3587
The importance of dynamic contrast-enhanced MRI in preoperative prediction of glioma genotype and prognosis1Sun Yat-sen University First Affiliated Hospital Department of Radiology, Guangzhou, China, 2Philips Healthcare, Guangzhou, China
Synopsis
Keywords: Tumors (Pre-Treatment), Brain, glioma
Motivation: Accurate preoperative noninvasive diagnosis and classification of diffuse gliomas have a significant impact on clinical management and are of significant prognostic importance.
Goal(s): To investigate the diagnostic efficacy and clinical value of preoperative DCE-MRI in predicting genotype and prognosis of glioma.
Approach: Adult diffuse gliomas were enrolled. Univariate and multivariate logistic or cox regression analysis are performed for diagnosing glioma gene and prognosis.
Results: Preoperative DCE-MRI exhibits favorable diagnostic capabilities in identification of IDH mutation status with AUC value of 0.77, 1p19q codeletion with AUC value of 0.71, and CDKN2A/B homozygous deletion with AUC value of 0.93, and assessment of glioma prognosis.
Impact: This study highlighted potential clinical application of DCE-MRI by demonstrating the robust diagnostic performance of DCE-derived parameters. These parameters exhibited not only excellent diagnostic accuracy in identifying functional biomarkers such as IDH, 1p19q and CDKN2A/B, but also in predicting prognosis.
Preoperative prediction of glioma genotype and prognosis is critical to know the natural course of glioma and stratify patients to optimize treatment strategy. Notely, the 2021 edition WHO classification of glioma underscored the importance of genotypes such as chomozygous losses of cyclin-dependent kinase inhibitor 2A/B (CDKN2A/B) in diagnosis and prognosis of adult-type diffuse gliomas [1, 2]. And as a noninvasive advanced MRI technique, dynamic contrast enhanced MR (DCE-MRI) looks particularly intriguing due to the superior ability of assessing intratumoral heterogeneity, tissue permeability and microcirculatio. So we explored to investigate efficacy of preoperative DCE-MRI examinations in gliomas genotype and their prognostic prediction, using the 2021 WHO classification.
Methods
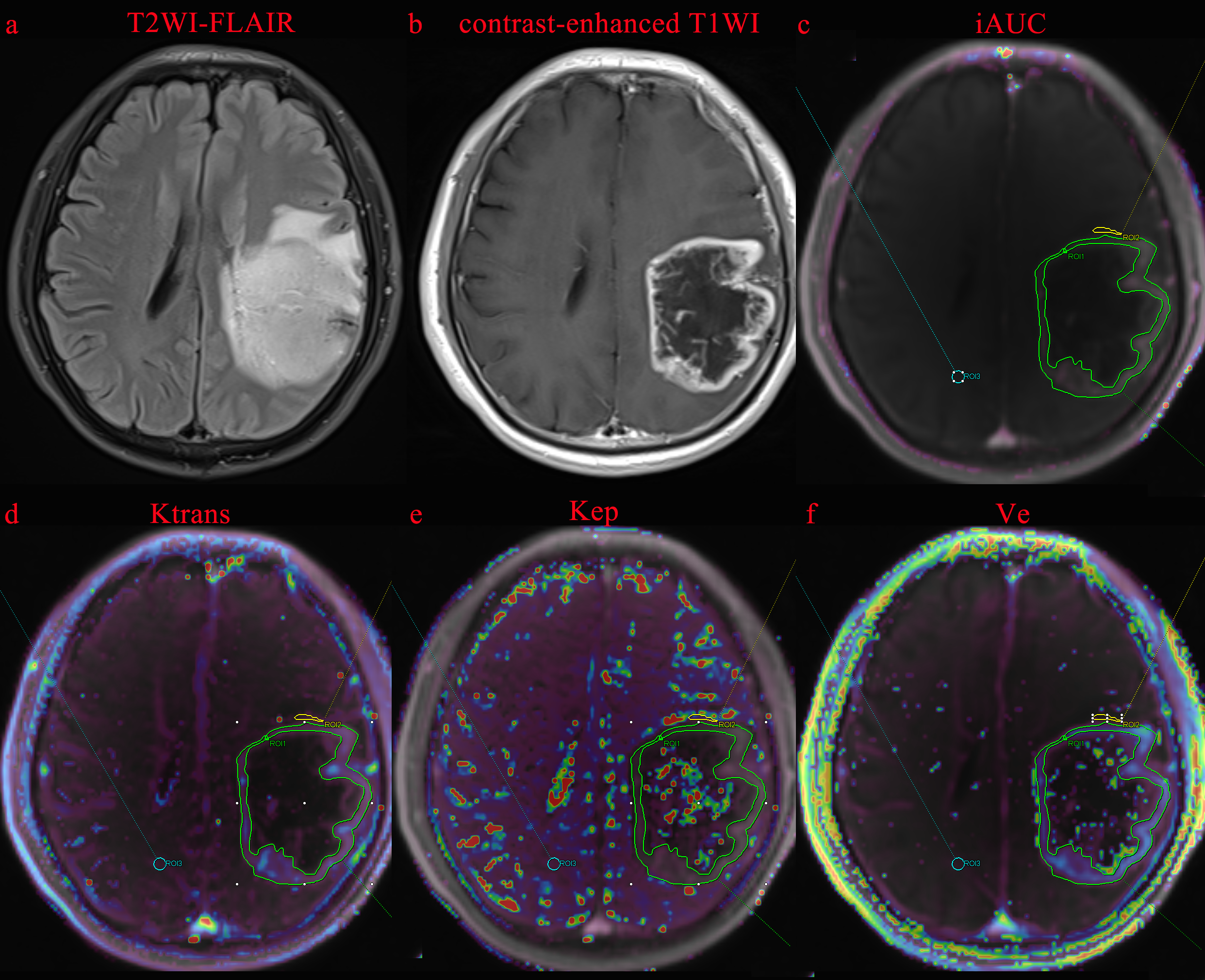
A total of 101 patients with adult-type diffuse gliomas were retrospectively reclassified according to the latest WHO classification criteria in 2021. All patients underwent conventional MRI and DCE-MRI sequence scanning on a 3.0T MR scanner. Volume transfer constant (Ktrans), rate constant for transfer (Kep), extravascular volume (Ve), and the initial area under the enhancement curve (iAUC) were calculated. The regions of interest (ROIs) of all solid components of tumor parenchyma, the peritumoral area and the contralateral normal brain tissues were drawn, as shown in Figure 1 [3]. The average values obtained from ROIs at three consecutive maximal levels of tumors were calculated as the final values for a certain parameter. We used COX or logistic regression analysis to establish predictive models for prognosis and genotype after univariate analysis. AUC, nomograms, and decision curves analysis (DCA) were performed to evaluate prediction models comprehensively.
Results
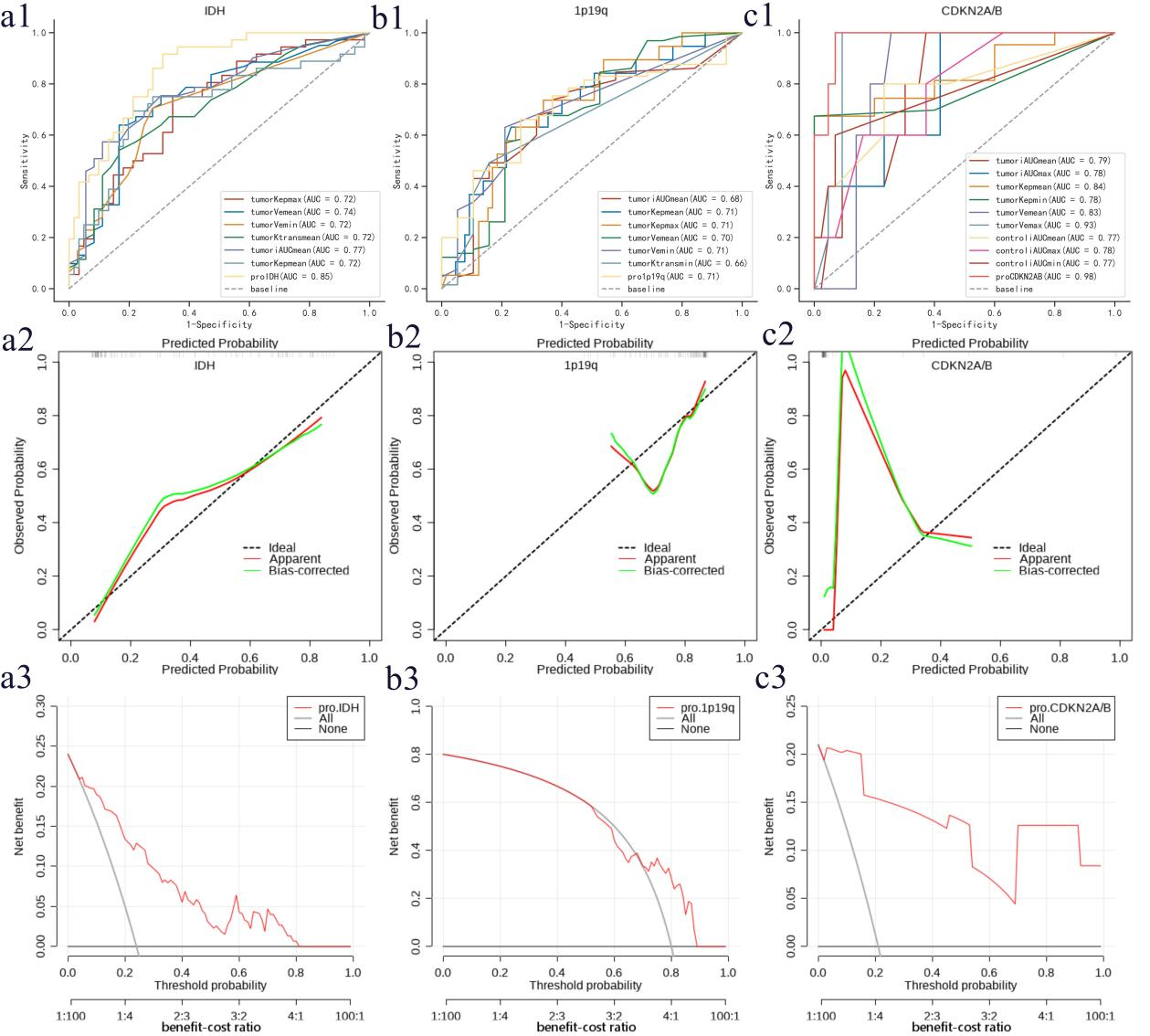
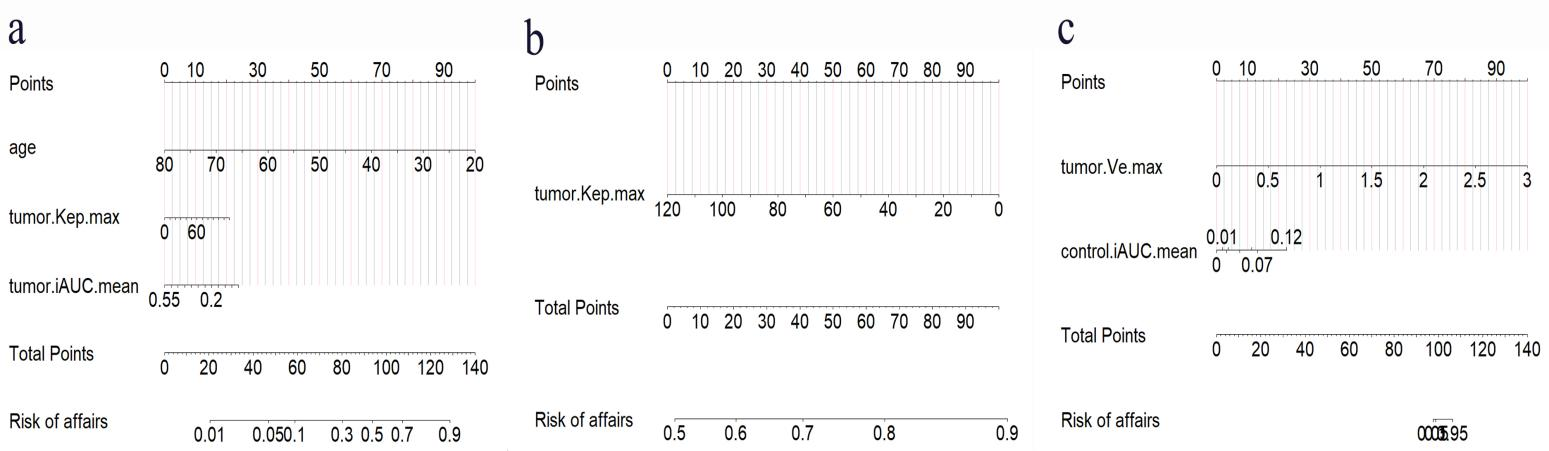
1. ROC analysis showed the diagnostic performance of the model for the DCE-derived parameters in differentiating molecular status of IDH, 1p19q and CDKN2A/B (Figure 2, P<0.05). Tumor.iAUC.mean had the highest AUC of 0.77 (95% confidence interval [CI]: 0.68, 0.87, P<0.001) in IDH mutation prediction. For 1p19q codeletion, tumor.Kep.mean has the highest AUC of 0.71 (95%CI: 0.58, 0.84, P =0 .002). For diagnosing CDKN2A/B homozygous deletion, tumor.Ve.max has the highest AUC of 0.93 (95%CI: 0.86, 1.00) with 100% sensitivity and 91% specificity.
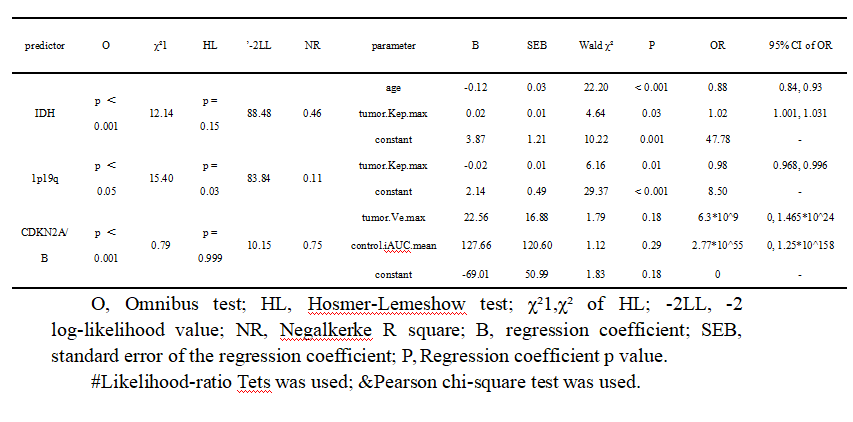
2. According to the logistic regression analysis (Table 1), the variate tumor.Kep.max was an independent predictive impeding factor for predicting 1p19q-codeletion (odds ratio [OR]:0.98, 95%CI: 0.968, 0.996, P=0.01), but an independent promoting factor for predicting IDH-mutant (OR:1.02, 95%CI: 1.001, 1.031, P=0.03).
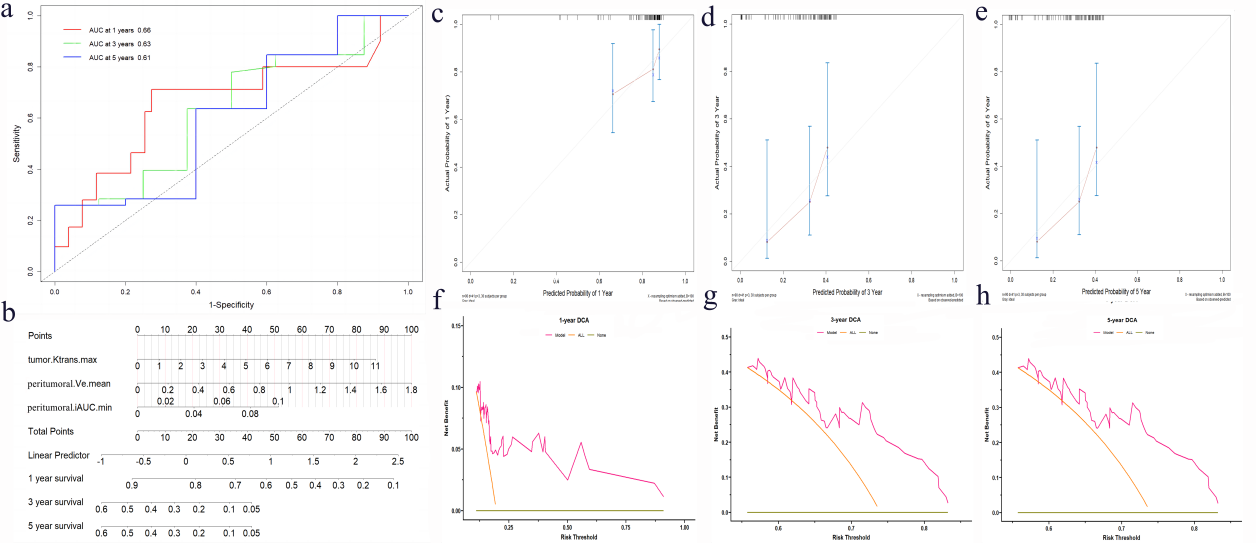
3. The final multivariate cox regression model showed that tumor.Ktrans.max (hazard ratio [HR]:1.29, 95%CI: 1.03, 1.61, P=0.02) and peritumoral.Ve.mean (HR: 5.84, 95%CI: 1.47, 23.29, P=0.01) were independent prognostic risk factors for glioma patients. Time-dependent ROC analysis revealed that AUC values of patients for 1-, 3-, and 5-year survival were 0.66, 0.63, and 0.61, respectively (Figure 3).
4. The nomograms, calibration curves, and DCA showed for prediction models based on the DCE-derived parameters were showen in Figure 2-4.
Discussion
Our results showed DCE-derived parameters such as the max Kep or max Ktrans have
good diagnostic performance in predicting prognosis and identifying genetic status of IDH, 1p19q and CDKN2A/B. We also visualized diagnostic and prognostic prediction models by nomograms, which were relatively quantitative and intuitive at acceptable levels.
In our study, tumor.Kep.max seems to be the most important parameter as it was an independent predictive factor in diagnostic prediction models for identifying IDH and 1p19q status of gliomas. Kep reflects the rate at which contrast agent transfers from the extravascular extracellular compartments back to the the intravascular space, and is known to reflect the vessel permeability and surface area [4]. The higher the and infiltrative degree of the tumor, the stronger permeability and the larger surface area, thus the easier the transferred contrast agent accumulate in the extravascular compartment, leading to delayed reverse transfer and decreased rate. Therefore, lower Kep may indicate IDH-wild genotype of glioma [5]. CDKN2A homozygous deletion may contribute to uncontrolled tumor cell proliferation and is a strong adverse prognosis factor in diffuse malignant IDH-mutant gliomas [6]. Our study showed Ve derived from tumor is the independent positive prediction index for CDKN2A/B homozygous deletion. We speculated the possible reasons is that Ve is correlated with cellularity and mitotic activity [7]. Our results also showed higher Ktrans are associated with worse overall survival or higher HR [8], and Ve and iAUC derived from peritumoral areas are independent negative prognostic factor.
Conclusion
This study comprehensively evaluated the clinical utility of DCE-MRI and provided prediction models that are convenient for clinicians to use. Further studies will enroll the recruitment of a larger sample size and expand genotype predictions, in order to provide one-stop service that enables to get as comprehensive clinical concerned information as possible through a single examination.
Acknowledgements
No acknowledgement found.References
1. Wen PY, Packer RJ. The 2021 WHO Classification of Tumors of the Central Nervous System: clinical implications. Neuro Oncol. 2021; 23:1215-1217.
2. Weller M, van den Bent M, Preusser M, et al. EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat Rev Clin Oncol. 2021; 18:170-186.
3. Zeng S, Ma H, Xie D, et al. Quantitative susceptibility mapping evaluation of glioma. Eur Radiol. 2023; 33:6636-6647.
4. Zhao M, Guo LL, Huang N, et al. Quantitative analysis of permeability for glioma grading using dynamic contrast-enhanced magnetic resonance imaging. Oncol Lett. 2017; 14:5418-5426.
5. Zhao J, Wang Y, Li X, et al. Comparative analysis of the diffusion kurtosis imaging and diffusion tensor imaging in grading gliomas, predicting tumour cell proliferation and IDH-1 gene mutation status. J Neurooncol. 2019; 141:195-203.
6. Mills SJ, du Plessis D, Pal P, et al. Mitotic Activity in Glioblastoma Correlates with Estimated Extravascular Extracellular Space Derived from Dynamic Contrast-Enhanced MR Imaging. AJNR Am J Neuroradiol. 2016; 37:811.
7. Choi YS, Kim DW, Lee SK, et al. The Added Prognostic Value of Preoperative Dynamic Contrast-Enhanced MRI Histogram Analysis in Patients with Glioblastoma: Analysis of Overall and Progression-Free Survival. AJNR Am J Neuroradiol. 2015; 36:2235.
8. Nguyen TB, Cron GO, Mercier JF, et al. Preoperative Prognostic Value of Dynamic Contrast-Enhanced MRI–Derived Contrast Transfer Coefficient and Plasma Volume in Patients with Cerebral Gliomas. AJNR Am J Neuroradiol. 2015; 36:63.
Figures