3572
Cardiac MR Fingerprinting with a Low-Rank Reconstruction for Simultaneous T1, T2, and T1ρ Mapping1Biomedical Engineering, University of Michigan, Ann Arbor, MI, United States, 2Radiology, University of Michigan, Ann Arbor, MI, United States
Synopsis
Keywords: MR Fingerprinting, MR Fingerprinting, Cardiac MRI, Quantitative MRI, Sequence Design, Contrast Mechanisms
Motivation: Quantification of T1, T2, and T1ρ may provide insight into myocardial fibrosis without the need for gadolinium-based contrast agents.
Goal(s): This study seeks to present and validate a rapid, single breath-hold cMRF approach for simultaneously mapping T1, T2, and T1ρ.
Approach: A cardiac-gated MRF sequence was designed to measure T1, T2, and T1ρ and was tested in simulation, phantom, and six healthy subjects.
Results: The proposed T1/T2/T1ρ cMRF technique yielded accurate high-resolution T1, T2, and T1ρ maps in simulation, phantom, and in vivo.
Impact: Cardiac Magnetic Resonance Fingerprinting can be used to quickly, accurately, and simultaneously map T1, T2, and T1ρ, and has the potential to quickly probe myocardial fibrosis without contrast.
Introduction
T1ρ has recently been suggested as a potential gadolinium-contrast-free marker for myocardial fibrosis1–4. Traditional cardiovascular magnetic resonance (CMR) techniques for mapping T1ρ require the acquisition of multiple T1ρ-weighted images across several breath-holds1,2,5–7, which may lead to errors in the maps. Magnetic Resonance Fingerprinting (MRF) has been used to simultaneously map T1ρ along with other tissue properties in various organs including the heart8–12. This work proposes a 2D cMRF sequence for simultaneous T1, T2, and T1ρ mapping that builds upon prior work by improving spatial resolution in conjunction with a low-rank reconstruction for future application in myocardial fibrosis detection.Methods
Acquisition: Data were acquired using an ECG-triggered 2D cMRF sequence during a single breath-hold, similar to that described previously8, as depicted in Fig. 1. A preparation pulse is followed by a series of 47 excitations and spiral readouts (1.6x1.6x8mm3, FA 4-15°, constant TR/TE 5.4/1ms) during the diastolic period of each heartbeat, for a total acquisition time of 15 heartbeats. Preparation pulses consist of either inversion recovery (IR), spin-lock (SL) at 400Hz, T2 preparation, or no preparation.Reconstruction: T1, T2, and T1ρ maps were generated using a low-rank reconstruction, consisting of an iterative optimization solved using nonlinear conjugate gradient descent which included terms for a truncated SVD compression (rank 5), coil sensitivity maps, NUFFT gridding, and locally low-rank (6x6 patches) and total variation regularization13. MRF subspace images were then matched to the SVD-compressed dictionary which modeled subject-specific heart rate effects. The dictionary consisted of fingerprints for 2,503,006 combinations of T1=10-2000ms, T2=6-1180ms, and T1ρ=6-1180ms for simulation and phantom experiments, and 373,118 combinations of T1=10-2000ms, T2=6-200ms, and T1ρ=6-200ms for in vivo experiments.
Simulations: Data were simulated using the XCAT14 phantom to represent two cases: (Case 1) healthy myocardium with T1=1000ms, T2=44ms, and T1ρ=50ms, and (Case 2) myocardium with a region of fibrosis where fibrotic tissue has T1=1100ms, T2=50ms, and T1ρ=90ms1,2,5,6,9. rRMSE values were computed relative to the ground truth maps.
Phantom Experiments: T1/T2/T1ρ cMRF data was collected from a single slice through the center of the T2 layer of the ISMRM/NIST MRI system phantom15 using a simulated heartbeat of 60 bpm. Conventional T1 (MOLLI)16 and T2 (T2-prepared bSSFP)17 maps were collected using the Siemens Myomaps package. Conventional T1ρ maps were obtained by collecting several T1ρ-weighted images using a T1ρ-prepared FLASH sequence with spin-lock times (TSL) of 0.5, 5, 7, 10, 15, 20, 30, 40, and 60ms. The weighted images were matched to a dictionary of exponential signal curves following $$$M=M_{0}e^{\frac{-TSL}{T_{1\rho}}}$$$ to obtain a T1ρ map. Correlations with reference values obtained using inversion recovery T1, spin-echo T2, and T1ρ map were computed.
In Vivo Experiments: T1/T2/T1ρ cMRF data from a single mid-ventricular short axis slice were acquired in six healthy volunteers at 1.5T (MAGNETOM Sola, Siemens Healthineers). Data were reconstructed using subject specific dictionaries using RR intervals obtained from the ECG signal. Myocardial T1, T2, and T1ρ values were obtained by computing the voxelwise mean and standard deviation from the T1, T2, and T1ρ maps within manually drawn ROIs in the left ventricular septum.
Results
Fig. 2 shows simulated and ground truth T1, T2, and T1ρ maps for both healthy and fibrotic myocardium. The proposed sequence yields accurate T1, T2, and T1ρ estimates for both the cases, with a rRMSE of 2.27%/2.33% for T1, 4.19%/4.27% for T2, and 3.02%/3.59% for T1ρ for cases 1 and 2, respectively. Furthermore, case 2 produces visible and quantifiable detection of fibrotic tissue with a rRMSE in the fibrotic region of 1.26% for T1, 2.07% for T2, and 9.57% for T1ρ.Fig. 3 depicts the T1, T2, and T1ρ maps using both T1/T2/T1ρ cMRF and reference scans. T1, T2, and T1ρ values obtained using cMRF are consistent with the reference values (R=0.99, 0.99, 0.98 respectively).
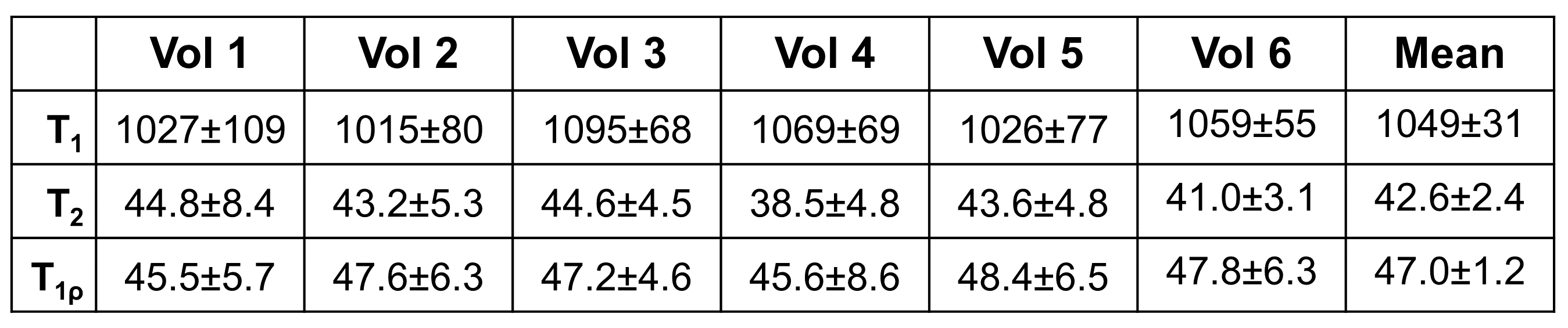
Representative T1, T2, and T1ρ maps obtained from healthy volunteers are shown in Fig. 4. Table 1 shows average T1, T2, and T1ρ values measured in the healthy myocardium. The values are consistent with those previously reported in the literature1,2,5–7,9.
Discussion and Conclusions
This study presents a cMRF technique for simultaneously mapping T1, T2, and T1ρ using a low-rank reconstruction in a single breath-hold. This method improves upon prior work by collecting data at a clinically appropriate spatial resolution and reducing SAR deposited during spin-locking. This technique has potential clinical implications for assessing myocardial fibrosis without gadolinium contrast. Utility in patient cohorts receiving LGE will be investigated in future work.Acknowledgements
This work was supported by the National Institutes of Health/National Heart, Lung, and Blood Institute R01HL153034-04 and R01HL163991-02, and Siemens Healthineers.References
- Witschey WR, Zsido GA, Koomalsingh K, et al. In vivo chronic myocardial infarction characterization by spin locked cardiovascular magnetic resonance. Journal of Cardiovascular Magnetic Resonance. 2012;14(1):37. doi:10.1186/1532-429X-14-37
- Berisha S, Han J, Shahid M, Han Y, Witschey WRT. Measurement of Myocardial T1ρ with a Motion Corrected, Parametric Mapping Sequence in Humans. PLoS One. 2016;11(3):e0151144. doi:10.1371/journal.pone.0151144
- Bustin A, Toupin S, Sridi S, et al. Endogenous assessment of myocardial injury with single-shot model-based non-rigid motion-corrected T1 rho mapping. Journal of Cardiovascular Magnetic Resonance. 2021;23(1):119. doi:10.1186/s12968-021-00781-w
- Bustin A, Witschey WRT, van Heeswijk RB, Cochet H, Stuber M. Magnetic resonance myocardial T1ρ mapping. Journal of Cardiovascular Magnetic Resonance. 2023;25(1):34. doi:10.1186/s12968-023-00940-1
- Wang L, Yuan J, Zhang SJ, et al. Myocardial T1rho mapping of patients with end-stage renal disease and its comparison with T1 mapping and T2 mapping: A feasibility and reproducibility study. Journal of Magnetic Resonance Imaging. 2016;44(3):723-731. doi:10.1002/jmri.25188
- Deng W, Xue Y, Li Y, et al. Normal Values of Magnetic Resonance T1ρ Relaxation Times in the Adult Heart at 1.5 T MRI. Journal of Magnetic Resonance Imaging. 2023;58(2):477-485. doi:10.1002/jmri.28506
- Kamesh Iyer S, Moon B, Hwuang E, et al. Accelerated free-breathing 3D T1ρ cardiovascular magnetic resonance using multicoil compressed sensing. Journal of Cardiovascular Magnetic Resonance. 2019;21(1):5. doi:10.1186/s12968-018-0507-2
- Hamilton JI, Jiang Y, Chen Y, et al. MR fingerprinting for rapid quantification of myocardial T1, T2, and proton spin density - Hamilton - 2017 - Magnetic Resonance in Medicine - Wiley Online Library. Accessed August 28, 2023. https://onlinelibrary.wiley.com/doi/10.1002/mrm.26216
- Velasco C, Cruz G, Lavin B, et al. Simultaneous T1, T2, and T1ρ cardiac magnetic resonance fingerprinting for contrast agent–free myocardial tissue characterization. Magnetic Resonance in Medicine. 2022;87(4):1992-2002. doi:10.1002/mrm.29091
- Sharafi A, Zibetti MVW, Chang G, Cloos M, Regatte RR. MR fingerprinting for rapid simultaneous T1, T2, and T 1 ρ relaxation mapping of the human articular cartilage at 3T. Magn Reson Med. 2020;84(5):2636-2644. doi:10.1002/mrm.28308
- Velasco C, Cruz G, Jaubert O, Lavin B, Botnar RM, Prieto C. Simultaneous comprehensive liver T1, T2, , T1ρ, and fat fraction characterization with MR fingerprinting. Magnetic Resonance in Medicine. 2022;87(4):1980-1991. doi:10.1002/mrm.29089
- Wyatt CR, Barbara TM, Guimaraes AR. T1ρ Magnetic Resonance Fingerprinting. NMR Biomed. 2020;33(5):e4284. doi:10.1002/nbm.4284
- Lima da Cruz G, Bustin A, Jaubert O, Schneider T, Botnar RM, Prieto C. Sparsity and locally low rank regularization for MR fingerprinting. Magnetic Resonance in Medicine. 2019;81(6):3530-3543. doi:10.1002/mrm.27665
- Segars WP, Sturgeon G, Mendonca S, Grimes J, Tsui BMW. 4D XCAT phantom for multimodality imaging research. Med Phys. 2010;37(9):4902-4915. doi:10.1118/1.3480985
- Stupic KF, Ainslie M, Boss MA, et al. A standard system phantom for magnetic resonance imaging. Magnetic Resonance in Medicine. 2021;86(3):1194-1211. doi:10.1002/mrm.28779
- Messroghli DR, Radjenovic A, Kozerke S, Higgins DM, Sivananthan MU, Ridgway JP. Modified Look-Locker inversion recovery (MOLLI) for high-resolution T1 mapping of the heart. Magnetic Resonance in Medicine. 2004;52(1):141-146. doi:10.1002/mrm.20110
- Giri S, Chung YC, Merchant A, et al. T2
quantification for improved detection of myocardial edema. J Cardiovasc Magn
Reson. 2009;11(1):56. doi:10.1186/1532-429X-11-56
Figures