3585
Discordant Molecular, Imaging, and Survival Manifestations between Molecular Glioblastomas and Histological Glioblastomas1Radiology, Yonsei University College of Medicine, Seoul, Korea, Republic of, 2NYU Langone, New York, NY, United States
Synopsis
Keywords: Tumors (Pre-Treatment), Brain, glioma; glioblastoma; molecular glioblastoma
Motivation: Whether molecular GBMs are equivalent to early histological GBMs are controversial.
Goal(s): To compare the clinicopathologic, imaging, surgical factors, and prognosis between molecular GBMs and histological GBMs.
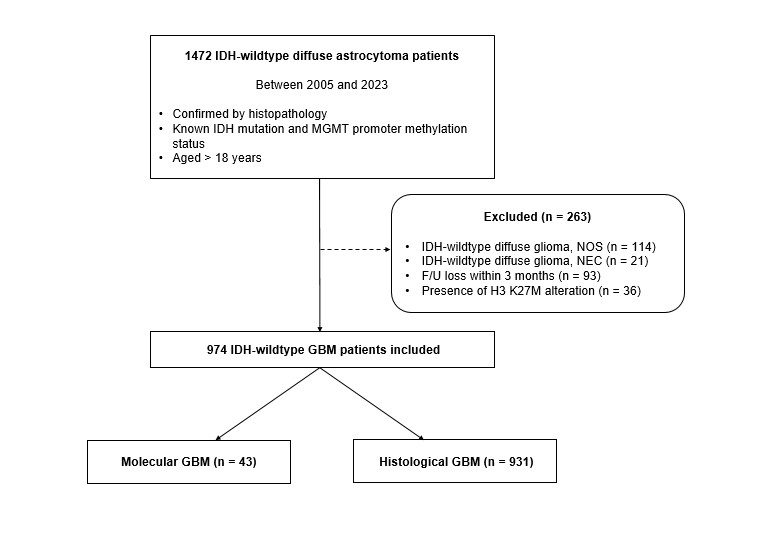
Approach: Retrospective chart and imaging review was performed in 974 IDH-wildtype GBM patients (43 molecular GBMs and 931 histological GBMs) from a single institution.
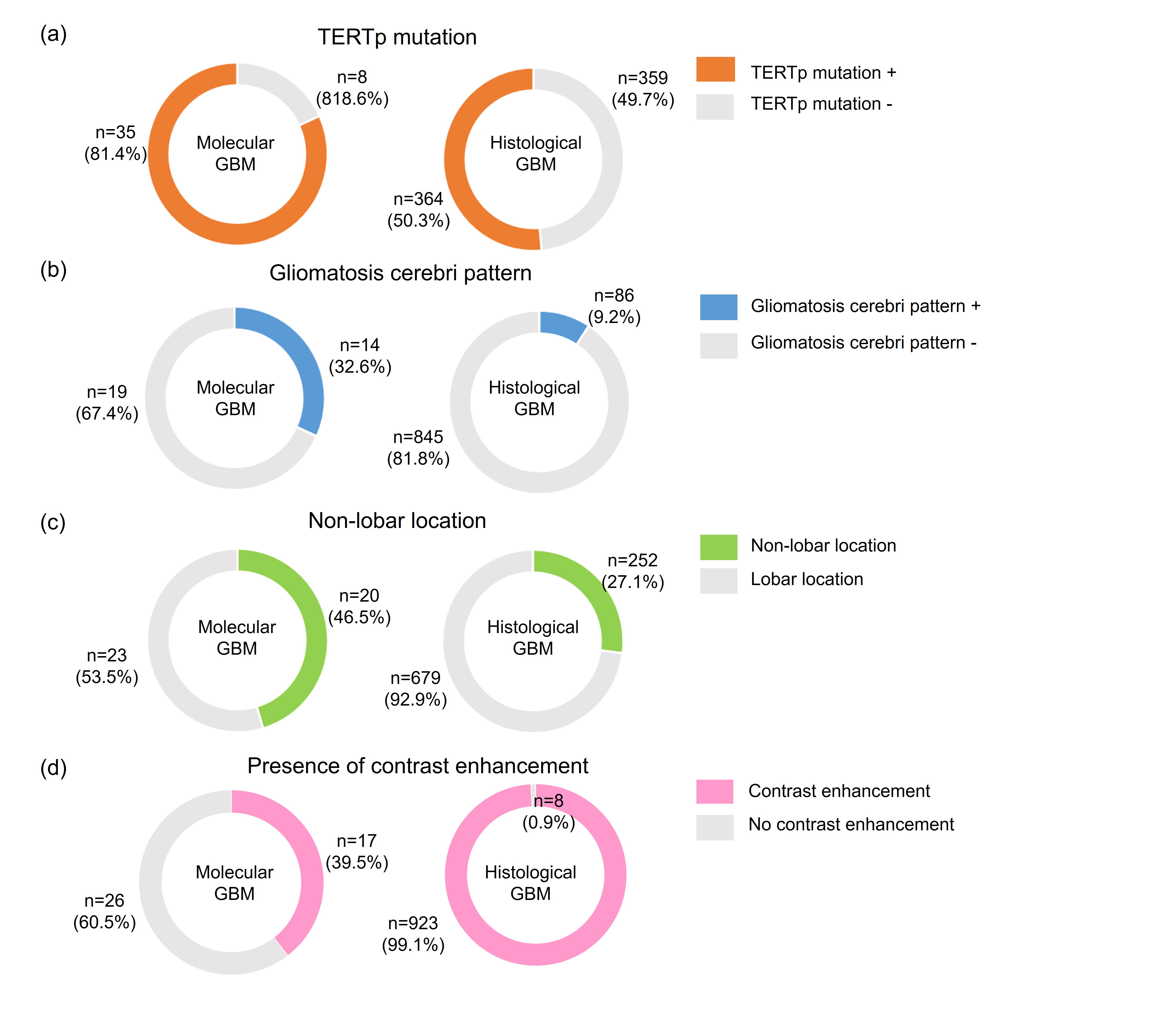
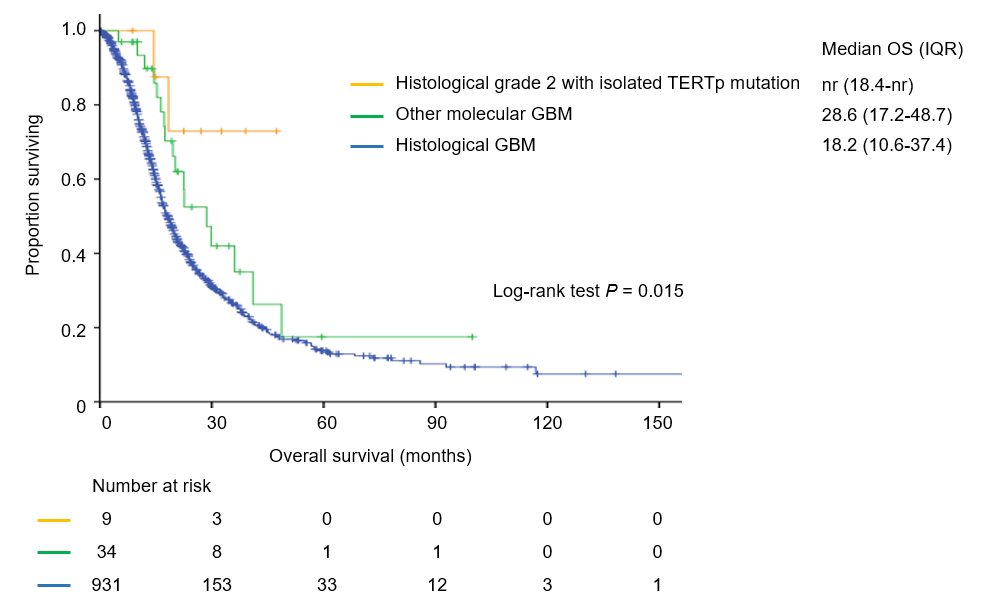
Results: Molecular GBMs were significantly younger with higher rate of TERTp, higher incidence of gliomatosis cerebri and non-lobar location compared with histological GBMs, resulting in less aggressive resection. Survival was significantly longer in molecular GBM, which was attributed to the longer OS in histological grade 2 molecular GBMs with isolated TERTp mutation.
Impact: Discordant clinicopathologic, imaging, and surgical features suggest molecular GBMs may not be equivalent to early histological GBMs. Histological grade 2 molecular GBMs with isolated TERTp mutation may not be sufficient to assume an aggressive clinical behavior similar to histological GBM.
Background
Whether molecular glioblastomas (GBMs) are equivalent to early histological GBMs are controversial. This study aimed to compare the clinicopathologic, imaging, surgical factors, and prognosis between molecular GBMs and histological GBMs to resolve this controversy.Methods
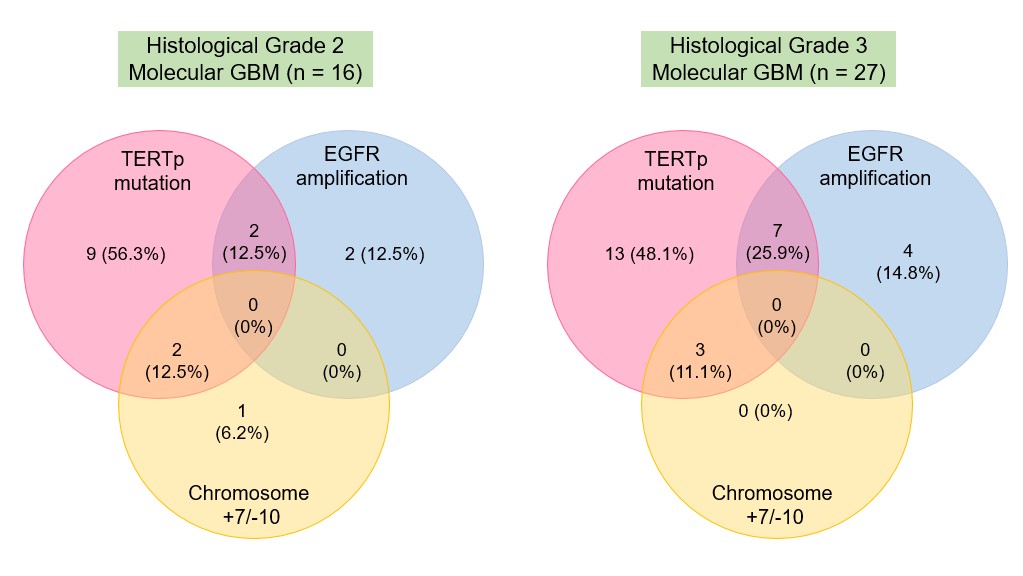
Retrospective chart and imaging review was performed in 974 IDH-wildtype GBM patients (43 molecular GBMs and 931 histological GBMs) from a single institution between 2005 and 2023. Following previous criteria, patients with molecular GBM were divided into histological grade 2 with isolated TERTp mutation and other molecular GBMs (histological grade 3 with isolated TERTp mutation and histological grade 2 or 3 with EGFR amplification and/or chromosome +7/-10).Results
Molecular GBM patients were substantially younger (58.1 vs 62.3, P = 0.036) with higher rate of TERTp mutation (81.4% vs 51.4%, P < 0.001) compared with histological GBMs. Imaging showed higher incidence of gliomatosis cerebri pattern (32.6% vs 9.2%, P < 0.001) and non-lobar location (46.5% vs 27.1%, P = 0.005) of molecular GBMs compared with histological GBMs, which resulted in lesser extent of resection (P < 0.001) in these patients. The survival was significantly different between molecular GBM and histological GBM (P = 0.006), with median OS of 29.8 in molecular GBM and 18.6 months in histological GBM. Further analysis indicated that this survival difference can be attributed to the longer OS in histological grade 2 molecular GBMs with isolated TERTp mutation compared with histological GBMs (P = 0.030).Conclusion
The significantly younger age of diagnosis, higher rate of TERTp mutation, and higher incidence of imaging manifestation in terms of gliomatosis cerebri pattern and non-lobar location in molecular GBM leading to lesser EOR suggests molecular GBMs may not be equivalent to early histological GBMs. Histological grade 2 molecular GBMs with isolated TERTp mutation may not be sufficient to assume an aggressive clinical behavior similar to histological GBMs.Acknowledgements
None.References
Brat DJ, Aldape K, Colman H, et al. cIMPACT-NOW update 3: recommended diagnostic criteria for "Diffuse astrocytic glioma, IDH-wildtype, with molecular features of glioblastoma, WHO grade IV". Acta Neuropathol. 2018; 136(5):805-810.
Berzero G, Di Stefano AL, Ronchi S, et al. IDH-wildtype lower-grade diffuse gliomas: the importance of histological grade and molecular assessment for prognostic stratification. Neuro Oncol. 2021; 23(6):955-966.
Nakasu S, Deguchi S, Nakasu Y. IDH wild-type lower-grade gliomas with glioblastoma molecular features: a systematic review and meta-analysis. Brain Tumor Pathol. 2023; 40(3):143-157.
Aibaidula A, Chan AK, Shi Z, et al. Adult IDH wild-type lower-grade gliomas should be further stratified. Neuro Oncol. 2017; 19(10):1327-1337.
Zhang Y, Lucas CG, Young JS, et al. Prospective genomically guided identification of "early/evolving" and "undersampled" IDH-wildtype glioblastoma leads to improved clinical outcomes. Neuro Oncol. 2022; 24(10):1749-1762.
Figures