3598
Preoperative prediction of lymph node metastasis in endometrial cancer based on an intra- and peritumoral multiparameter MRI radiomics nomogram1Department of Radiology, Shaanxi Provincial Tumor Hospital, Xi'an Jiaotong University, Xi'an, China
Synopsis
Keywords: Diagnosis/Prediction, Tumor, Endometrial cancer; Lymphatic metastasis; Lymph node; Magnetic resonance imaging; Radiomics
Motivation: Whether lymph node metastasis (LNM) affects surgical management in endometrial cancer (EC) patients.
Goal(s): To develop and validate a nomogram based on intra- and peritumoral radiomics features and multiparameter MRI imaging features to preoperatively predict LNM in EC.
Approach: Three hundred and seventy-four women with histologically confirmed EC were divided into training (n = 220), test (n = 94), and external-validation cohorts (n = 60). Radiomics features were extracted from intra- and peritumoral regions based on axial T2WI and ADC mapping.
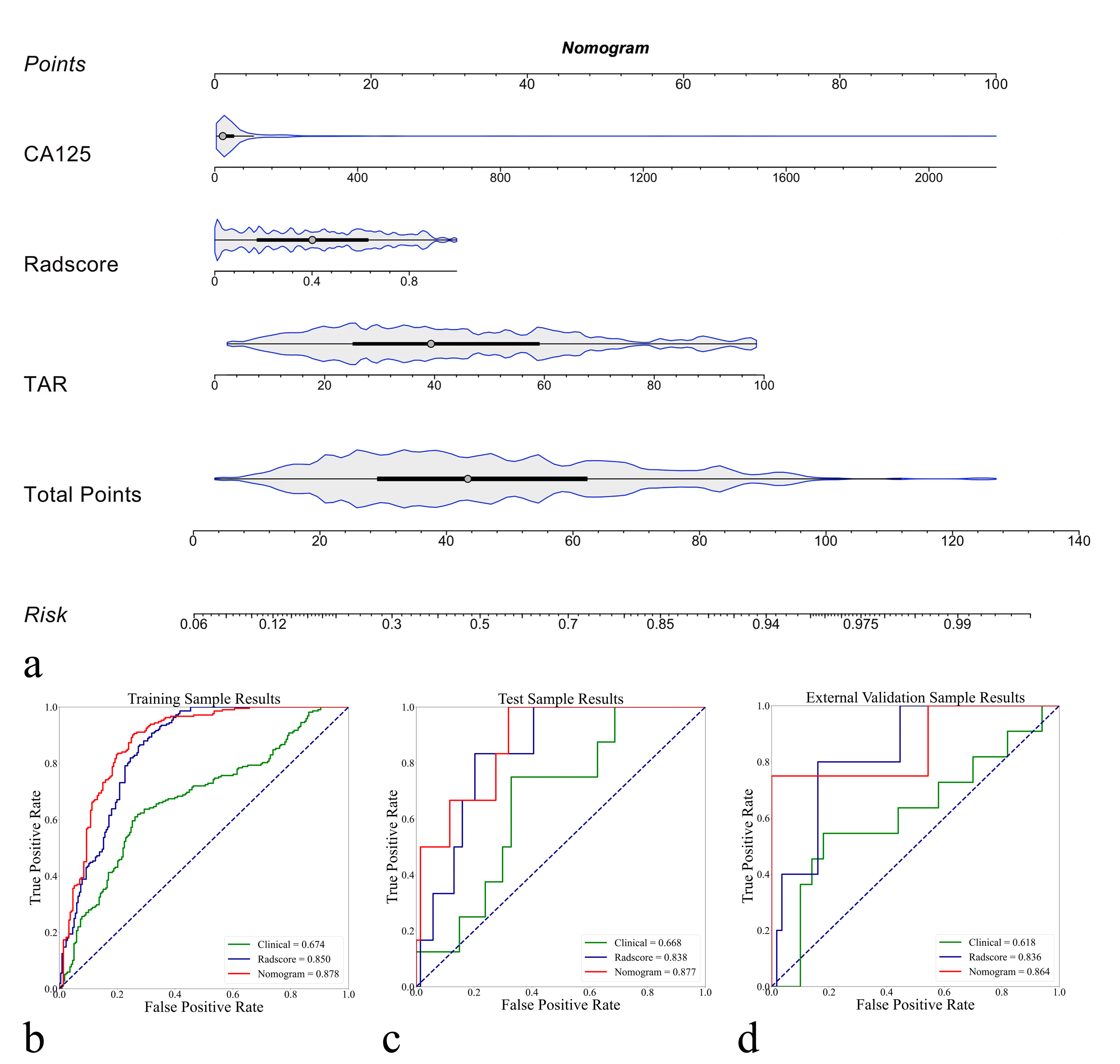
Results: The nomogram combining the Radscore, CA125, and TAR showed good diagnostic performance (AUCtraining = 0.878, AUCtest = 0.877, AUCexternal-validation = 0.864).
Impact: The combined intra- and peritumoral region multiparameter MRI radiomics nomogram could be used to preoperatively predict LNM in EC. Moreover, different field strength data were proportionally mixed for modeling and external validation, expanding the real-world application scenarios of prediction models.
Introduction
Whether lymph node metastasis (LNM) affects surgical management in endometrial cancer (EC) patients. MRI remained the cornerstone for evaluating LNM in EC, showing satisfactory specificity but relatively low sensitivity with 36%–89.5% [1]. Recently, radiomics research (based on intratumoral features) on the preoperative prediction of LNM has shown encouraging achievements [2-5]. However, research on improving the diagnostic performance of the preoperative prediction of LNM in EC by combining different tumor regions is lacking.In this study, we aimed to develop and validate an MR-based radiomics nomogram combining different imaging sequences (i.e., apparent diffusion coefficient (ADC) mapping and T2-weighted imaging (T2WI)), different tumor regions (combined intra- and peritumoral regions), and different parameters (CA125, tumor morphological features, and radiomics features) for predicting LNM in EC.
Methods
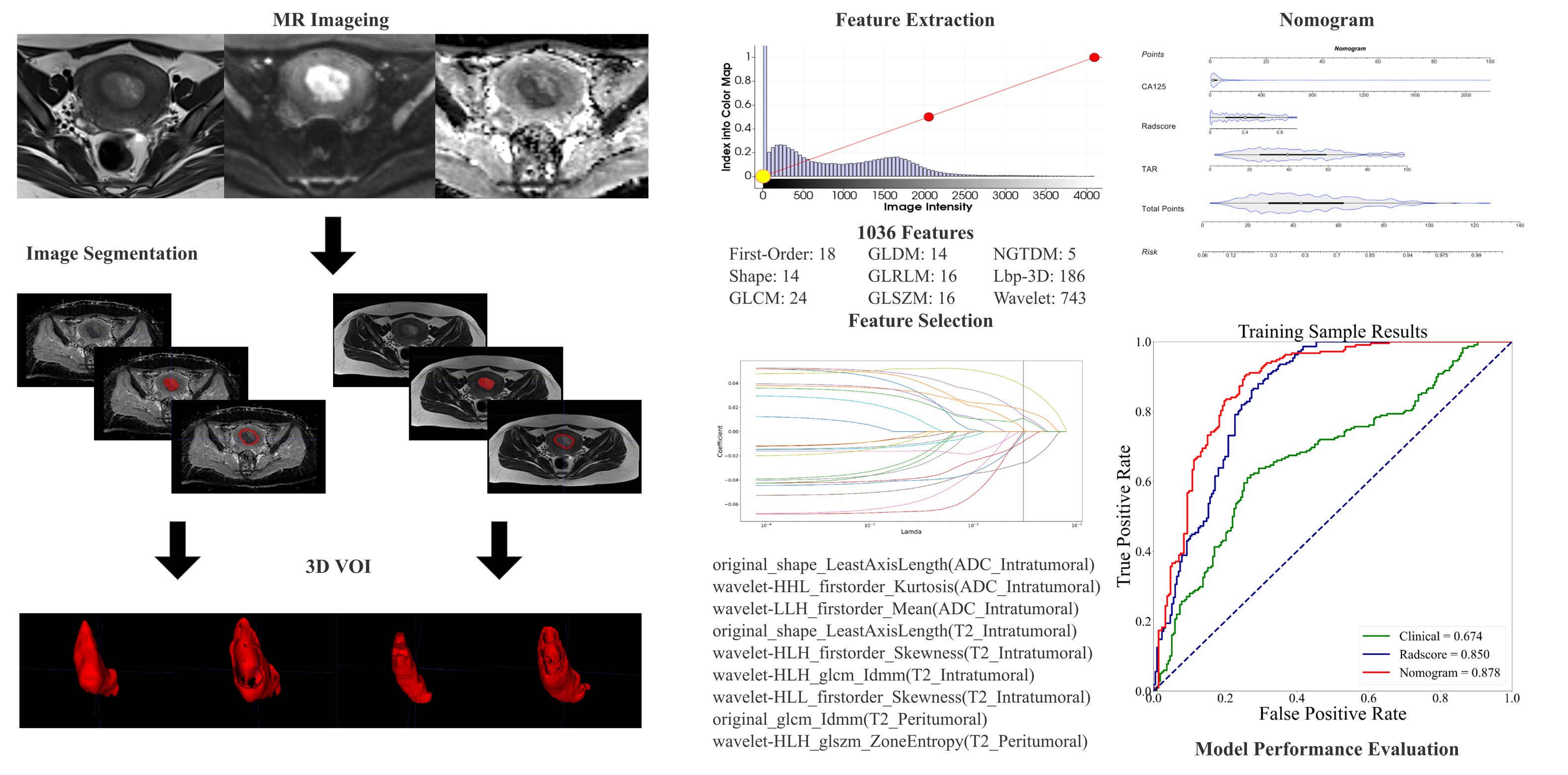
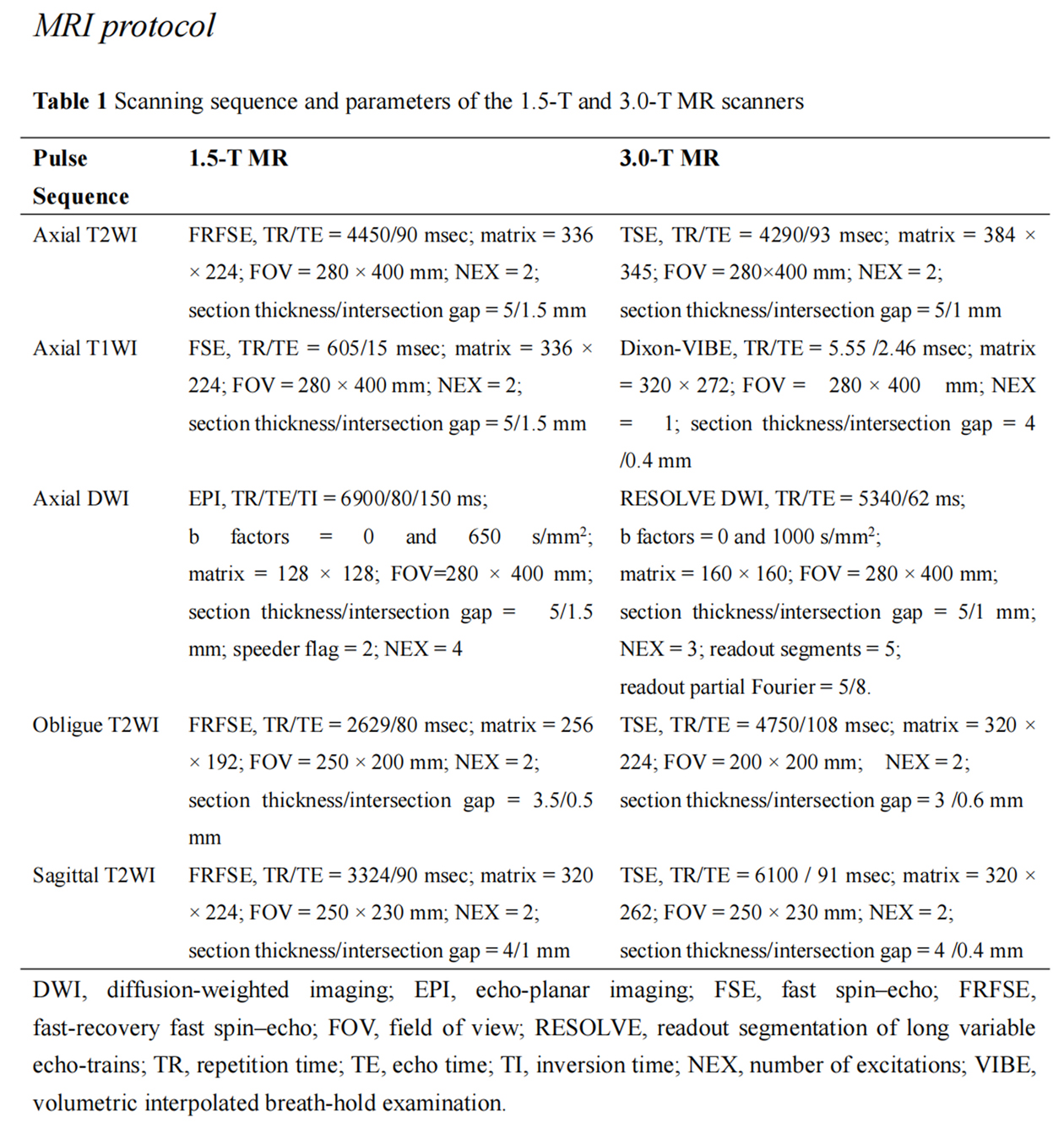
A total of 374 patients with EC confirmed by postoperative histology were enrolled from June 2015 to July 2022. MRI was performed using a 1.5-T (EXCELART VantageTM powered by Atlas, Canon Medical Systems Corp., Tochigi, Japan) or 3.0-T (Siemens Magnetom Skyra, Erlangen, Germany) scanner with an 8-channel phased-array abdominal coil. All MRI sequences were acquired using a standard protocol in Table 1.The software 3D Slicer (version 4.10.2) was used for whole-tumor manual segmentation. Three volumes of interest (VOIs) were chosen: (1) Intratumoral region: ROIs included areas of hemorrhage and necrosis. (2) Peritumoral margin: The tumor contour was automatically dilated by 3 mm to generate dilated VOIs. Peritumoral region = dilated VOI - tumor VOI. (3) Combined intra- and peritumoral regions. Feature extraction was performed with Artificial Intelligence Kit (AK, Version 3.3.0, GE Healthcare) software. The extraction process for the radiomics parameters is shown in Fig. 1. The morphological parameter were included: tumor size, maximum anteroposterior tumor diameter (APsag), tumor volume, and tumor area ratio (TAR).
The training cohort was used for feature selection and model construction, and the external validation cohort was used only to evaluate model performance. A binary logistic regression (LR) classifier was constructed to predict the LNM status: "LNM-positive" and "LNM-negative".
R software (Version 4.2.0) was used to evaluate clinical and radiomics data. Clinical data were selected using LR. Radiomics data were filtered using the t, Fisher’s exact, and chi-square tests and, when applicable, the Mann‒Whitney U test, after then LASSO identified key features. LR trained prediction models, leading to a nomogram integrating clinical parameters and Radscore. The radiomics nomogram's clinical benefit was assessed using Hosmer-Lemeshow (HL) test, and decision curve analysis (DCA).
Results
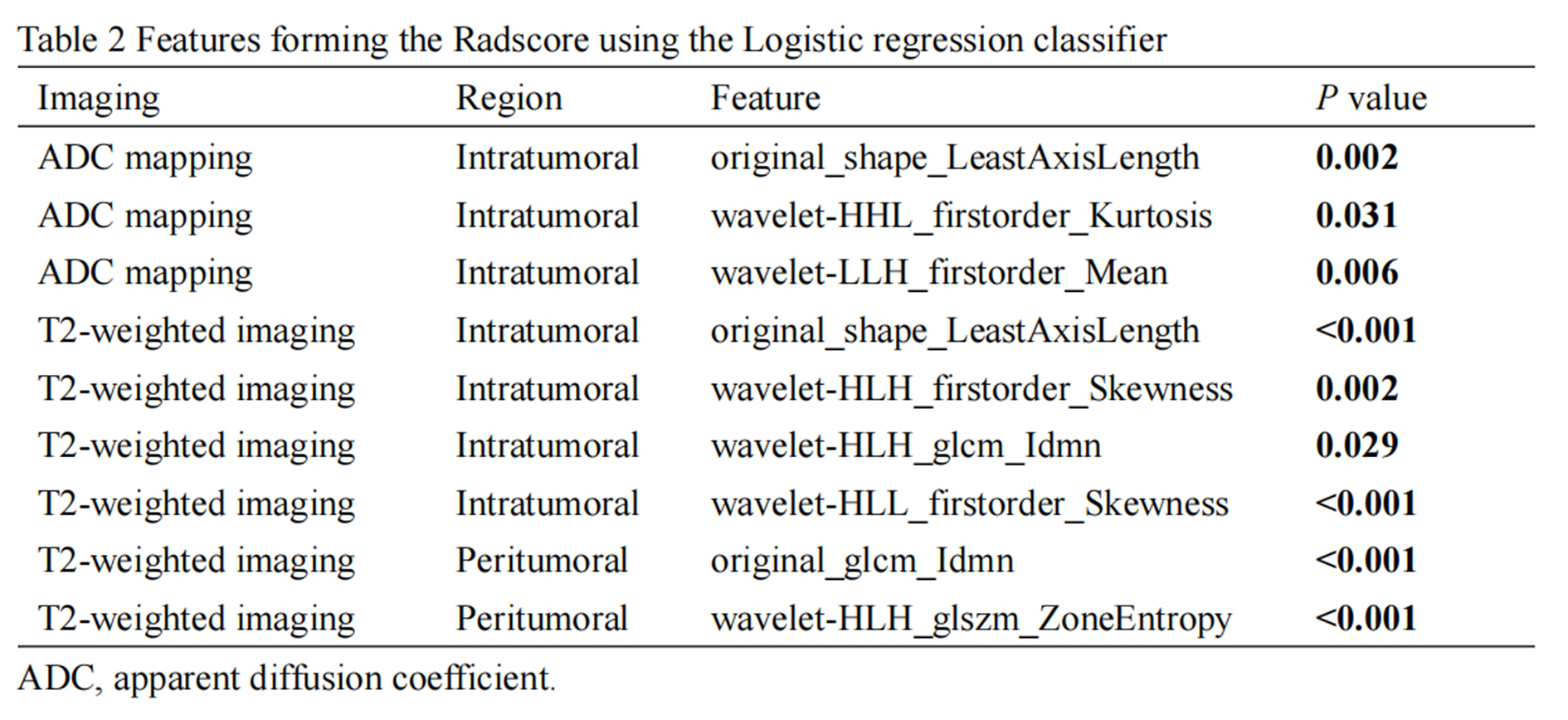
The 374 EC (1.5-T, n = 233; 3.0-T, n = 141) included 40 LNM-positive and 334 LNM-negative patients. First, 60 patients were randomly selected as the external validation group. Then, the remaining 314 patients were randomly divided into a training (n = 220) and a test cohort (n = 94) at a ratio of 7:3. All patients were recruited from a single center.One thousand thirty-six features were extracted from each VOI (i.e., ADCIntratumoral, ADCPeritumoral, T2WIIntratumoral, and T2WIPeritumoral). After feature selection, 9 features remained and were selected for evaluating LNM status in EC (forming the Radscore, Table 2). The Radscore combined the features of ADC mapping (intratumoral region) and T2WI (intra- and peritumoral regions) to build the best prediction model, which showed the best classification performance (AUCtraining = 0.850, AUCtest = 0.838, AUCexternal-validation = 0.836). Combining clinical model (predictors including TAR and CA125) and Radscore, a nomogram was developed (Fig. 2) with AUCs of 0.878, 0.877, and 0.864. The formula was as follows:Risk = -1.68215933-0.025*TAR+0.001*CA125+4.96239835*Radscore
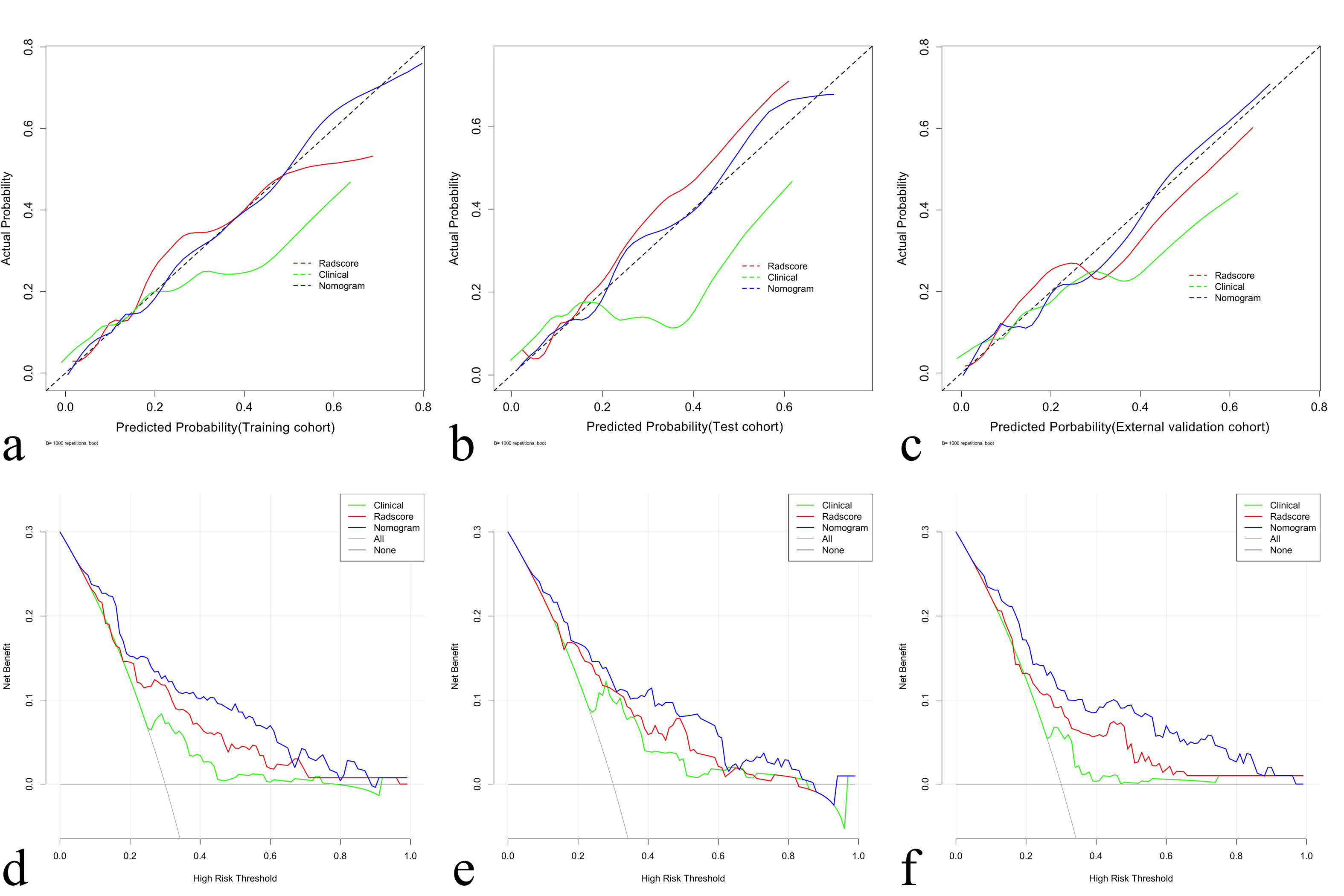
The calibration curves, with HL scores of 0.481, 0.346 and 0.226 for the training, test, and external validation cohorts (Fig. 3a-c), respectively. DCA indicated that the radiomics nomogram produced more net benefit than the clinical model for predicting LNM in EC patients in all of the cohorts (Fig. 3d-f).
Discussion
In the current study, we developed and validated a brief radiomics nomogram for predicting LNM in patients with EC based on clinical and morphological parameters and the Radscore, and this model showed good diagnostic performance. Second, the features from different imaging sequences and different VOIs provided complementary information. Compared with previous radiomics model (such as Xu et al [6] and Liu et al [5], in which the training and test cohorts were designed), we set up an external validation cohort, and our nomogram achieved good predictive performance (AUC = 0.864), proving that our model has good robustness.Conclusion
In conclusion, the multiparameter MRI radiomics nomogram was used to predict LNM presence in EC. The nomogram has generalization ability for predicting LNM, and has potential clinical usefulness in the surgical management of patients with EC.Acknowledgements
I would like to express my deepest gratitude to Zhihao Li (GE Healthcare, PDx, Xi'an), for his continuous guidance, feedback, and unwavering support throughout this research.References
[1] Nougaret S, Lakhman Y, Vargas HA, et al. From staging to prognostication: achievements and challenges of MR imaging in the assessment of endometrial cancer. Magn Reson Imaging Clin N Am. 2017;25(3):611-633.
[2] Lu W, Zhong L, Dong D, et al. Radiomic analysis for preoperative prediction of cervical lymph node metastasis in patients with papillary thyroid carcinoma. Eur J Radiol. 2019;118:231-238.
[3] Dong Y, Feng Q, Yang W, et al. Preoperative prediction of sentinel lymph node metastasis in breast cancer based on radiomics of T2-weighted fat-suppression and diffusion-weighted MRI, Eur Radiol. 2018;28(2):582-591.
[4] Shen C, Liu Z, Wang Z, et al. Building CT radiomics based nomogram for preoperative esophageal cancer patients lymph node metastasis prediction. Transl Oncol. 2018;11(3):815-824.
[5] Liu XF, Yan BC, Li Y, et al. Radiomics nomogram in assisting lymphadenectomy decisions by predicting lymph node metastasis in early-stage endometrial cancer. Front Oncol. 2022;12:894918.
[6] Xu X, Li H, Wang S, et al. Multiplanar MRI-based predictive model for preoperative assessment of lymph node metastasis in endometrial cancer. Front Oncol. 2019;9:1007.
Figures