3565
Cluster-Based Low-Rank Regularization for Cardiac Rosette MR Fingerprinting1Radiology, University of Michigan, Ann Arbor, MI, United States, 2Biomedical Engineering, University of Michigan, Ann Arbor, MI, United States
Synopsis
Keywords: MR Fingerprinting, MR Fingerprinting, Sparse & Low-Rank Models, Heart, Quantitative Imaging
Motivation: Breathholds limit the amount of data which can be acquired in cardiac MRF, which can impact the precision of fat/water separated T1, T2, and T2* maps.
Goal(s): We developed a regularization method to reconstruct accurate maps from multi-echo cMRF data without introducing blurring into the resulting tissue property maps.
Approach: A k-means cluster-based approach is used to group the signal evolutions during reconstruction and a low-rank constraint is applied to each cluster. We compared our method to existing approaches in 23 healthy volunteers.
Results: This approach can be used to generate accurate myocardial T1, T2, and T2* maps using rosette MRF data.
Impact: Traditional cardiac MRF reconstructions can fail when working with multi-echo rosette MRF data due to insufficient sampling. We developed a reconstruction method which enables T1, T2, and T2* maps to be collected in a single breathhold without compromising accuracy.
Intoduction
In clinical practice, myocardial T1, T2, and T2* maps are used to assess a variety of conditions, including myocarditis, myocardial edema, and iron deposition1,2. In current practice, a separate breathheld scan is required to collect each of these maps. Previously, MR Fingerprinting3 has been used to estimate T1 and T2 properties in the heart4,5, and recent works have extended MRF to include T2* mapping6. Some MRF reconstruction techniques use locally low-rank models to enhance image quality7. However, in rosette MRF, the image series is also decomposed into images using data collected in each rosette echo8, leading to higher acceleration rates for individual MRF images. This high level of undersampling demands high degrees of regularization in low-rank reconstructions, which can cause blurring in the final maps. We propose a regularization method that clusters voxels with similar signal evolutions, and apply low-rank constraints to each cluster individually. We demonstrate that this cluster-based technique can be used in conjunction with rosette MRF to reconstruct tissue property maps with reduced noise and improved precision.Methods
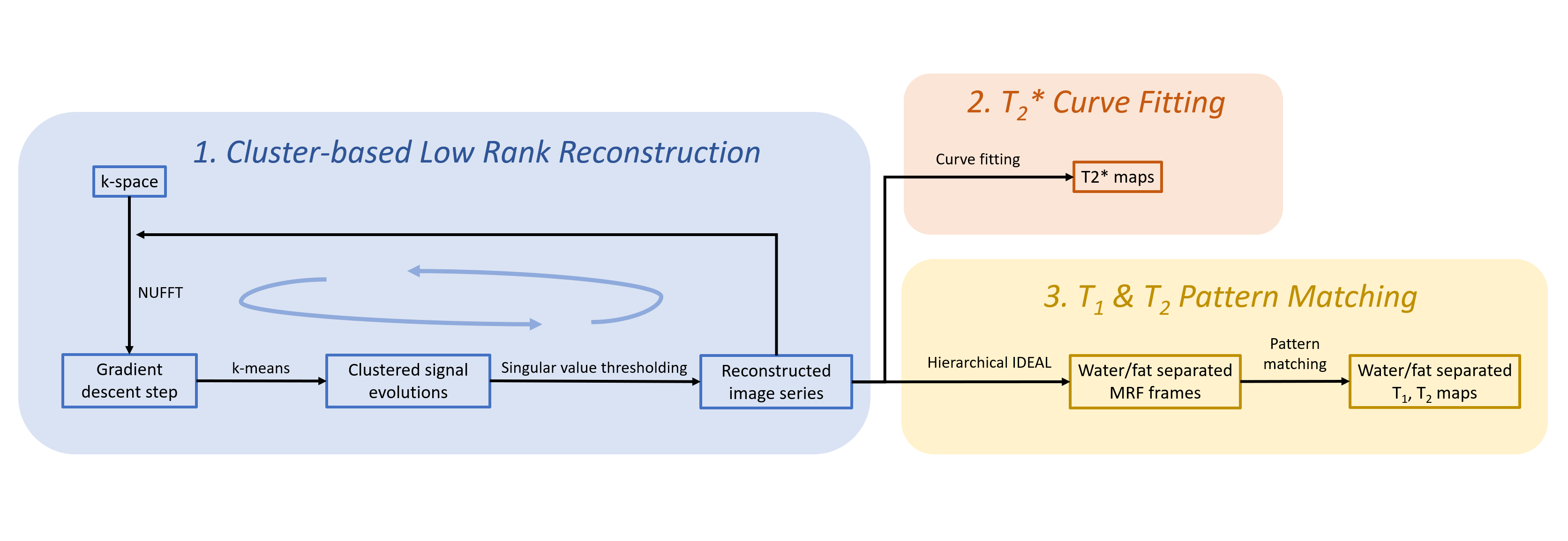
Rosette MRF scans were acquired using a 1.5T Sola scanner (Siemens Healthineers, Erlangen, Germany) using the ISMRM/NIST MRI system phantom and in 23 healthy volunteers. In vivo scans were acquired over 15 heartbeats and were breathheld and ECG-gated. Sequence parameters were: TR=20.4ms, TE1=1.74ms, ΔTE=0.79ms, rosette echo train length=22, FOV=300x300mm2, voxel size=1.56x1.56mm2, 8mm slice thickness, 180 excitations (12 per heartbeat), flip angle range 5.7°-20°. The MRF dictionary was corrected for slice profile and inversion efficiency effects9. Images were reconstructed by solving the following optimization problem using the proximal optimized gradient method10:$$\hat{x}=\mathrm{argmin}\frac{1}{2}||Ex-y||_2^2+\beta\sum_{i=1}^k||C_ix||_*$$
Where E represents the encoding matrix, including the NUFFT11, coil sensitivity encoding, SVD compression12, and B0 correction13 operations. x represents the image series, and y represents the acquired k-space data. At each iteration, k-means clustering is performed to group similar fingerprints; Ci represents the operation to select voxels within the ith cluster.
The reconstructed image series is then used to estimate the tissue property maps. First, T2* maps are calculated using a curve-fitting algorithm14. Next, Hierarchical IDEAL is used to generate fat/water separated MRF images13, which are used in a pattern matching step to estimate T1 and T2 maps. Reference values for the ISMRM/NIST phantom were acquired using inversion recovery T1, spin-echo T2, and GRE T2* sequences. Reference scans were collected in each volunteer using Siemens Myomaps (MOLLI15 T1, T2-prep bSSFP T216, and GRE T2*). A Bland-Altman analysis was used to compare myocardial values for the study population.
Results and Discussion
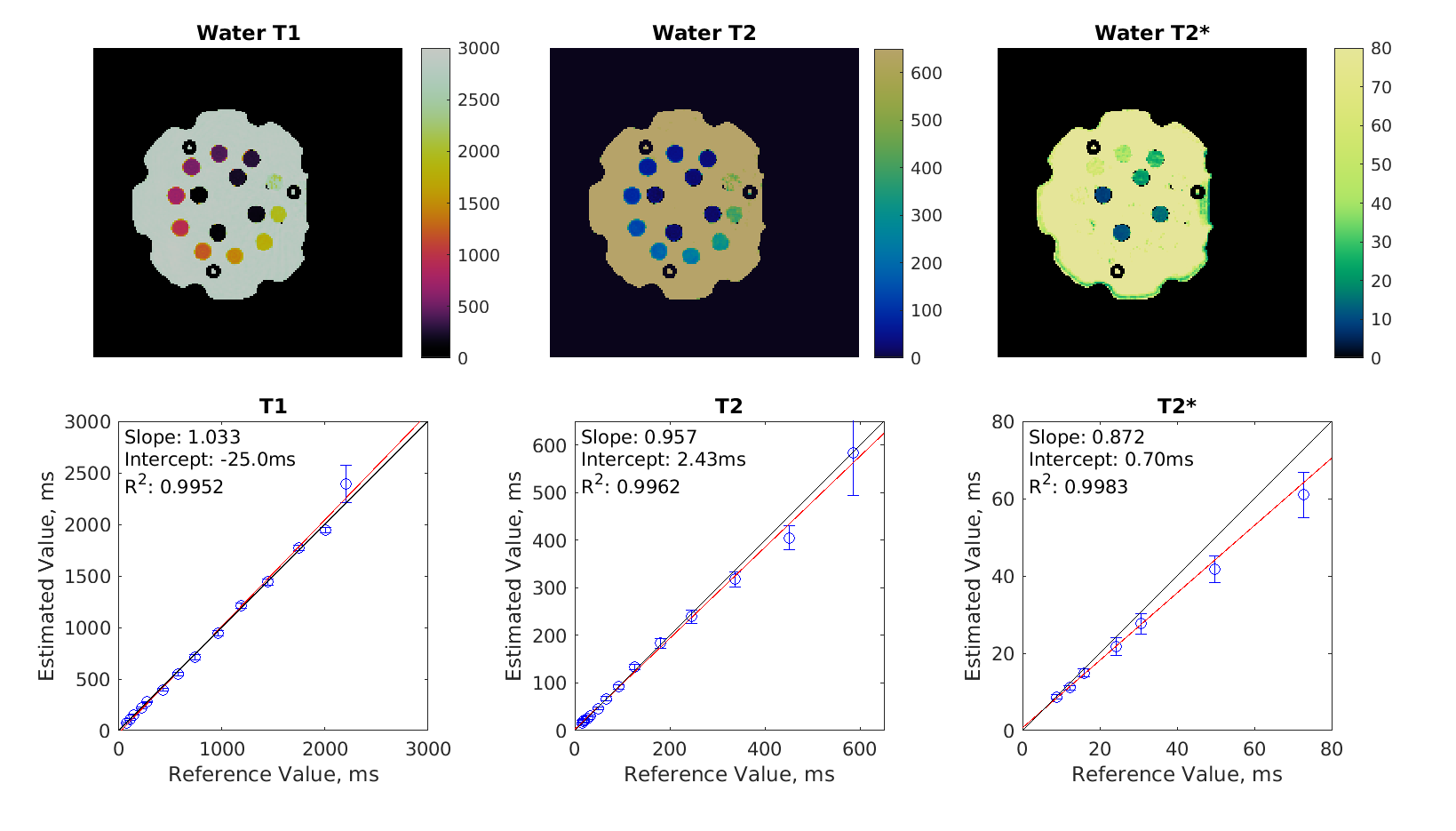
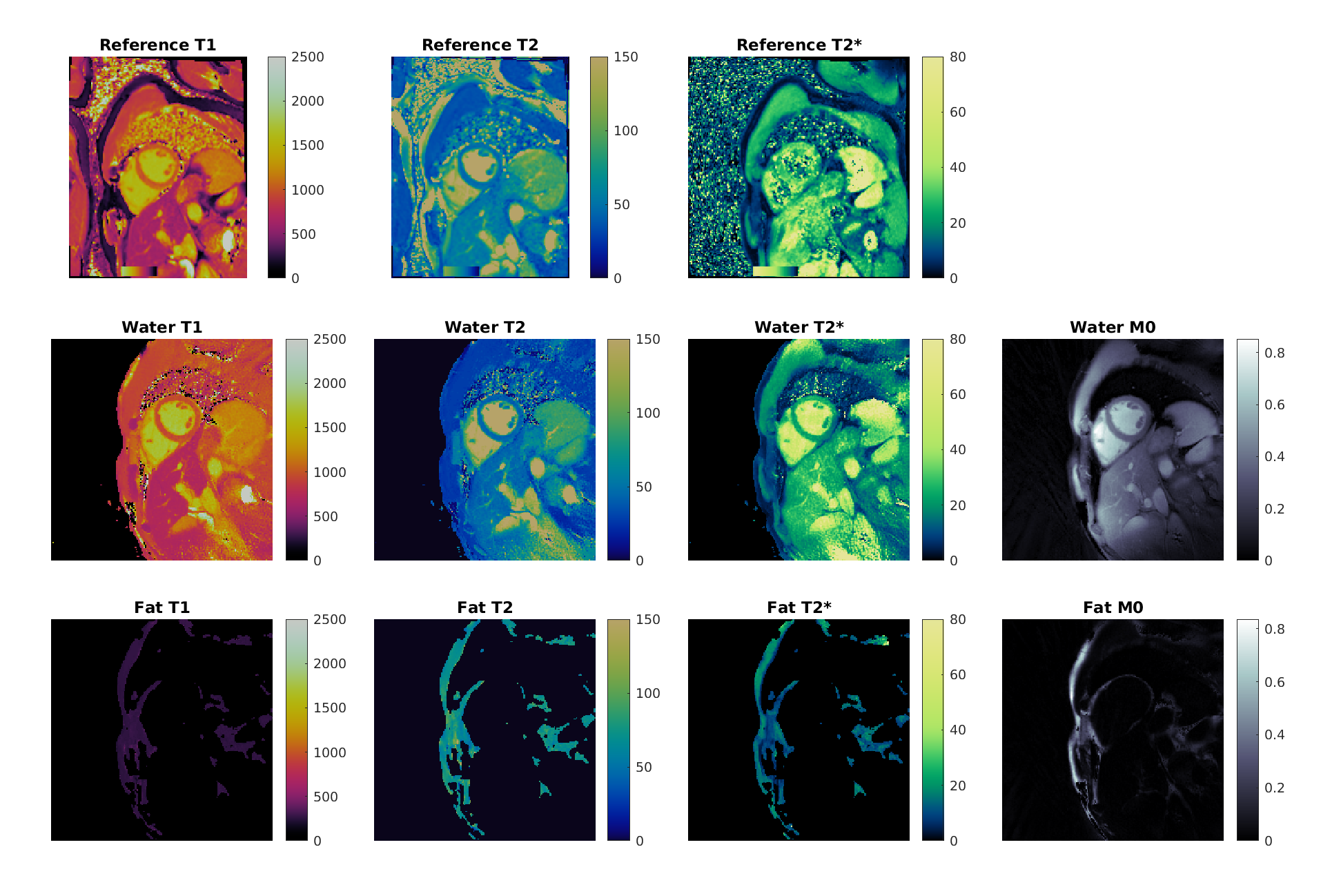
Figure 2 shows regressions between rosette MRF and standard measurements in the ISMRM/NIST phantom. T1 and T2 show good agreement with regression slopes of 1.033 and 0.957, respectively; T2* shows lower agreement with a regression slope of 0.872 due to an underestimation by rosette MRF at high T2* values.Maps from a healthy subject are shown in Figure 3. Using the proposed reconstruction, we report average myocardial values for the healthy subjects of T1=1071±50ms, T2=46.6±2.9ms, T2*=24.6±4.8ms. Reference scans in the same subjects had values of T1=1017±26ms, T2=48.3±1.6ms, T2*=30.9±3.8ms.
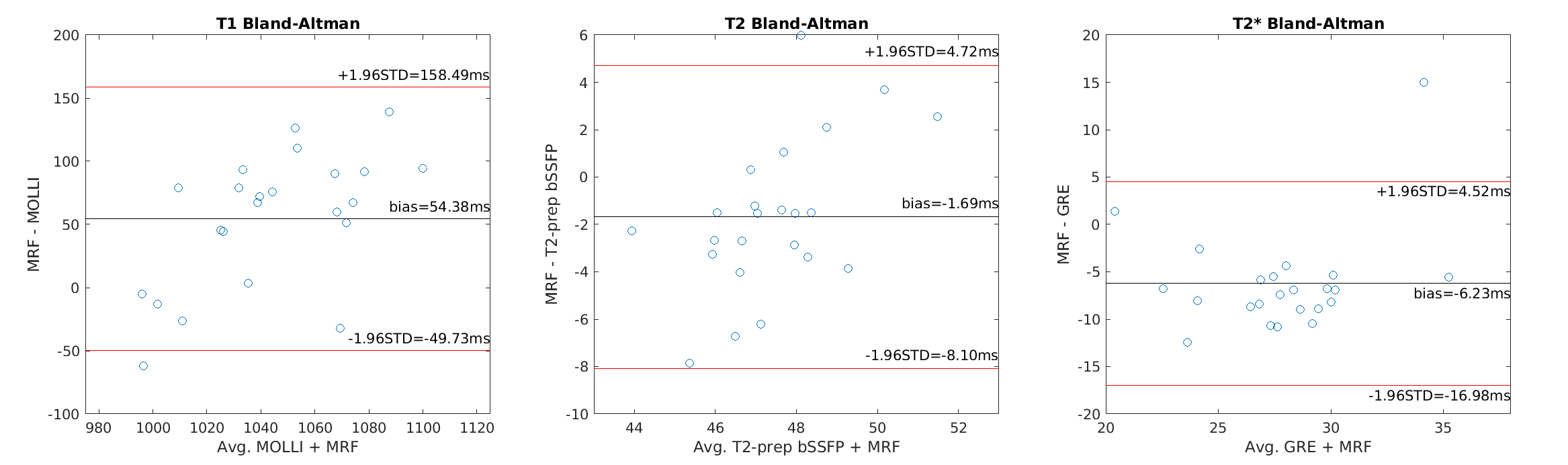
Figure 4 shows the results of Bland-Altman analysis of myocardial values for the entire study population. For T1, the bias of measured MRF values with respect to MOLLI is 54ms, and the 95% confidence interval (CI) is ±104ms. This bias is within bounds previously reported in literature9,17. For T2, the bias of MRF with respect to T2-prep bSSFP is -1.7ms, and the 95%CI is ±6.4ms. For T2*, the bias of MRF with respect to GRE mapping is -6.2ms, and the 95%CI is ±10.8ms. One potential explanation for this disagreement is that in vivo GRE measurements are plagued with artifacts (as seen in Figure 3). Moreover, this implementation of rosette MRF may be less sensitive to T2* values above 20 ms as seen in the phantom study.
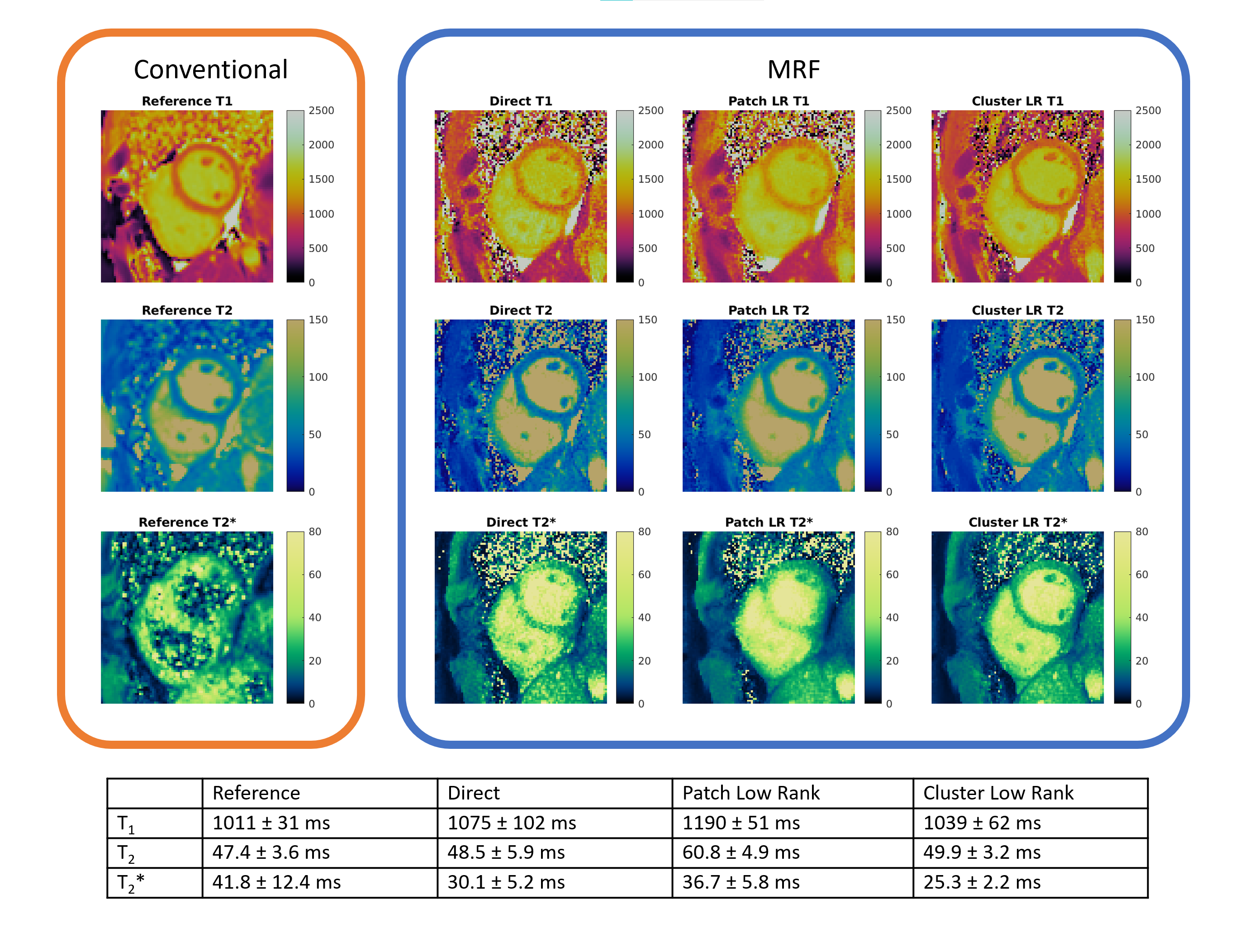
Figure 5 shows a comparison between the direct4, patch-based8, and the proposed cluster-based reconstruction. Compared to the direct reconstruction in a septal ROI, the patch-based reconstruction reduces the standard deviation in T1 and T2, but overestimates both properties due to blurring. In the cluster-based reconstruction, the standard deviation of T1 and T2 are reduced, but the mean values are similar to those obtained with a direct reconstruction. Note that while the T2* values vary between the reconstructions, the cluster-based reconstruction exhibits the lowest noise level.
Conclusion
We introduce a novel cluster-based regularization approach to reconstruct multi-echo rosette MRF data with improved precision compared to previous reconstruction techniques. This approach can be used to generate accurate myocardial water and fat T1, T2, and T2* maps using rosette MRF data.Acknowledgements
NIH NHLBI R01HL153034-04
NIH NHLBI R01HL163991-02
Siemens Healthineers
References
1. Messroghli DR, Moon JC, Ferreira VM, et al. Clinical Recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2*, and extracellular volume. J Cardiovasc Magn Reson 2017; 19(1):75
2. Tridyaska P, Oudkerk M, Sijens PE. Cardiac T2* mapping: Techniques and clinical applications. JMRI 2020; 52(5):1340-1351
3. Ma D, Gulani V, Seiberlich N, et al. Magnetic Resonance Fingerprinting. Nature 2013; 495:187-192
4. Hamilton JI, Jiang Y, Chen Y, et al. MR Fingerprinting for Rapid Quantification of Myocardial T1, T2 and Proton Spin Density. Magn Reson Med 2017; 77:1446-1458
5. Liu Y, Hamilton J, Eck B, et al. Myocardial T1 and T2 quantification and water-fat separation using cardiac MR fingerprinting with rosette trajectories at 3T and 1.5T. Magn Reson Med 2021; 85:103-119
6. Cruz GJL, Velasco C, Lavin B, et al. Myocardial T1, T2, T2*, and fat fraction quantification via low-rank motion-corrected cardiac MR fingerprinting. Magn Reson Med 2022; 87(6):2757-2774
7. Hamilton JI, Jiang Y, Ma D, et al. Simultaneous multislice cardiac magnetic resonance fingerprinting using low rank reconstruction. NMR Biomed 2019; 32(2):e4041
8. Bush AM, Sandino CM, Ramachandran S, et al. Rosette Trajectories Enable Ungated, Motion-Robust, Simultaneous Cardiac and Liver T2* Iron Assessment. JMRI 2020; 52(6):1688-1698
9. Hamilton JI, Jiang Y, Ma D, e al. Investigating and reducing the effects of confounding factors for robust T1 and T2 mapping with cardiac MR fingerprinting. Magn Reson Imaging 2018; 53:40-51
10. Kim D, Fessler JA. Optimized first-order methods for smooth convex minimization. Mathematical Programming 2016; 159(1):81-107
11. Fessler JA, Sutton BP. Nonuniform fast Fourier transforms using min-max interpolation. IEEE Trans Signal Processing 2003; 51:560-574
12. McGivney DF, Pierre E, Ma D, et al. SVD Compression for Magnetic Resonance Fingerprinting in the Time Domain. IEEE Trans Med Imaging 2014; 33(12):2311-2322
13. Tsao J, Jiang Y. Hierarchical IDEAL: fast, robust, and multiresolution separation of multiple chemical speces from multiple echo times. Magn Reson Med 2013; 70(1):155-159
14. Chebrolu VV, Hines CDG, Yu H, et al. Independent estimation of T2* for Water and Fat for Improved Accuracy of Fat Quantification Magn Reson Med 2010; 62(4):849-857
15. Messroghli DR, Radjenovic A, Kozerke S, et al. Modified Look-Locker Inversion Recovery (MOLLI) for High-Resolution T1 mapping of the Heart. Magn Reson Med 2004; 52:141-146
16. Giri S, Chung Y, Merchant A, et al. T2 quantification for improved detection of myocardial edema. J Cardiovasc Magn Reson 2009; 11(1):56
17. Liu Y, Hamilton J, Rajagopolan S, Seiberlich N. Cardiac Magnetic Resonance Fingerprinting: Technical Overview and Initial Results. JACC Cardiovascular Imaging 2018; 11(12):1837-53
Figures