3586
Reevaluating the Role of T2/FLAIR Mismatch Sign: Improving Diagnostic Accuracy With Qualitative MRI Features?1Radiology, Yale School of Medicine, New Haven, CT, United States, 2Radiology, University of Leipzig, Leipzig, Germany, 3Pathology, Yale School of Medicine, New Haven, CT, United States, 4Neuroradiology, The Ohio State University School of Medicine, Columbus, OH, United States
Synopsis
Keywords: Tumors (Pre-Treatment), Cancer, IDH-Mutation, 1p/19q Codeletion
Motivation: There is a critical need for improved diagnostic precision in distinguishing between IDH-mutant, 1p/19q non-codeleted astrocytomas and 1p/19q co-deleted oligodendrogliomas. While the T2/FLAIR-mismatch sign is specific for IDH-mutant astrocytomas, its limited sensitivity calls for enhanced diagnostic methods in glioma cohorts.
Goal(s): To evaluate the role of T2/FLAIR-mismatch in combination with qualitative VASARI features to classify IDH-mutant glioma.
Approach: We analyzed VASARI features and the presence of T2/FLAIR-mismatch in 179 IDH-mutant gliomas and determined the predictive accuracy of these features.
Results: Findings indicate the limitations of the T2/FLAIR-mismatch sign for accurate preoperative diagnosis, emphasizing the need for refined noninvasive methods to enhance diagnostic accuracy.
Impact: This research underscores the critical need for improved diagnostic tools in distinguishing glioma subtypes, as the T2/FLAIR-mismatch sign exhibits limitations, risking misclassification. Addressing these challenges is essential for accurate patient management and treatment planning in the context of IDH-mutant gliomas.
BACKGROUND OR PURPOSE
IDH-mutant gliomas share many similarities on MRI and histopathology but have distinct differences in their survival based on their molecular subtypes (s. Figure 1) [1-3]. Previous research has highlighted the significance of accurate molecular diagnosis between astrocytomas (IDH-mutant, 1p/19q non co-deleted), and oligodendrogliomas (IDH-mutant, 1p/19q co-deleted) due to its impact on patient outcomes and treatment strategies. Histological diagnosis is prone to sampling errors owing to insufficient biopsy specimens or heterogeneous tissue samples. Noninvasive diagnosis of these molecular subtypes before surgery can change treatment planning and involvement of patients in neoadjuvant clinical trials [4], necessitating the development of noninvasive methods for preoperative grading. In clinical practice, the T2/FLAIR-mismatch has served as an imaging feature to distinguish between these two tumor entities, however, its application requires precision, as there have been instances of false positives, particularly among IDH-mutant, 1p/19q co-deleted oligodendrogliomas. Its diagnostic performance for the prediction of IDH-mutation (non-1p/19q-co-deleted) in a cohort of gliomas showed sensitivity of 100%, however, specificity was shown to be at 42% [5-7]. It is worth noting that intratumoral cysts and necrosis can potentially confound the interpretation of T2/FLAIR mismatch and thus should not be considered indicative of such mismatches [8].In this study, we evaluated the role of combined T2/FLAIR-mismatch sign and qualitative imaging features in VASARI format in differentiating two similar tumor entities: astrocytomas (IDH-mutant, 1p/19q non co-deleted), and oligodendrogliomas (IDH-mutant, 1p/19q co-deleted).
METHODS
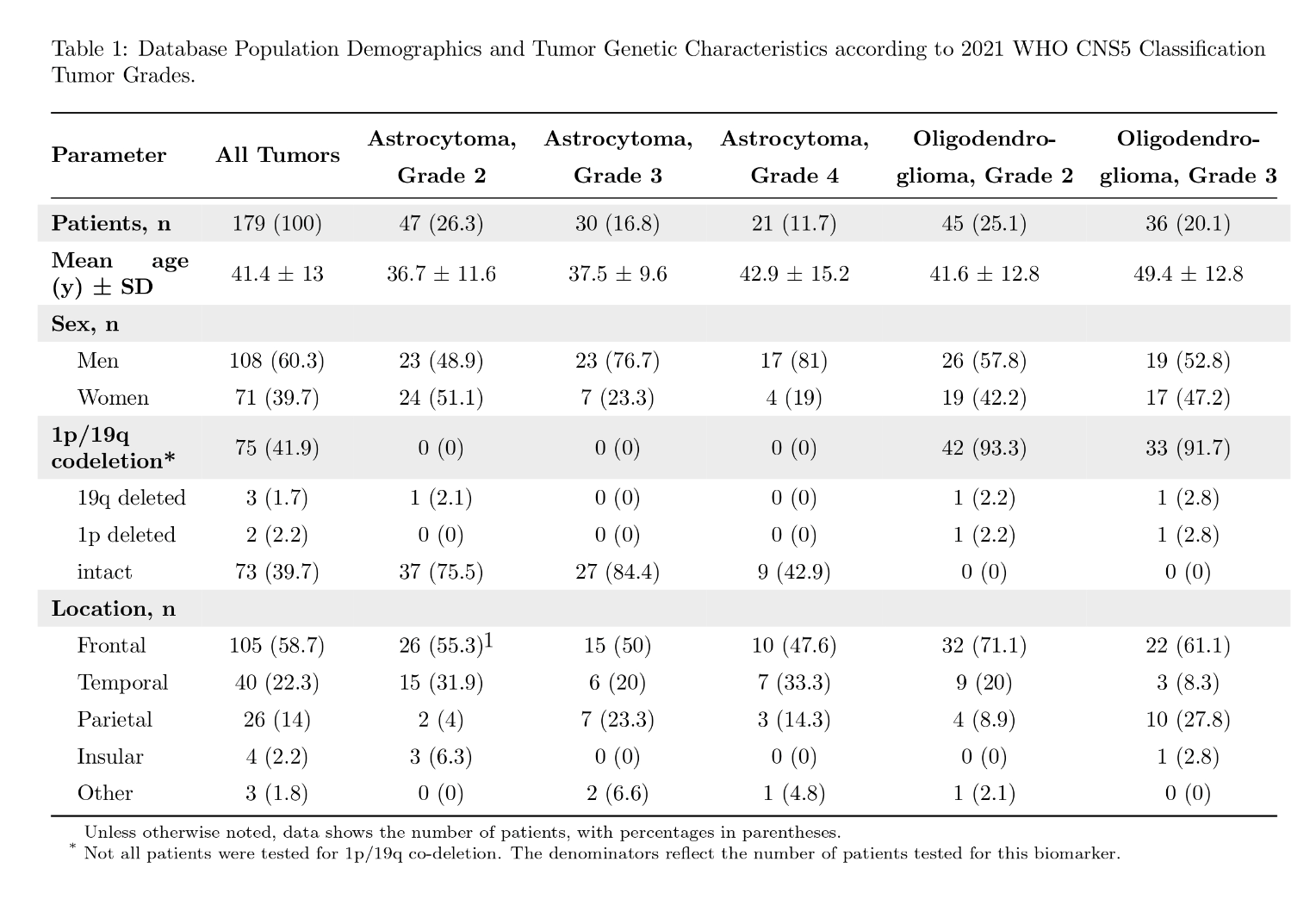
In this retrospective study, a total of 179 patients who received surgical and/or radiotherapeutic treatment for primary brain tumors at the study institution between January 2000 and December 2023 were reviewed preoperatively (s. Table 1). Patients with IDH-mutant grade 2-4 astrocytomas and IDH-mutant, 1p/19q co-deleted grade 2-3 oligodendrogliomas, as confirmed by histopathology according to the 2021 WHO CNS5 classification criteria [9] and with available pretreatment MRI scans were included. For the assessment of the VASARI features and the T2/FLAIR mismatch sign, two board-certified neuroradiologists (F.M., B.S.) conducted independent assessments of preoperative imaging to diagnose glioma subtype and assess the T2/FLAIR mismatch sign. The included sequences were FLAIR, T1WI, and T2WI. The T2/FLAIR mismatch sign was evaluated based on predefined criteria, with cases being categorized into one of three groups: positive mismatch, negative mismatch, or partial mismatch (the lack of hyperintense rim on FLAIR). The readers were blinded to the clinical data and the diagnosis of each case.The statistical analysis involved descriptive statistics and the Chi-square test, a p-value<0.05 was considered statistically significant.RESULTS
The results showed that the diagnostic accuracy for distinguishing between these two tumor entities using the T2/FLAIR-mismatch sign was limited, with fair Cohen's Kappa for glioma subtype diagnosis (Cohen’s κ = 0.27) and moderate agreement for T2/FLAIR mismatch sign (Cohen’s κ = 0.43). The accuracies of correct diagnosis varied across different tumor grades, with only a minority of cases being correctly diagnosed: 37.6% of grade 2 astrocytomas, 20% of grade 3 astrocytomas, 37.1% of grade 4 astrocytomas, 41.3% of grade 2 oligodendrogliomas, and 32% of grade 3 oligodendrogliomas were correctly diagnosed. Astrocytoma, grade 3 were diagnosed in 32.1% as grade 2; grade 4 in 23.7% as oligodendroglioma, grade 3; oligodendroglioma, grade 2 in 34.9% as astrocytoma, grade 2; and oligodendroglioma, grade 3 in 34.9% as grade 2.Furthermore, the ability to correctly differentiate between IDH mutant, 1p/19q codeleted and non-codeleted gliomas using VASARI features and the T2/FLAIR-mismatch sign was limited. Diagnostic accuracy for astrocytomas was at 68.1%, and for oligodendrogliomas 62.5%. Classic T2/FLAIR mismatch sign was found in 8.1% of the grade 2 oligodendrogliomas and in 9.1% of grade 3 oligodendrogliomas. Of these oligodendrogliomas with positive T2/FLAIR mismatch sign, radiologists misdiagnosed 55.6% of them as grade 2 astrocytoma, 16.7% as grade 3 astrocytoma, and 10% as grade 3 oligodendroglioma or grade 4 astrocytoma. Partial T2/FLAIR mismatch sign was seen in 10.1% of the cases.
The following VASARI features revealed significant association with tumor subtype using Chi-Square test (p<0.05): Proportion necrosis (Chi-square = 48), enhancement quality (Chi-square = 38.5), pial invasion (Chi-square = 23.9), proportion enhancing (Chi-square = 42.9), thickness of enhancing margin (Chi-square = 43.3), proportion of non-contrast-enhancing tumor (Chi-square = 40), deep WM invasion (Chi-square = 11.9), definition of non-enhancing margin (Chi-square = 11.2), proportion edema (Chi-square = 26.4, p=0.04).
CONCLUSIONS
We show that the T2/FLAIR-mismatch sign is limited in distinguishing between IDH-mutant, 1p/19q non-codeleted astrocytomas and IDH-mutant, 1p/19q co-deleted oligodendrogliomas based on preoperative MRI imaging. While VASARI features are associated with tumor subtype, using these qualitative methods does not significantly improve preoperative disgnosis and pathological diagnosis is recommended for patient management.Acknowledgements
No acknowledgement found.References
- van den Bent MJ, Chang SM. Grade II and III Oligodendroglioma and Astrocytoma. Neurol Clin. 2018;36(3):467-484. doi:10.1016/j.ncl.2018.04.005
- White ML, Zhang Y, Kirby P, Ryken TC. Can Tumor Contrast Enhancement Be Used as a Criterion for Differentiating Tumor Grades of Oligodendrogliomas? AJNR Am J Neuroradiol. 2005;26(4):784-790.
- Juratli TA, Tummala SS, Riedl A, et al. Radiographic assessment of contrast enhancement and T2/FLAIR mismatch sign in lower grade gliomas: correlation with molecular groups. J Neurooncol. 2019;141(2):327-335. doi:10.1007/s11060-018-03034-6
- Bunse L, Rupp AK, Poschke I, et al. AMPLIFY-NEOVAC: a randomized, 3-arm multicenter phase I trial to assess safety, tolerability and immunogenicity of IDH1-vac combined with an immune checkpoint inhibitor targeting programmed death-ligand 1 in isocitrate dehydrogenase 1 mutant gliomas. Neurol Res Pract. 2022;4(1):20. doi:10.1186/s42466-022-00184-x
- Patel SH, Poisson LM, Brat DJ, et al. T2–FLAIR Mismatch, an Imaging Biomarker for IDH and 1p/19q Status in Lower-grade Gliomas: A TCGA/TCIA ProjectT2–FLAIR Mismatch Predicts Low-Grade Glioma Molecular Class. Clin Cancer Res. 2017;23(20):6078-6085.
- Deguchi S, Oishi T, Mitsuya K et al. Clinicopathological Analysis of T2-FLAIR. Scientific Reports. 2020;10(1):1-6. doi:10.1038/s41598-020-67244-7
- Juratli T, Tummala S, Riedl A et al. Radiographic Assessment of Contrast Enhancement and T2/FLAIR Mismatch Sign in Lower Grade Gliomas: Correlation with Molecular Groups. J Neurooncol. 2018;141(2):327-35. doi:10.1007/s11060-018-03034-6 - Pubmed
- Jain R, Johnson DR, Patel SH, et al. “Real world” use of a highly reliable imaging sign: “T2-FLAIR mismatch” for identification of IDH mutant astrocytomas. Neuro-Oncol. 2020;22(7):936-943. doi:10.1093/neuonc/noaa041
- Louis DN, Perry A, Wesseling P, et al. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro-Oncol. 2021;23(8):1231-1251. doi:10.1093/neuonc/noab106
Figures
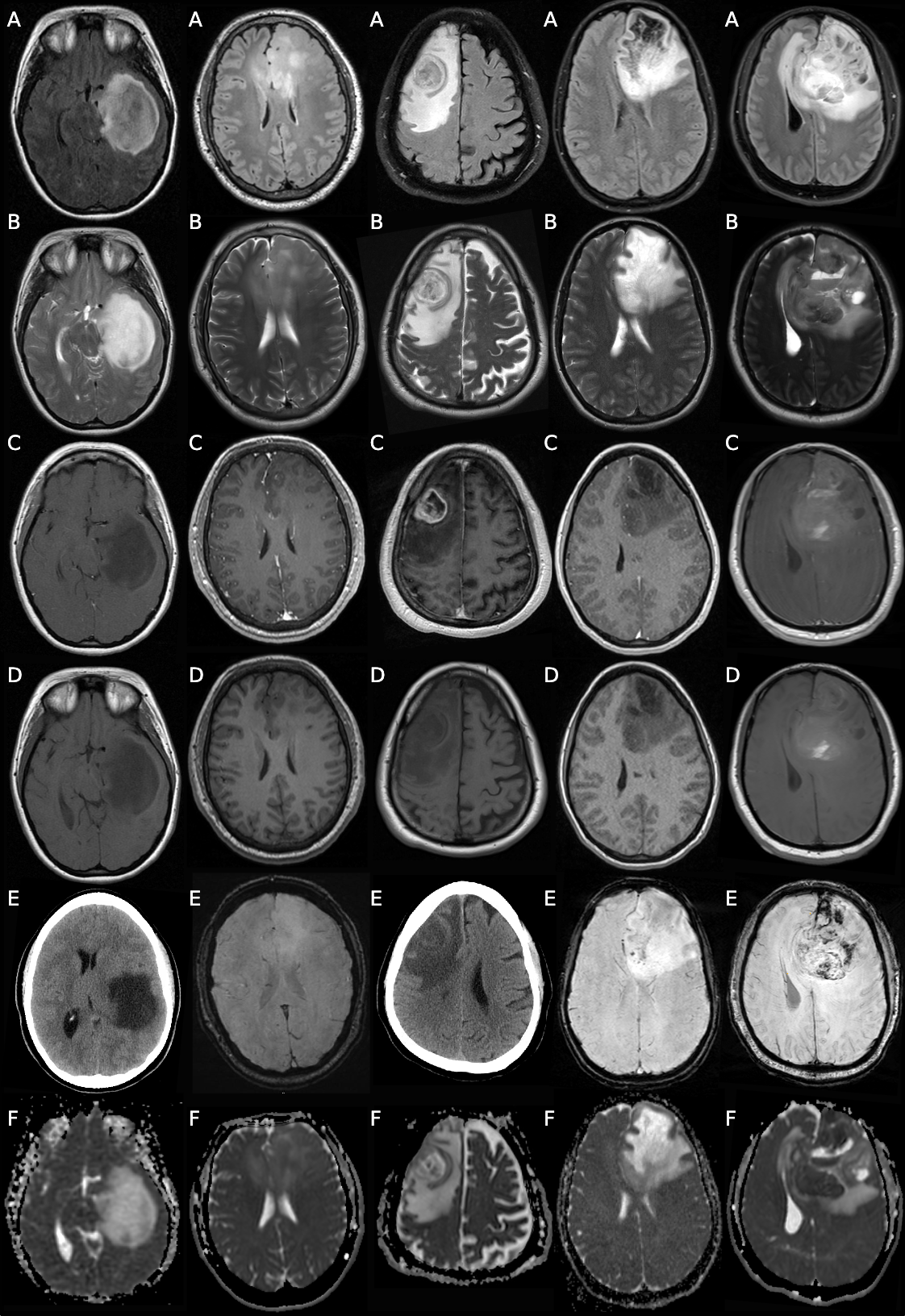
Spectrum of imaging features of IDH-mutant glioma subtypes (from left to right): IDH-mutant 1p/19q non co-deleted astrocytoma WHO CNS5 grade 2-4, and 1p/19q co-deleted oligodendroglioma WHO CNS5 grade 2-3. Rows (top to bottom): FLAIR, T2WI, T1 post-contrast (PGSE, PGGE), T1WI, SWI/CT (in column 1 and 3), and ADC.