3593
Low-dose Dynamic Imaging for Cerebrovascular Evaluation (LD-DICE)1Department of Biomedical Engineering, University of Southern California, Los Angeles, CA, United States, 2Department of Radiology, Keck School of Medicine, University of Southern California, Los Angeles, CA, United States, 3Department of Radiological Sciences, University of California, Los Angeles, Los Angeles, CA, United States, 4Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 5Department of Neuro-oncology, Keck School of Medicine, University of Southern California, Los Angeles, CA, United States, 6Department of Neurosurgery, Keck School of Medicine, University of Southern California, Los Angeles, CA, United States, 7Department of Radiation Oncology, Keck School of Medicine, University of Southern California, Los Angeles, CA, United States
Synopsis
Keywords: Tumors (Post-Treatment), DSC & DCE Perfusion, Low dose
Motivation: Gadolinium retention in the human body following dynamic contrast-enhanced (DCE) and dynamic susceptibility contrast (DSC) MRI remains a health concern to many patients, especially those who need long-term imaging follow-up.
Goal(s): This work aims to investigate the feasibility of using a recently developed technique, MR multitasking-based dynamic imaging for cerebrovascular evaluation (DICE), to quantify permeability and perfusion with a 0.03 mmol/kg dose.
Approach: Numerical simulations were conducted to determine the optimal dose level. Assessments for the agreement of low-dose DICE (LD-DICE) with full-dose DICE (FD-DICE) were performed.
Results: Good correlation was achieved. Brain tissue perfusion and permeability can be quantified simultaneously with LD-DICE.
Impact: Low-dose DICE will allow for comprehensive tumor vascularity evaluation with considerably less contrast agent than clinical standard protocols, which will benefit brain tumor patients who need frequent imaging follow-ups.
Introduction
Dynamic contrast-enhanced (DCE) MRI for microvascular permeability assessment and dynamic susceptibility contrast (DSC) MRI for brain perfusion can both offer important biomarkers during the management of brain tumors. However, conventional DCE and DSC are acquired with separate scans, often resulting in the need for double-dose gadolinium (Gd) contrast. This may cause remarkable Gd retention in many patients who need frequent imaging follow-ups. We recently developed a novel hybrid permeability-perfusion quantification technique, MR multitasking-based dynamic imaging for cerebrovascular evaluation (DICE)1, that had theoretically higher sensitivity to the brief Gd contrast bolus than conventional signal intensity-based methods because of mapping-based dynamic quantification of contrast concentration. In this work, we hypothesize that DICE imaging with a lower contrast dose is feasible for brain tumor assessment.Methods
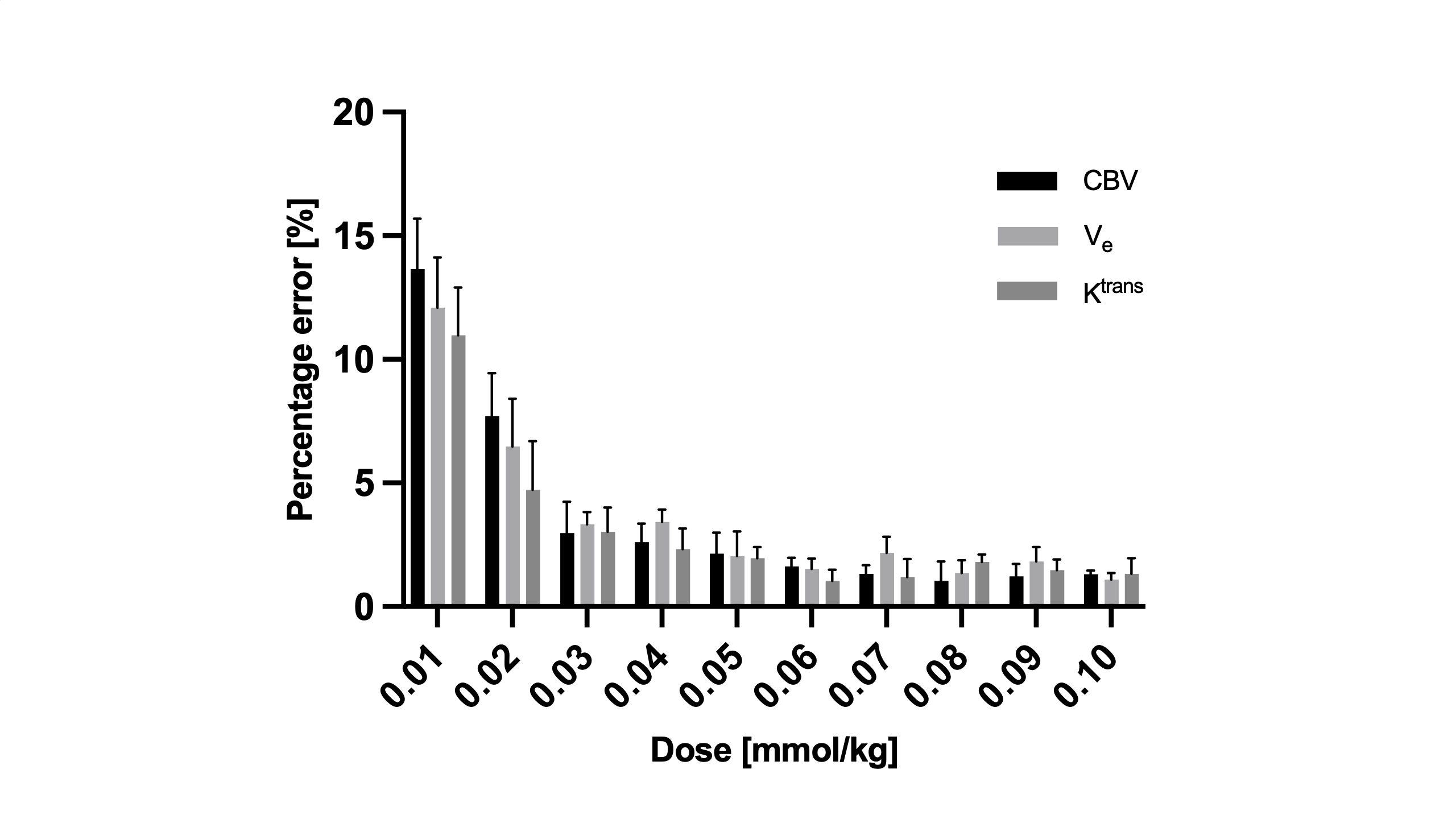
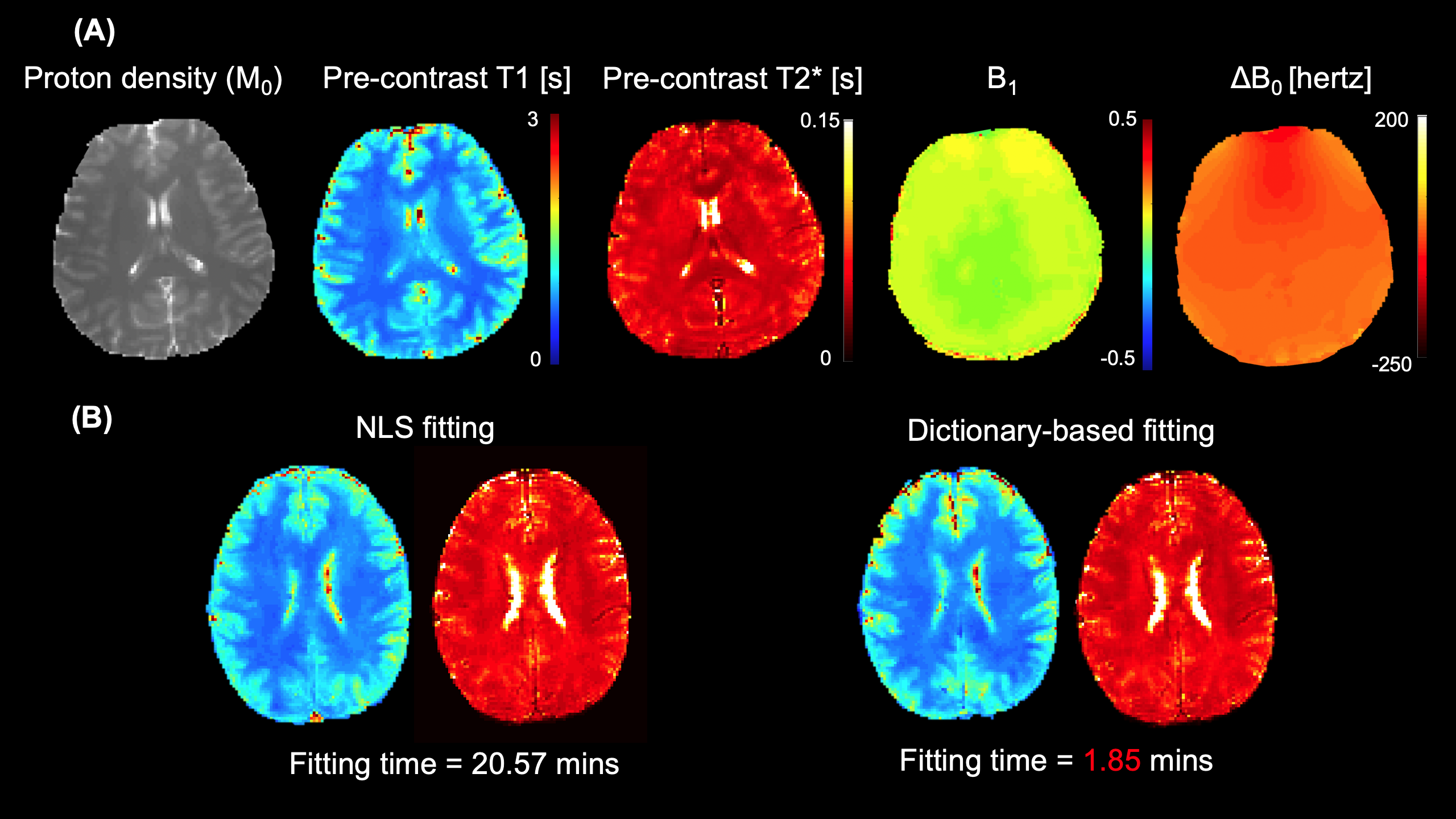
Numerical simulations: Numerical simulations were performed to determine the optimal contrast dosage with a 3D anthropomorphic digital brain phantom2 incorporating a heterogeneous tumor model. The T1-/T2*-based arterial input functions (AIFs) were generated with contrast dosage from 0.01 to 0.1 mmol/kg at a 0.01 mmol/kg increment. Dynamic images were created based on our DICE sequence design with white Gaussian noise added. To simulate the real situation, the k-space data were obtained from simulated dynamic images with the undersampling pattern and coil sensitivity maps from real in-vivo studys. After reconstruction with DICE framework, dynamic T1/T2* mapping and DCE/DSC metric estimation were conducted. Each simulation was repeated 10 times to analyze the quantification accuracy with each contrast dosage level. In-vivo experiment: Five healthy subjects were recruited to assess the correlation between low-dose DICE (LD-DICE) and full-dose DICE (FD-DICE). Both LD-DICE and FD-DICE were performed within the same imaging session with a 30-minute interval between them. One GBM patient was also recruited. All LD-DICE data were collected on a Siemens Vida 3T scanner (Siemens Healthineers, Germany) with the following imaging parameters: FOV=220×220×120 mm3, spatial resolution=1.7×1.7×3.5 mm3, TR=24.3 ms, TE=2.46//7.38/12.30/22.14 ms, temporal resolution (i.e., saturation recovery period) =1.1s, FA=10°, total time=8 min. MultiHance of 0.03 mmol/kg (determined with the numerical simulations) was administered 1.5 min into the scan at the rate of 3.0 mL/s. FD-DICE data were collected using the same sequence parameters with a single-dose contrast injection (0.1 mmol/kg). Image and statistical analysis: A dictionary-based mapping method was used to rapidly derive dynamic T1/T2* values from reconstructed six-dimensional images. The off-resonance effect ($$$\Delta B_0$$$) and B1 inhomogeneity were also considered during mapping. The dictionary was generated with the following signal equation:$$\begin{aligned} & S\left(A, \alpha, B_1, n, T E, T 1(t), T 2^*(t), \Delta B_0\right) \\ & =A \frac{1-e^{-T R / T 1(t)}}{1-e^{-T R / T 1(t)} \cos \alpha}\left[1+\left(B_1-1\right)\left(e^{-T R / T 1(t)} \cos \alpha\right)^n\right] e^{-T E / T 2^*(t)} e^{\mathrm{j} 2 \pi \Delta \mathrm{B}_0 T E} \sin \alpha\end{aligned}$$
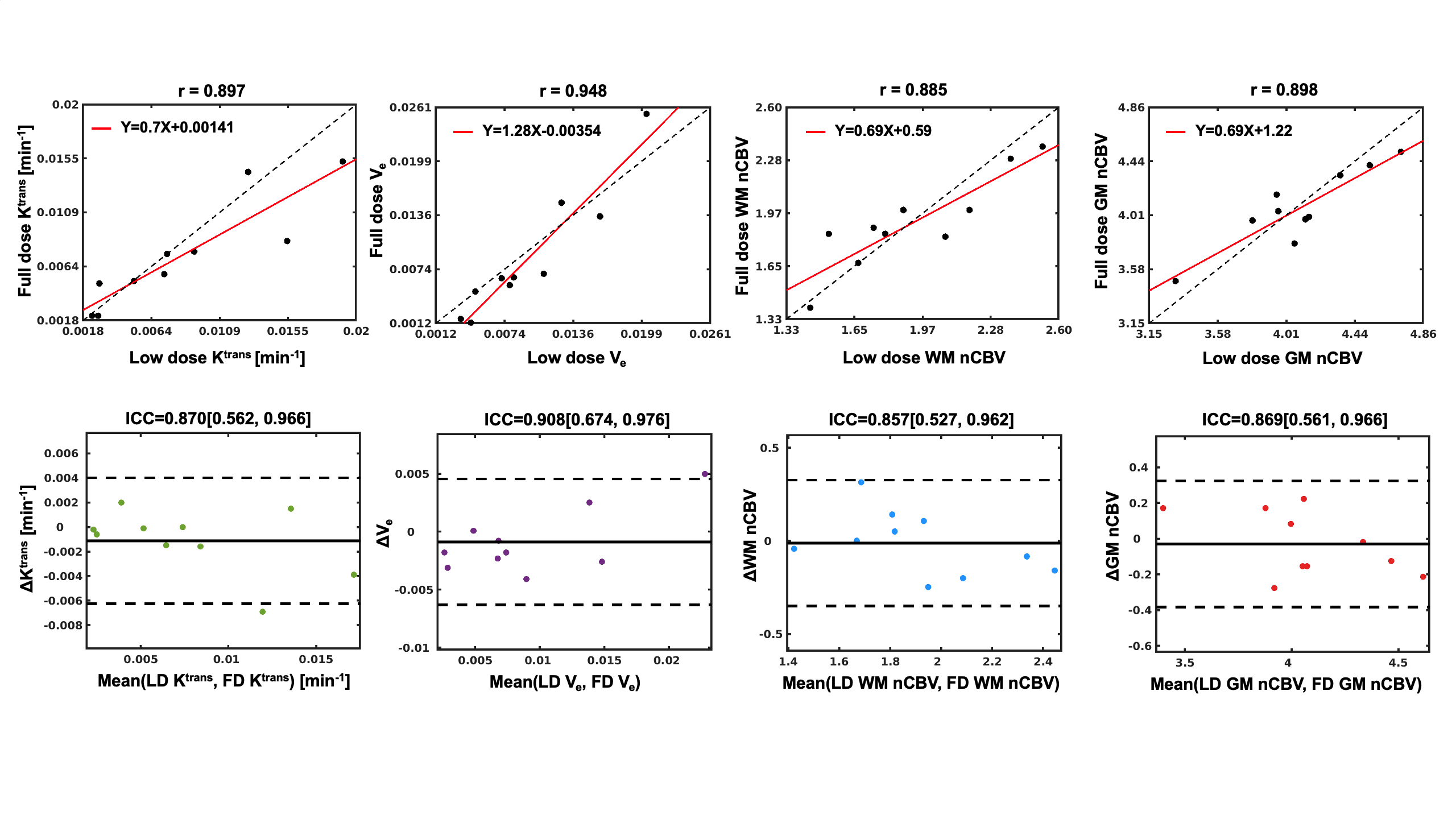
The ranges of T1, B1, T2* and were chosen according to typical values of tissues in the brain considering contrast agent influence. Dynamic T1/T2*/B1/$$$\Delta B_0$$$ maps can be obtained with pixel-wise template matching. Kinetic parameters Ktrans, Ve and leakage-insensitive CBV were estimated with the same post-processing pipeline demonstrated in our previous MT-DICE. Ten regions of interest (5 each from gray matter (GM) and white matter (WM)) were selected on 5 healthy subjects. Then, the linear regression and Bland-Altman analysis were used to assess correlation between LD-DICE and FD-DICE. Intraclass correlation coefficient (ICC) and Pearson correlation coefficient (r) were also calculated.
Results
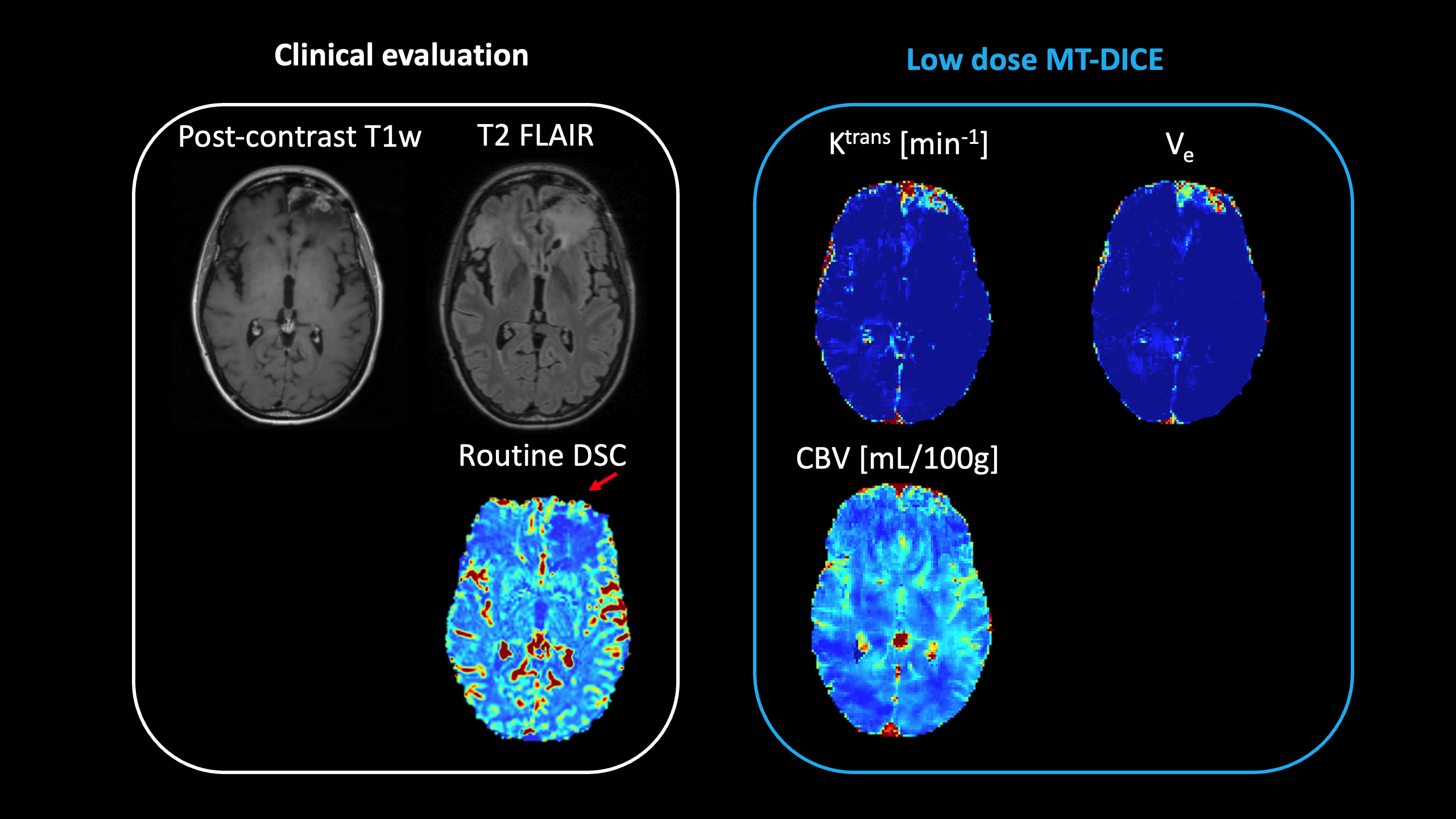
Fig.1 shows means and standard deviations (SD) of parameter estimation percentage errors for different dose levels in numerical simulations. The 0.03 mmol/kg was found to be the optimal dose level for our LD-DICE (the mean percentage error is 2.81%). Example pre-contrast maps generated with the dictionary-based mapping are shown in Fig. 2(A). Considerably shorter fitting time (1.85 vs 20.57 mins) with a similar map quality was achieved using the dictionary-based mapping (Fig. 2(B)). LD-DICE derived parameters Ktrans, Ve, and CBV are in good agreement with FD-DICE measurements (r=0.897, 0.948, 0.885, 0.898; ICC=0.870, 0.908, 0.857, 0.869, respectively; Fig. 3). Representative maps of low-dose DICE for a GBM patient are displayed in Fig. 4.Discussion and conclusion
With higher sensitivity to the brief MR contrast bolus, low-dose DICE is feasible to simultaneously provide high-quality DCE/DSC metric maps with a single 8-min scan. However, double (for both DCE and DSC) or single (for DSC) contrast dose injection is needed in standard clinical protocols. By substantially reducing Gd dose from 0.2 mmol/kg to 0.03 mmol/kg without losing quantification accuracy, low-dose DICE should become a useful tool for comprehensive tumor vascularity evaluation. Both the concern regarding the Gd deposition in body tissues and the distress endured by brain tumor patients will be alleviated.Acknowledgements
No acknowledgement found.References
1. Hu Z, Christodoulou AG, Wang N, et al. MR multitasking-based dynamic imaging for cerebrovascular evaluation (MT-DICE): Simultaneous quantification of permeability and leakage-insensitive perfusion by dynamic T1/T2* mapping. Magnet Reson Med. 2022. doi:10.1002/mrm.29431
2. C.A. Cocosco, V. Kollokian, R.K.-S. Kwan, A.C. Evans : "BrainWeb: Online Interface to a 3D MRI Simulated Brain Database"NeuroImage, vol.5, no.4, part 2/4, S425, 1997 -- Proceedings of 3-rd International Conference on Functional Mapping of the Human Brain, Copenhagen, May 1997.
Figures