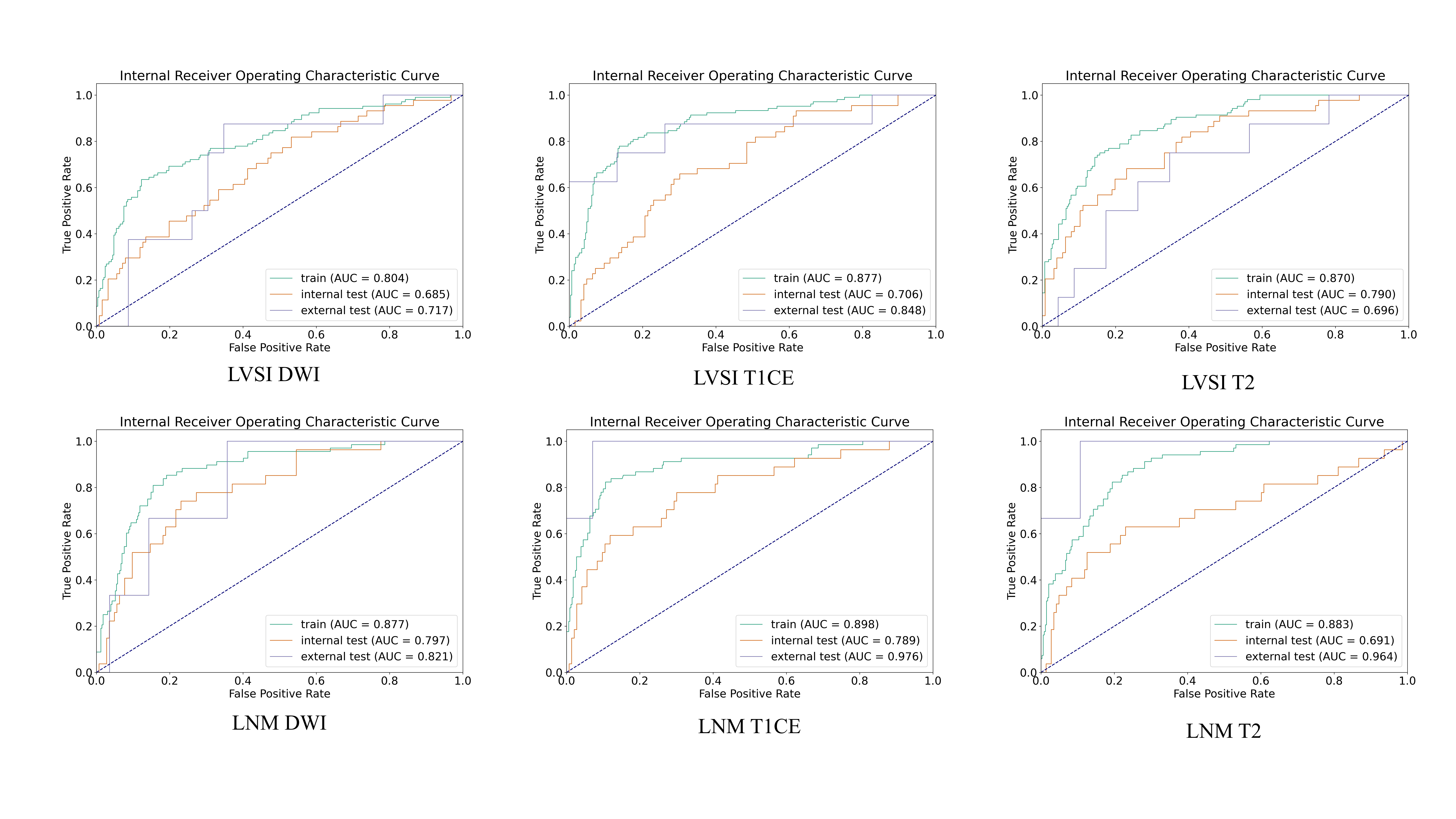
Results: For LVSI, T2W model using both intra- and peri-tumoral features achieved AUC values of 0.790/0.696 in internal/external test cohorts. For LNM, the combined model achieved AUC values of 0.801/0.976 in internal/external test cohorts.
Impact: The radiomics signatures built with intra- and peri-tumoral features extracted from DWI, T1CE, T2W sequences can yield satisfactory predictions for both LVSI and LNM status in endometrial cancer.
INTRODUCTION
Endometrial cancer (EC) is the most common gynecological cancer worldwide [1]. Lymph node metastasis (LNM) and lymphatic vascular space invasion (LVSI) status are crucial factors influencing the treatment plan and prognosis of EC[2, 3]. Therefore, the preoperational detection of both is very important.Magnetic resonance imaging (MRI) is the modality of choice for EC diagnosis, staging, and posttreatment evaluation. While LNM is associated with suspected pelvic metastatic node with a short diameter larger than 10mm, LVSI cannot be identified by naked eye. Radiomics has been used to predict LNM and LVSI positive status. However, these studies only extracted features from the whole tumor. We extracted radiomics features from both intra- and peri-tumor regions to assess their values in both LVM and LVSI status identification.
METHODS
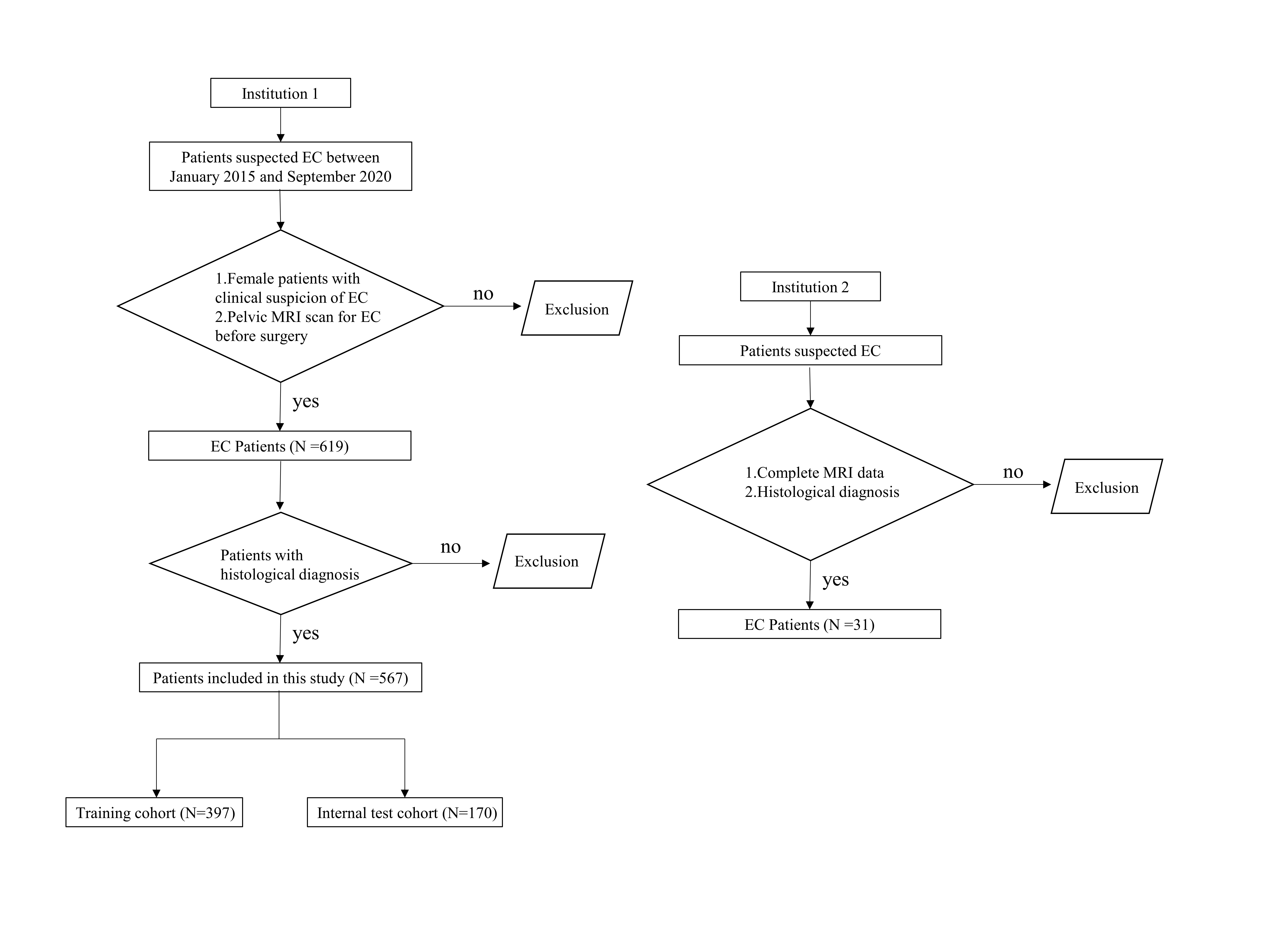
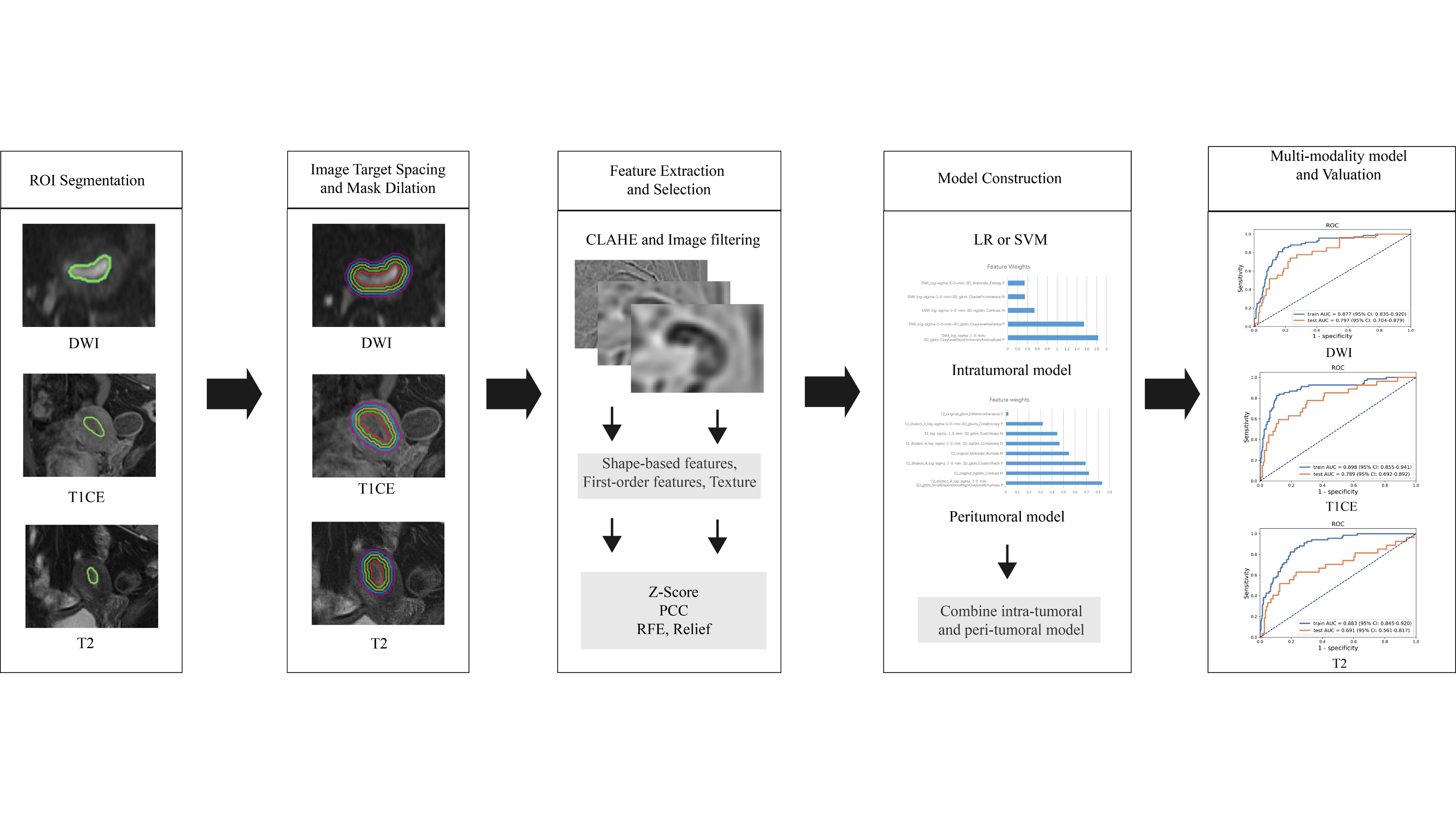
We retrospectively recruited (Fig. 1) 567 EC patients who underwent 1.5 T preoperative MRI scanning and split all patients randomly into training (N = 398) and test cohorts (N = 169). External test cohort contained 31 patients who underwent 1.5T scans in another institution. Scanning protocol includes DWI, T1CE, and T2W sequences.The workflow was presented in Fig. 2. Firstly, two experienced radiologists outlined the whole lesion ROI, which were dilated to get the peri-tumor region. Features were extracted from both intra- and peri-tumor regions using an open-source software FeatureExplorer (version 0.5.2)[4] and normalized with z-score. Pearson correlation coefficient (PCC) was used to remove redundancy among features. We adopted a heuristic hierarchical approach for feature selection, where features were grouped to small subgroups and a scout model was built for each subgroup. Features retained in the scout model with a validation AUC≥0.6 were used in further model construction. Combination of two feature selectors (RFE and Relief) and two classifiers (logistic regression and SVM) were tried out. Five-fold cross validation over the training cohort was used for model selection and hyperparameter tuning. Features retained in the scout models were combined to build intra- and peri-tumor models, and features kept in these two models were combined to build intra-/peri-tumor model. The same process was used to build models for both LVSI and LNM prediction.
To find the optimal thickness used for peri-tumor features extraction for different sequences, different thickness was used to build single sequence peri-tumor models, and cross-validation was used on the training set to select the thickness yielding the highest average cross-validation AUC.
RESULTS
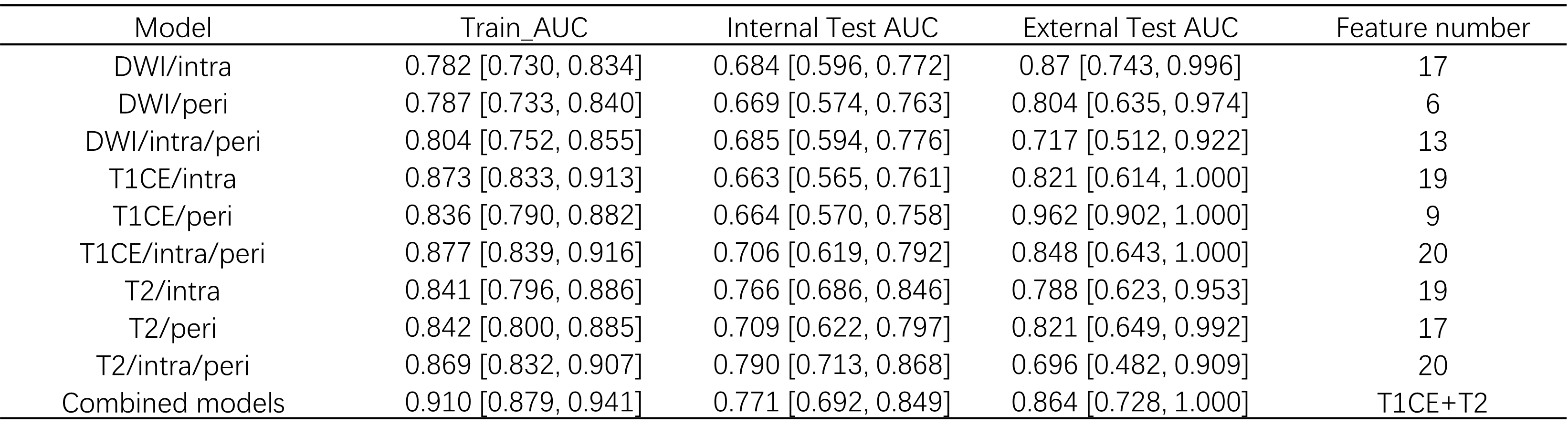
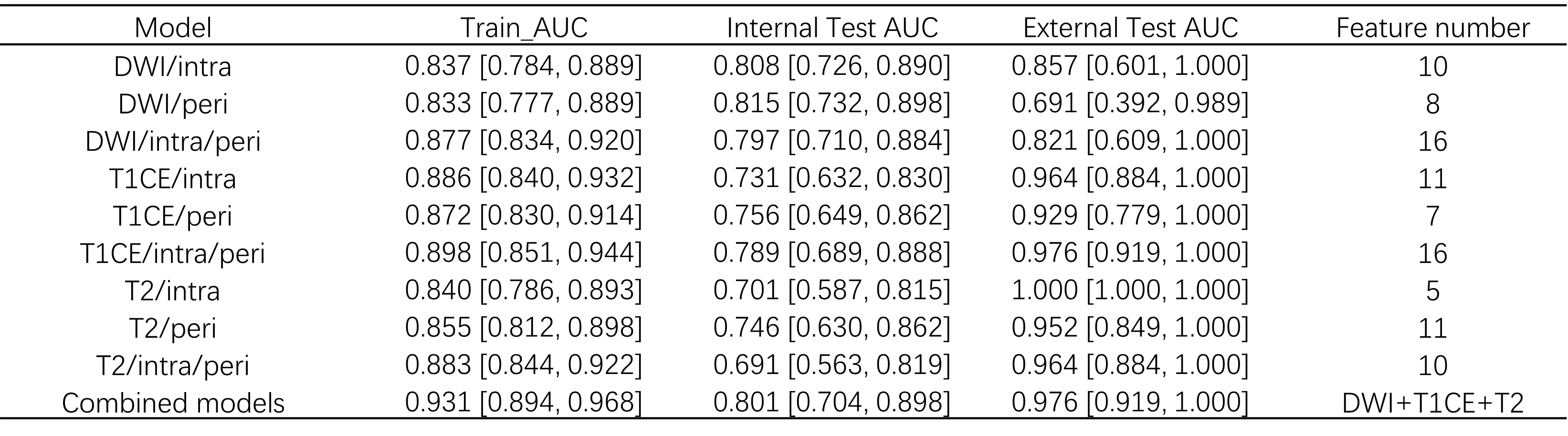
The performance metrics of different models are summarized in Table 1 and Table 2. For LVSI status identification, intra-tumor features showed better performance. Radiomic features extracted from the T2W images achieved the best performance with an internal test AUC of 0.766 (95%CI: [0.686-0.846]) and external test AUC 0.788 (95%CI: [0.623-0.954]). For LNM, peritumoral features showed better performance. Radiomic features extracted from the DWI achieved the highest performance with AUC values of 0.815 (95%CI: [0.732, 0.898]) and 0.691 (95%CI: [0.392-0.989]) in internal and external cohorts, respectively.For models using both intra- and peri-tumoral features, T2W model achieved the highest AUC of 0.790 (95%CI:0.713-0.867) for LVSI and DWI model achieved the highest AUC of 0.797 (95%CI: 0.710-0.884), which were not significantly different from models built with only intra- or peri-tumoral features. A combined LR model using output from three intra-/peri-tumor models was also built, however, the performance of model was not significantly different from models built with single sequences.
DISCUSSION and CONCLUSION
The results demonstrated that both intra- and peri-tumor features contributed to the identification of LNM and LVSI status, suggesting peritumor morphology is also related to the pathological type. Interestingly, different thickness was found for different sequences, with the best thickness for DWI, T1CE and T2W was 10, 6, and 5 mm, respectively. This also demonstrated the differences in manifestations of peri-tumor morphology on different sequences.Each sequence exhibits varying discriminative power for different tasks. T2W model and T1CE models exhibited the best performance for LVSI and LNM identification, respectively. It is worth noting that combining features from different sequences did not lead to a significant performance improvement, same as combining both intra- and peri-tumor features. This may be due to the redundancy in the information provided by different regions and sequences, or due to the overfitting caused by high dimension data from multiple regions on multiple sequence images, which should be studied with larger dataset in the future.
In intra-tumor models, SurfaceVolumeRatio was frequently used with a significant negative weight, implying that tumors with a spheric shape tend to be diagnosed as LVSI or LNM positive. This may provide some new insights for doctors diagnosing endometrial cancer.
Acknowledgements
No acknowledgement found.References
1. Crosbie EJ, Kitson SJ, McAlpine JN, Mukhopadhyay A, Powell ME, Singh N (2022) Endometrial cancer. Lancet 399:1412-1428
2. Bodurtha Smith AJ, Fader AN, Tanner EJ (2017) Sentinel lymph node assessment in endometrial cancer: a systematic review and meta-analysis. Am J Obstet Gynecol 216:459-476 e410
3.
Kitchener H, Swart AM, Qian Q, Amos
C, Parmar MK (2009) Efficacy of systematic pelvic lymphadenectomy in
endometrial cancer (MRC ASTEC trial): a randomised study. Lancet 373:125-136
Figures