3584
Pre-RT Fiber Density-Weighted White Matter Pathlength Maps Can Predict Tumor Progression in Patients with Glioblastoma Multiforme1UCSF/UC Berkeley Graduate Program in Bioengineering, University of California, San Francisco, San Francisco, CA, United States, 2Radiation Oncology, University of California, San Francisco, San Francisco, CA, United States, 3Radiology and Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States
Synopsis
Keywords: Tumors (Post-Treatment), Cancer, DTI, AI, Progression, GBM
Motivation: Utilizing the knowledge of glioma cells' infiltration along white matter pathways to better predict GBM progression.
Goal(s): To enhance GBM progression prediction by analyzing the map of adjacent white matter fibers and building models to incorporate that map with anatomical MR.
Approach: Developed a novel algorithm, DW-WMPL, from Diffusion-Tensor Imaging data that adjusts white matter fiber lengths to reveal possible tumor advancement. Employed deep learning models to predict progression with anatomical MRI and DW-WMPL maps.
Results: DW-WMPL-enhanced deep learning models achieved higher precision in tumor delineation and reduced normal brain inclusion versus the standard 2cm radiation margin.
Impact: The introduction of density-weighted white-matter path-length maps provides valuable insights into tumor cell migration, significantly refining GBM progression prediction. This advancement indicates a pivotal step towards personalized, more effective radiation therapy planning.
Introduction
Histopathological evidence suggests that glioma tumor cells tend to migrate along large white matter bundles [1-4]. Leveraging peritumoral white matter fiber bundles to predict the trajectory of tumor cells beyond surgical margins and generate an anisotropic expansion of the radiation therapy (RT) target volume could enhance target delineation, improving tumor control while minimizing the exposure of normal brain to ionizing radiation. This study developed an innovative density-weighted white-matter path-length (DW-WMPL) algorithm from Diffusion-Tensor Imaging (DTI) that adjusts the length of viable fiber segments based on tract density, prioritizing the preservation of major fibers. A deep-learning (DL) model was then trained to predict GBM recurrence from pre-treatment MRI scans that included DW-WMPL maps. We hypothesize that this new mapping of white-matter bundles prior to RT will correlate with subsequent tumor recurrence and improve the prediction performance of a segmentation-based DL model.Methods
Subjects: Longitudinal MRI exams from 57 patients with GBM were retrospectively analyzed prior to surgery, immediately post-op, and at the time of recurrence.Image Acquisition: Imaging was performed on a 3T GE scanner using an eight-channel phased-array head-coil. Standard anatomical imaging included T2-weighted FLAIR and pre- and post-contrast 3D T1-weighted IR-SPGR imaging. DTI was acquired with b=2000s/mm2, 55 gradient directions, and 4 b0 images (TR/TE=1000/108ms, voxel size=1.7-2.0×1.7-2.0×2.0-3.0mm).
Processing: After aligning all baseline images to the T1 post-contrast (T1c) images, post-operative anatomical MRI were registered to the pre-operative MR using rigid registration [5]. The post-op cavity was manually delineated and expanded by 5mm to establish an ROI for seeding white-matter tracts. A deformable registration algorithm specifically trained to account for tissue shift after surgery [6] was employed to align the progression scan to pre-op images. A DL-based segmentation model [7] was applied to identify T2-lesion (T2L) and contrast-enhancing lesion (CEL) regions, which were edited if necessary before merging to establish the region of progression.
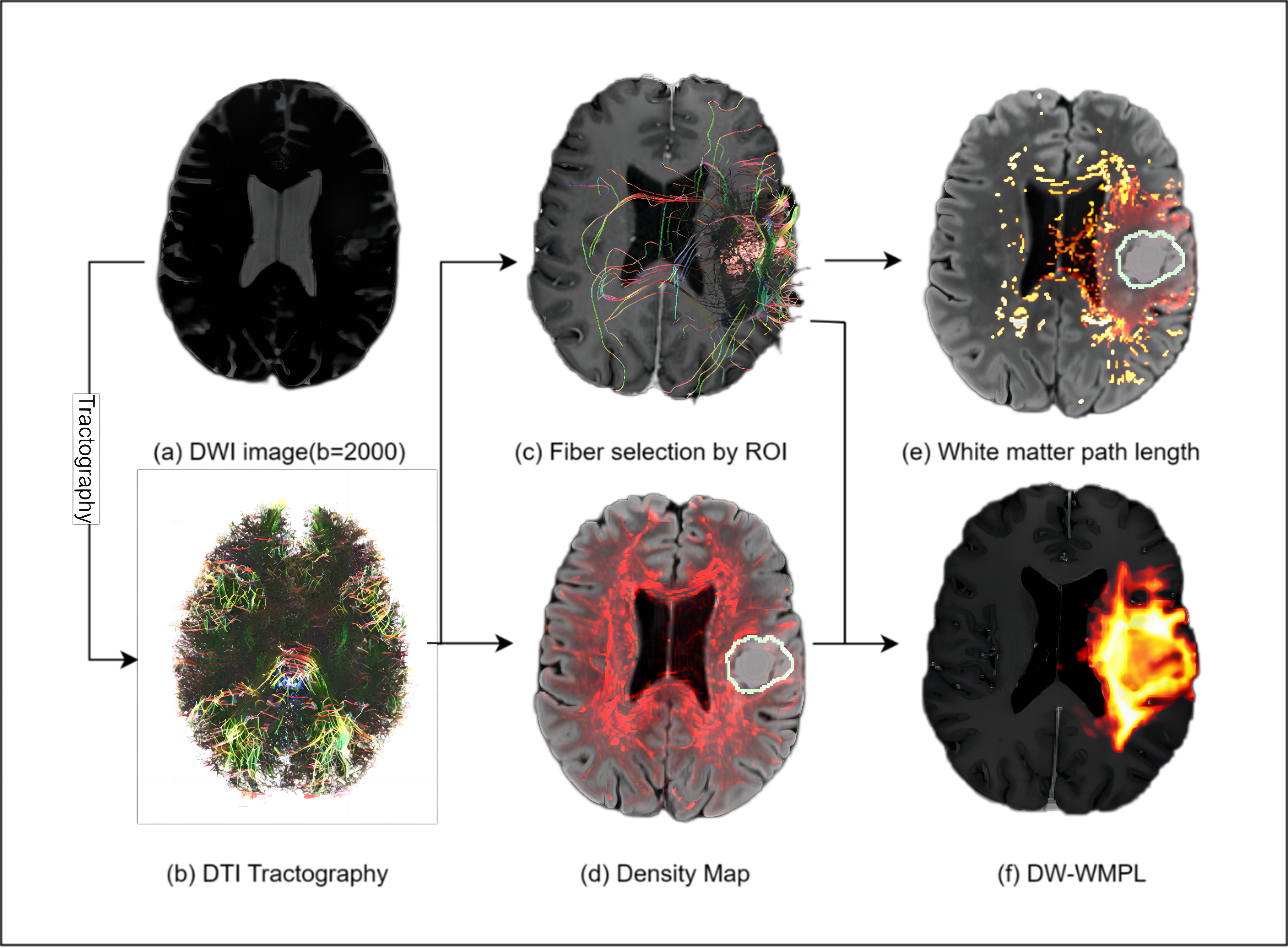
DW-WMPL: DTI Tractography was implemented with DIPY open-source package [8]. The whole-brain streamline was generated using Residual Bootstrap Q-ball [9], with initial seeding and threshold for tracking of fractional anisotropy (FA)>0.15 and tracking angle <60o. [10] A density map was constructed by tallying the trajectories of bundles traversing each voxel. The expanded cavity mask was used to select intersecting bundles that were then weighted by the average track density (Fig.1).
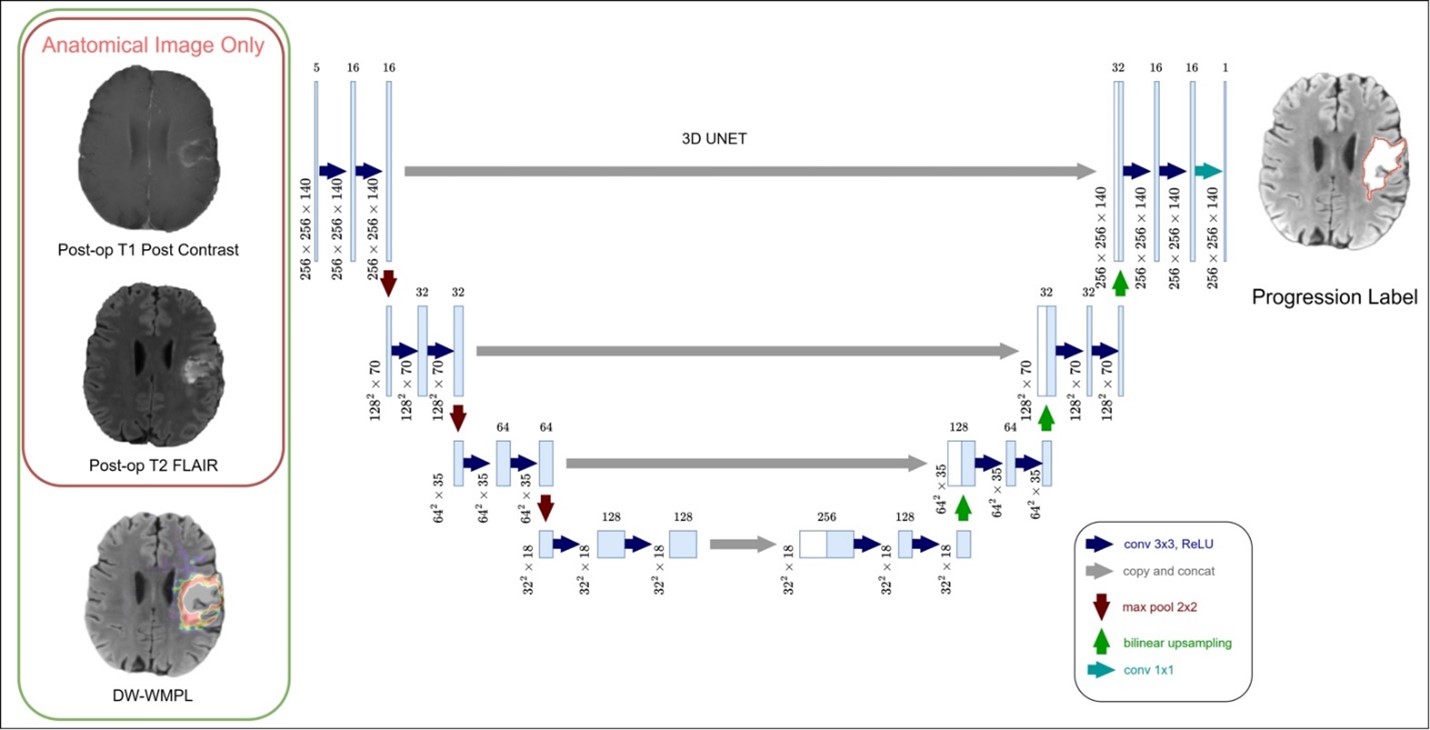
Deep-Learning: Post-op T1c and T2-FLAIR images, along with the pre-surgery DW-WMPL map, were inputs for the DL model, a 3D-UNET network (Fig.2).[11] The CEL and T2L at progression was the ground truth in training. Dice, Tversky, and binary cross-entropy losses were applied in training with learning rate=1e-4 and batch-size=2. Sensitivity, specificity, Dice, and Tversky coefficients were compared among models with 5-fold cross-validation.
Results & Discussion
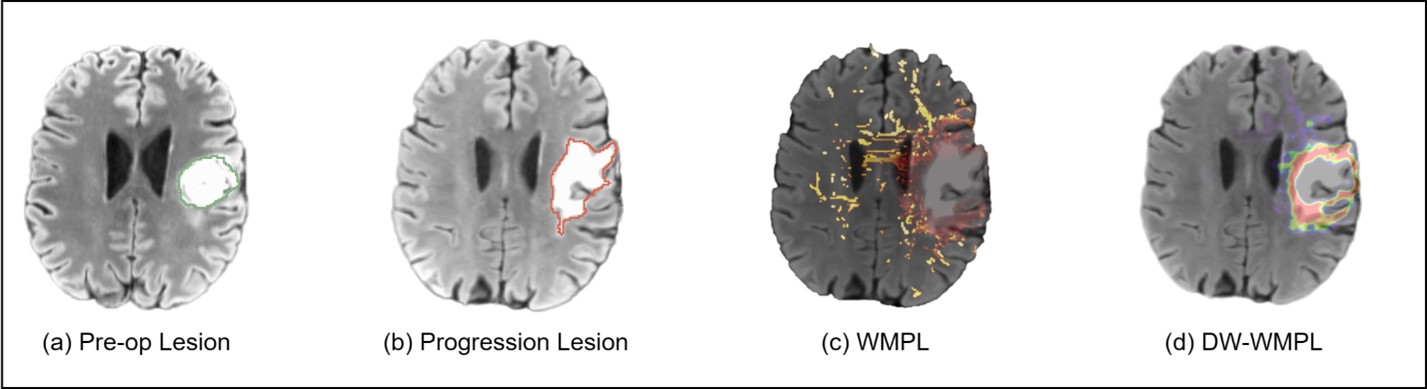
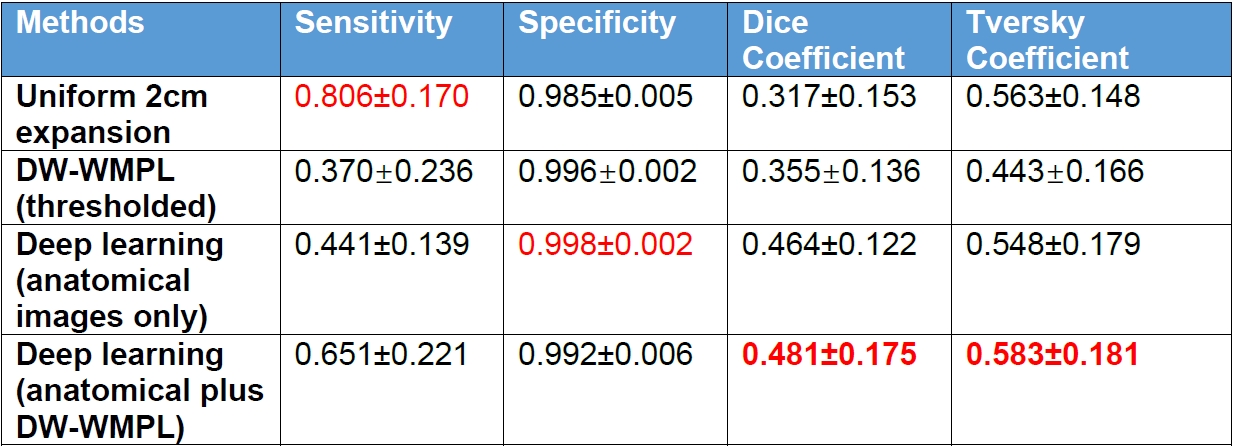
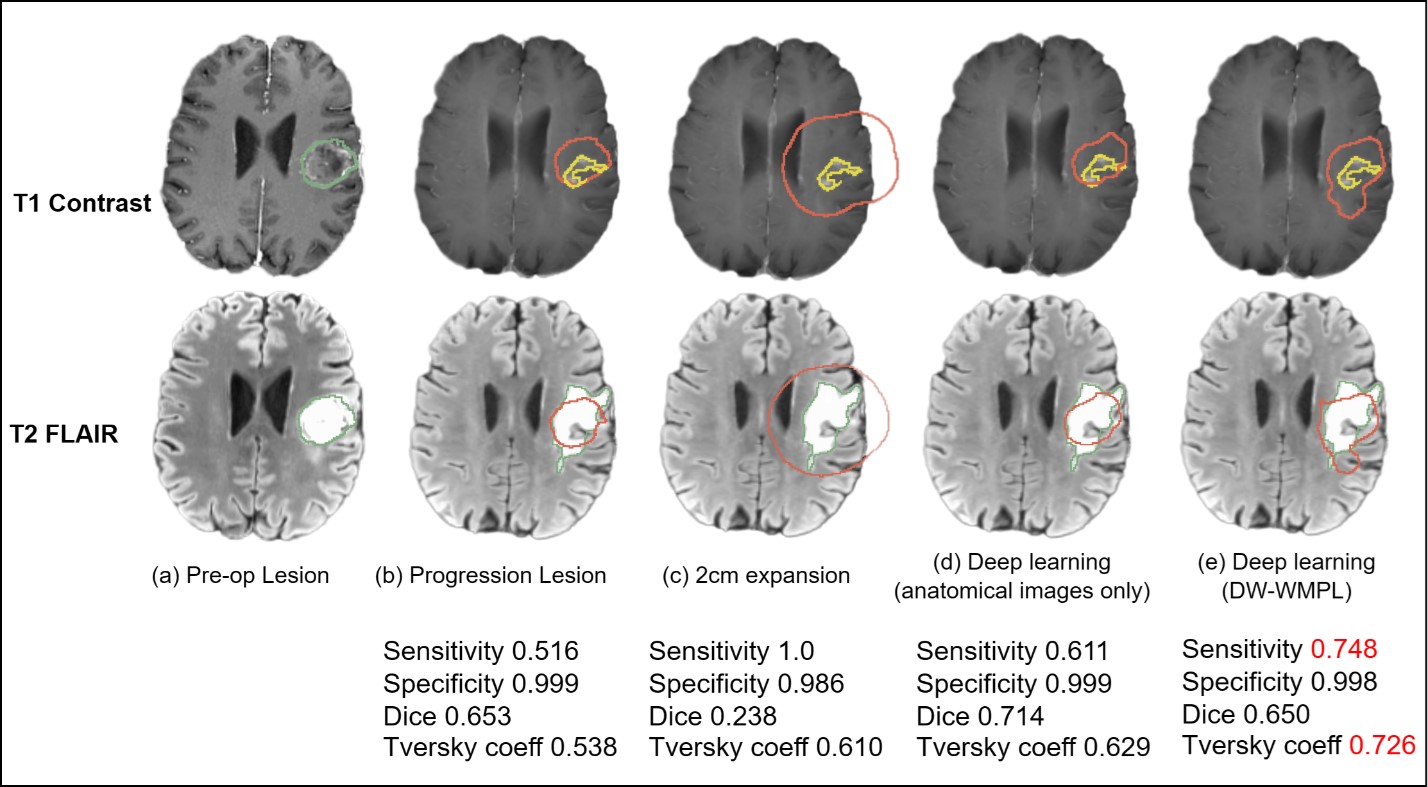
DW-WMPL: Fig.5 demonstrates an example where the DW-WMPL algorithm improves performance and interpretability of WMPL maps. WMPL maps are noisier and include fibers far from lesion ROI. Due to the different density of fibers around the ROI, only those extending in the A/P direction capture where tumor migrated, while the remaining are confined to a limited area around the ROI. The Dice coefficient, however, is only 0.355±0.136 (Fig.4) because the fibers from tractography are sparse and cannot be directly converted into the label mask for quantification.Deep learning: Fig.4 compares the evaluation metrics of our DL model trained only on anatomical images and with DW-WMPL maps to standard care of 2cm expansion of lesion and thresholded DW-WMPL maps. Our model resulted in the best Dice (0.481±0.175) and Tversky coefficients (0.583±0.181). Fig.5 illustrates the results of the different model predictions where the DL model with DW-WMPL map keeps the directionality of tumor migration along fibers towards the posterior side of the brain. Even though the Dice score is lower than the anatomical image DL model, both sensitivity (0.611->0.748) and Tversky coefficient (0.629->0.726) increase, indicating that more of the progressed lesion can be predicted correctly.
Conclusions
This study introduces an algorithm to create a DW-WMPL map from DTI that considers track density, directionality, and length, and demonstrates the feasibility of incorporating it with DL models to improve the prediction of progression in patients with GBM. DL models informed by the DW-WMPL map improved model performance compared to using only anatomical pre-RT MRI in forecasting tumor growth, with greater sensitivity and Tversky coefficient in targeting tumors and sparing healthy brain tissue compared to standard clinical methods. This suggests the algorithm's potential to refine radiation therapy planning once validated in a larger cohort.Acknowledgements
DoD Impact Award W81XWH2210695References
[1] Giese A, Bjerkvig R, Berens ME, Westphal M. Cost of migration: invasion of malignant gliomas and implications for treatment. J Clin Oncol. (2003) 21:1624–36. doi: 10.1200/JCO.2003.05.063
[2] Giese A, Westphal M. Glioma invasion in the central nervous system. Neurosurgery. (1996) 39:235–50. doi: 10.1097/00006123-199608000-00001
[3] Poonnoose SI, Daniel RT. Radiological evidence of glioma invasion of the central nervous system along tracts. Surg Neurol. (2000) 54:194–6. doi: 10.1016/S0090-3019(00)00280-9
[4] Cuddapah VA, Robel S, Watkins S, Sontheimer H. A neurocentric perspective on glioma invasion. Nat Rev Neurosci. (2014) 15:455–65. doi: 10.1038/nrn3765
[5] BRAINSFit: Mutual Information Registrations of Whole-Brain 3D Images, Using the Insight Toolkit, Johnson H.J., Harris G., Williams K., The Insight Journal, 2007.
[6] Tony C. W. Mok, Albert C. S. Chung. Unsupervised Deformable Image Registration with Absent Correspondences in Pre-operative and Post-Recurrence Brain Tumor MRI Scans. MICCAI 2022. eprint arXiv:2206.03900
[7] Aly H Abayazeed, Ahmed Abbassy, Michael Müeller, Michael Hill, Mohamed Qayati, Shady Mohamed, Mahmoud Mekhaimar, Catalina Raymond, Prachi Dubey, Kambiz Nael, Saurabh Rohatgi, Vaishali Kapare, Ashwini Kulkarni, Tina Shiang, Atul Kumar, Nicolaus Andratschke, Jonas Willmann, Alexander Brawanski, Reordan De Jesus, Ibrahim Tuna, Steve H Fung, Joseph C Landolfi, Benjamin M Ellingson, Mauricio Reyes, NS-HGlio: A generalizable and repeatable HGG segmentation and volumetric measurement AI algorithm for the longitudinal MRI assessment to inform RANO in trials and clinics, Neuro-Oncology Advances, Volume 5, Issue 1, January-December 2023, vdac184, https://doi.org/10.1093/noajnl/vdac184
[8] Garyfallidis E, Brett M, Amirbekian B, Rokem A, van der Walt S, Descoteaux M, et al. Dipy a library for the analysis of diffusion MRI data. Front Neuroinf. (2014) 8:8. doi: 10.3389/fninf.2014.00008
[9] Berman J, Chung S, Mukherjee P, Hess CP, Han ET, Henry RG. Probabilistic streamline q-ball tractography using the residual bootstrap. Neuro Image. (2008) 39:215–22. doi: 10.1016/j.neuroimage.2007.08.021
[10] Jordan K, Morin O, Wahl M, Amirbekian B, Chapman C, Owen J, Mukherjee P, Braunstein S, Henry R. An Open-Source Tool for Anisotropic Radiation Therapy Planning in Neuro-oncology Using DW-MRI Tractography. Front Oncol. 2019 Aug 30;9:810. doi: 10.3389/fonc.2019.00810. PMID: 31544062; PMCID: PMC6730482.
[11] Çiçek, O., Abdulkadir, A., Lienkamp, S.S., Brox, T., Ronneberger, O.: 3D U-Net: learning dense volumetric segmentation from sparse annotation. Proc. International Conference on Medical Image Computing and Computer-Assisted Intervention (MICCAI), Springer (2016), pp. 424-432, 10.1007/978-3-319-46723-8_49
Figures