3541
Native T1 Mapping Radiomics for Classification of Pulmonary Valve Replacement Risk Factors in Patients with Repaired Tetralogy of Fallot1Department of Biomedical Engineering and Environmental Sciences, National Tsing Hua University, Hsinchu, Taiwan, 2Department of Radiology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 3Department of Electrical Engineering, National Taiwan University of Science and Technology, Taipei, Taiwan, 4Department of Automatic Control Engineering, Feng Chia University, Taichung, Taiwan, 5Department of Pediatrics, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 6Dpartment of Pediatrics, National Yang Ming Chiao Tung University, Hsinchu, Taiwan
Synopsis
Keywords: Myocardium, Radiomics
Motivation: Right ventricular (RV) dilation and exercise intolerance are important prognostic indicators in repaired Tetralogy of Fallot (rTOF) patients. The conventional native T1 value may ignore subtle changes of myocardial fibrosis patterns in rTOF patients. Radiomics uncovers concealed insights regarding cardiomyopathy.
Goal(s): To establish a radiomics model using native T1 mapping for identifying rTOF patients with severe RV dilation and exercise intolerance.
Approach: We extracted 623 radiomic features from native T1 mapping and employed machine learning for feature selection and classification that enhance diagnostic accuracy in identifying cardiac involvements.
Results: Optimal performance was achieved in the segmental mid-slice T1 mapping model.
Impact: The radiomic analysis of myocardial native T1 can reveal the different myocardial T1 distribution patterns between different severity of RV dilation and exercise intolerance before substantial changes of conventional native T1 values.
Introduction
Patients with surgical repair of tetralogy of Fallot (rTOF) often face reduced exercise capacity [1] and pulmonary regurgitation (PR), which has been associated with right ventricular (RV) dilation and dysfunction [2]. A previous study demonstrated that preoperative oxygen uptake in rTOF patients undergoing pulmonary valve replacement (PVR) can early postoperative mortality [3].Conventional visualization of CMR images and averaging native T1 may ignore subtle changes of myocardial fibrosis patterns in rTOF patients. Radiomics was reported to demonstrate disease-specific quantitative features in several cardiovascular diseases [4].This study aimed to develop a radiomics-based classification model by native T1 mapping to identify patients with severe RV dilation and exercise intolerance.
Methods
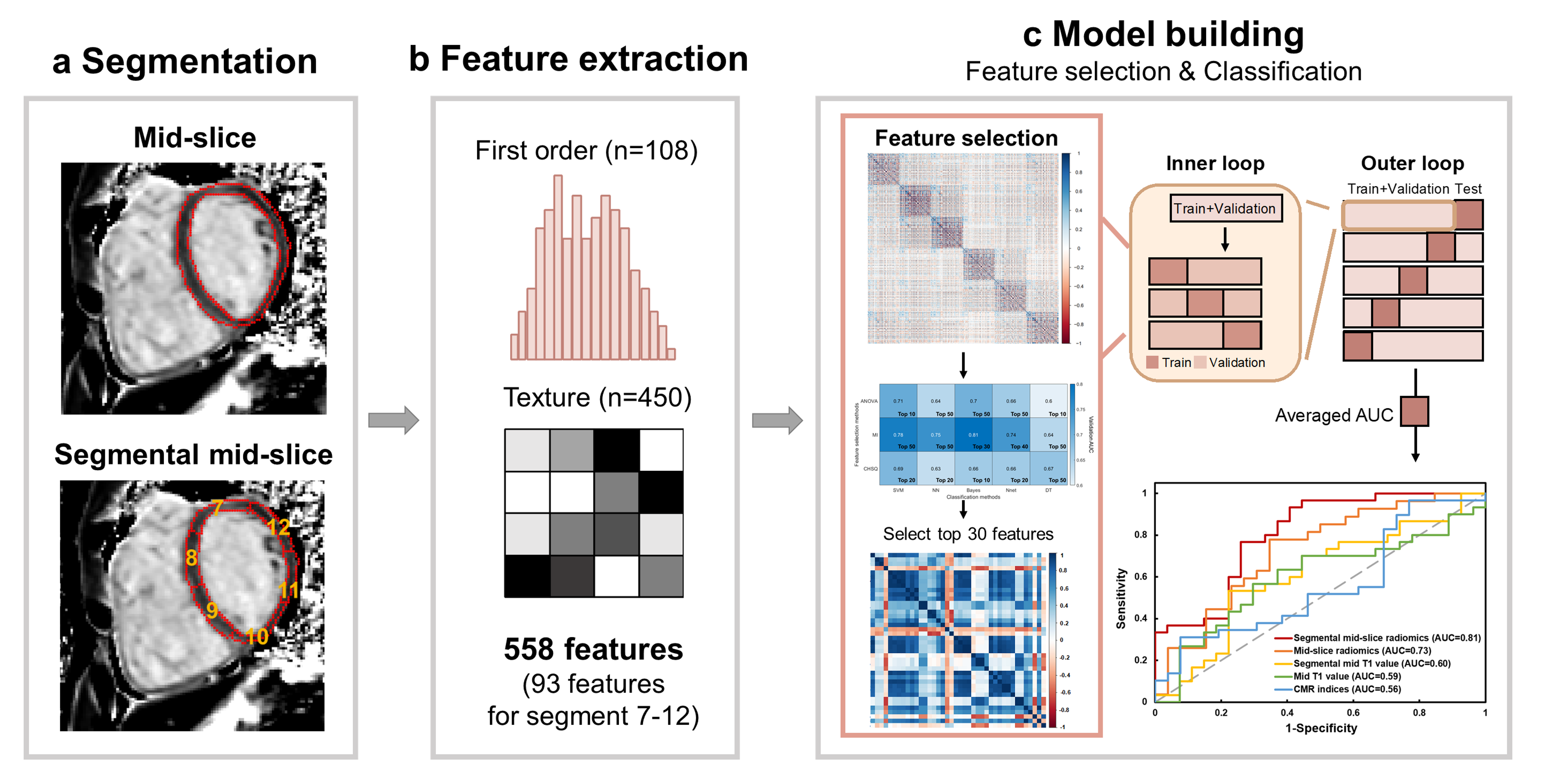
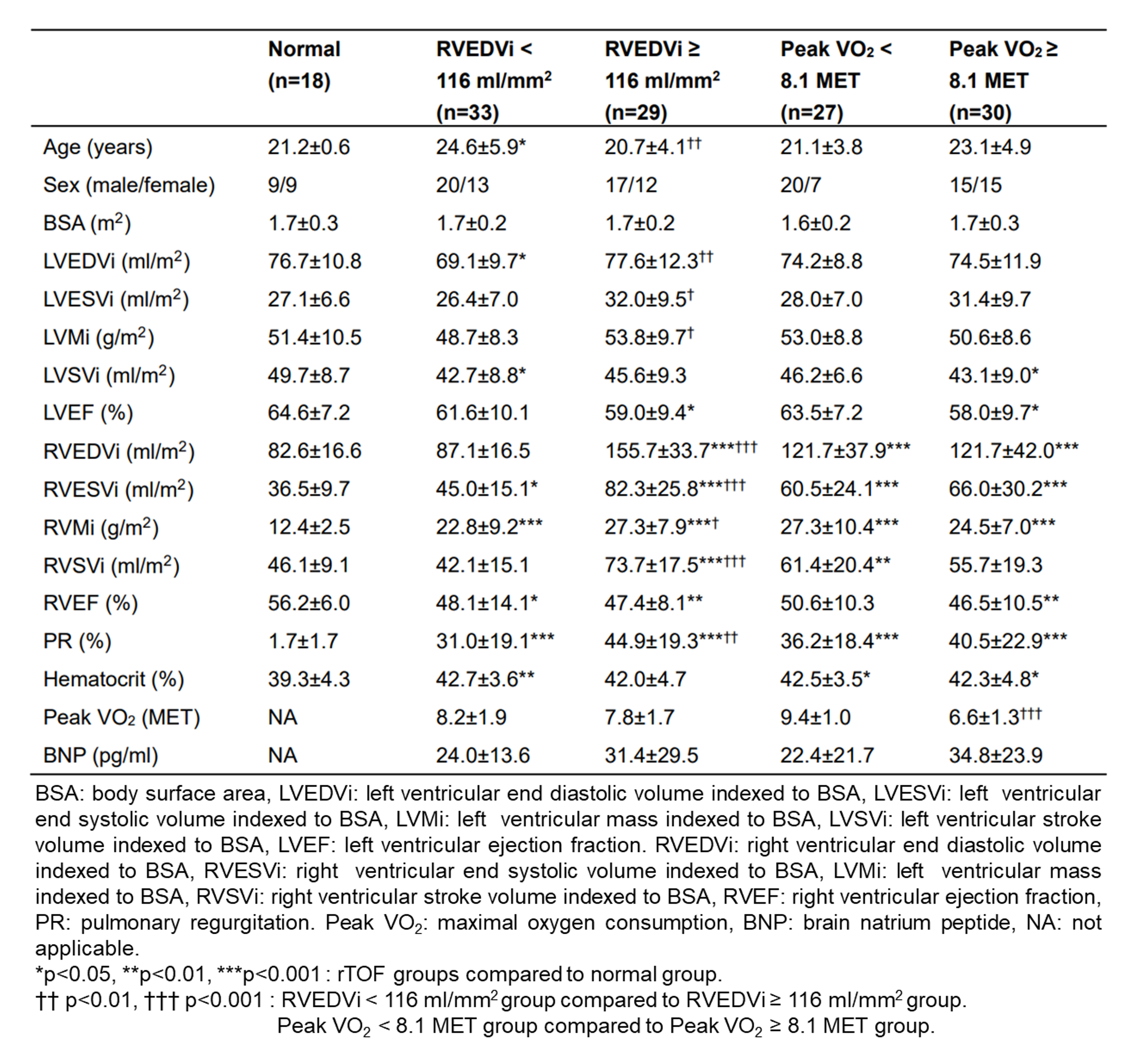
In this study, one of the two radiomic classification task was to distinguish rTOF patients with RVEDVi≥116 ml/mm2 (n=29) from those with RVEDVi<116 ml/mm2 (n=33). The other radiomic classification task was to discriminate rTOF patients with peak VO2<8.1 MET (n=30) from those with peak VO2≥8.1 MET (n=27). CMR images were acquired in a 3T scanner (Skyra, Siemens). A single-breath-hold ECG-gated Modified Look-Locker inversion recovery (MOLLI) sequence was acquired in diastole, with scanning parameters of TR/TE=2.57/1.2 ms, flip angle=35∘, and voxel size=1.1×1.1×8 mm3. The manually delineated regions of interest (ROIs) of LV myocardium on the mid-slice were divided into 6 segments.Figure 1 illustrates the radiomics workflow. Pyradiomics (version 3.0.1) [5] was used to extract 89 radiomic features from the whole mid-slice and 623 features from segment 7-12 of mid-slice.
We employed different feature selection methods and classification models to achieve the best classification performance in different tasks. In the classifying RV dilation task, we employed mutual information (MI) to extract the top 30 features in the mid-slice model and ANOVA to extract the top 10 features in the segmental mid-slice model. The support vector machine (SVM) was used as classification method in this task. In classifying exercise intolerance task, we used ANOVA to extract the top 5 features in the mid-slice model and MI to select the top 30 features in the segmental mid-slice model. SVM and Bayes methods were used as classification methods in the mid-slice and segmental mid-slice model, respectively. A p-value<0.05 was considered statistically significant.
Results
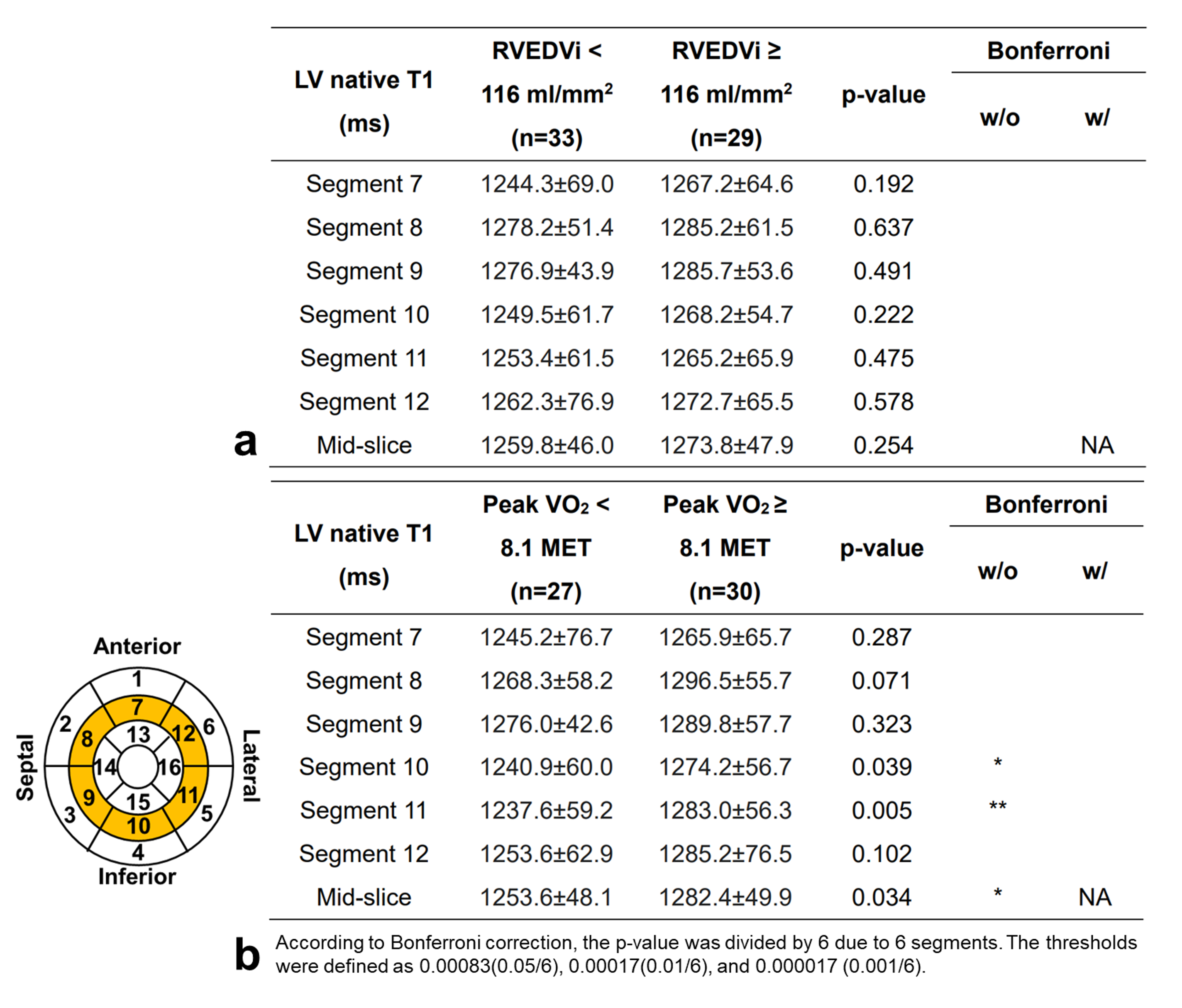
Table 1 summarizes the demographics and cardiovascular characteristics of rTOF patients. The RVEDVi≥116 group exhibited higher RVEDVi, RVESVi, RVMi, RVSVi, and PR (all p<0.05) than the RVEDVi<116 group. There was no significant difference between peak VO2≥8.1 and peak VO2<8.1 groups.In Figure 2a, the native T1 values of segment 7-12 and the whole mid-slice presented no significant difference between RVEDVi<116 and RVEDVi≥116 groups. Without Bonferroni correction, the peak VO2≥8.1 group exhibited significantly increased native T1 in segment 10, 11, and mid-slice (all p<0.05) compared to the peak VO2<8.1 group. However, there is no significant difference between the two groups in segment 7-12 after Bonferroni correction (Figure 2b).
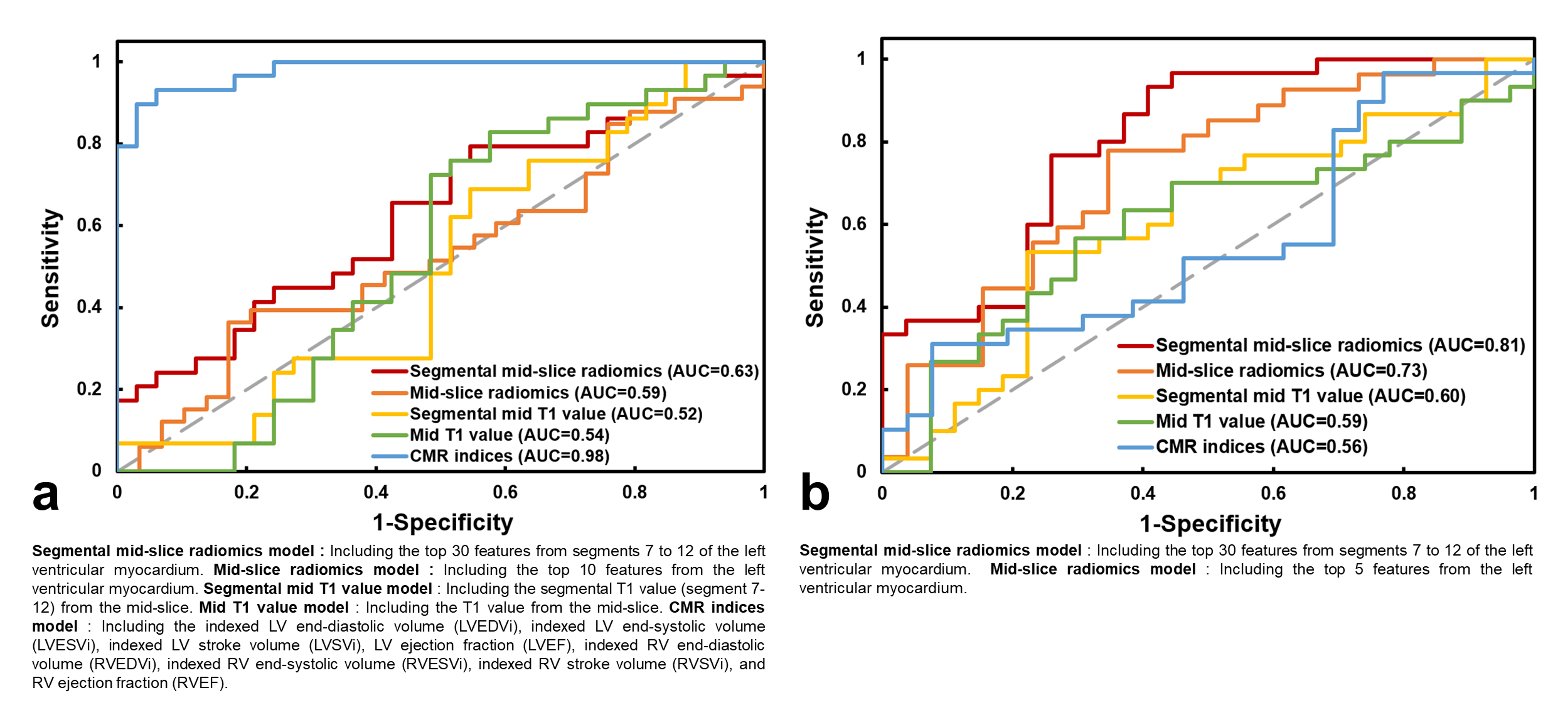
In Figure 3a, the area under curve (AUC) in classifying RVEDVi by segmental mid-slice radiomics model was 0.63 which was higher than the other four models (AUC=0.52-0.59). The AUC exercise intolerance by segmental mid-slice radiomics model was 0.81 which was higher than the other four models (AUC=0.56-0.73) (Figure 3b).
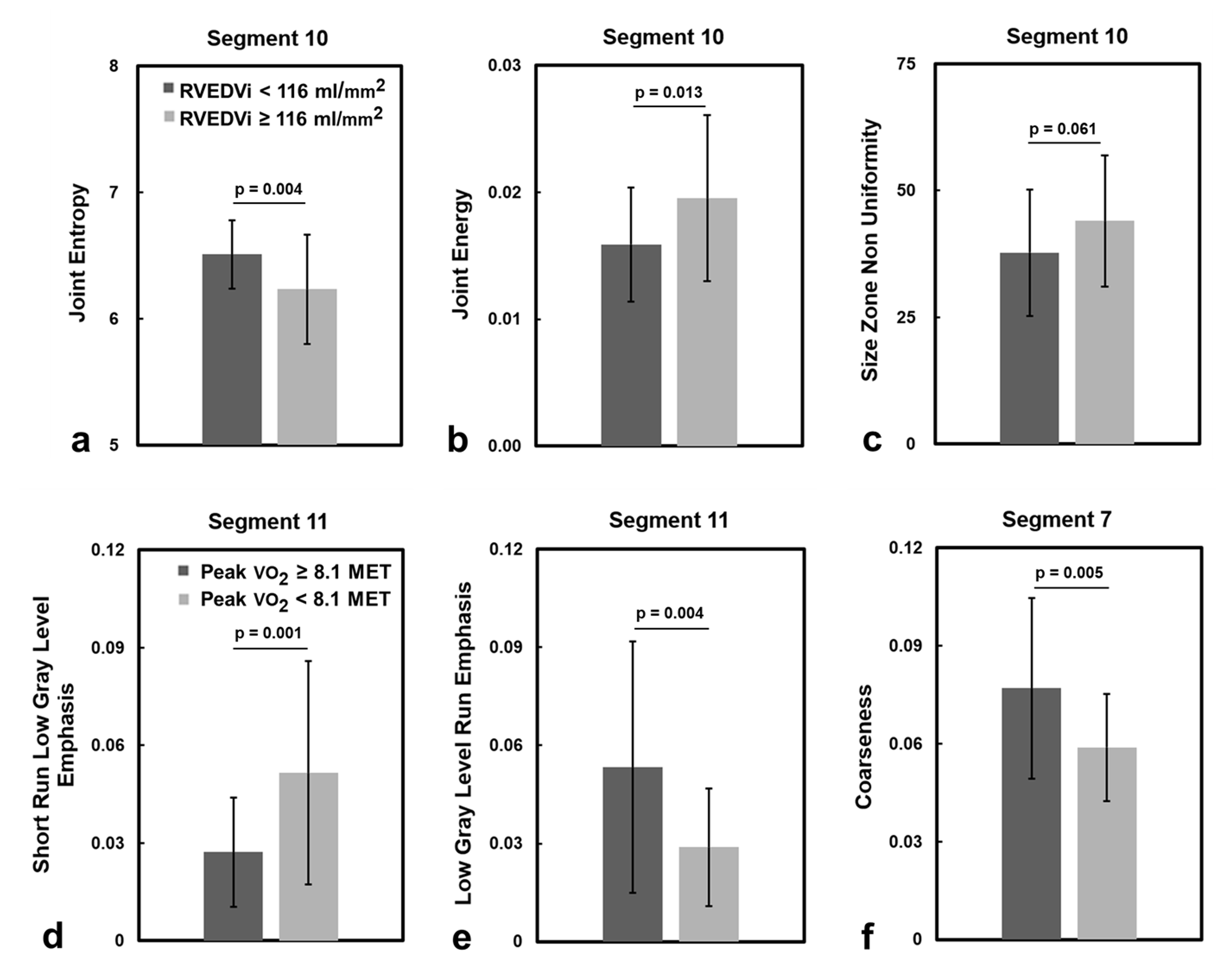
Compared to the RVEDVi<116 group, the RVEDVi≥116 group presented lower joint entropy, higher joint energy and size zone non-uniformity (all p<0.05) in segment 10. Compared to the peak VO2≥8.1 group, the peak VO2<8.1 group presented higher short run low gray level emphasis and lower low gray level run emphasis in segment 11 and lower coarseness in segment 7 (all p<0.01).
Discussion and Conclusion
Compared to conventional native T1 values, the proposed segmental mid-slice native T1 radiomics-based classification model demonstrated high AUC in classifying patients with severe RV dilation and exercise intolerance.In the classifying RV dilation task, the selected top 3 features unveiled a greater degree of heterogeneous myocardial tissue in RVEDVi≥116 group. In the classifying exercise intolerance task, the selected top 3 features demonstrated more intricate textural details and a less uniform texture of myocardial fibrosis in the peak VO2<8.1 group. A previous study suggested an association between elevated markers of diffuse fibrosis and myocardial dysfunction, RV dilation and exercise intolerance in rTOF patients [6]. Our study similarly identified a comparable phenomenon through native T1 radiomics. The prominent features might reveal an inherent correlation with tissue-level alterations associated with increased RV volume and decreased exercise tolerance.
In conclusion, the radiomic analysis of myocardial native T1 can reveal the different myocardial T1 distribution patterns between different severity of RV dilation and exercise intolerance before substantial changes of conventional native T1 values.
Acknowledgements
No acknowledgement found.References
[1] Fredriksen, P.M., et al. Aerobic capacity in adults with tetralogy of Fallot. Cardiol Young. 2002.
[2] Redington AN, et al. Determinants and Assessment of Pulmonary Regurgitation in Tetralogy of Fallot: Practice and Pitfalls. Cardiol Clin. 2006.
[3] Babu-Narayan, S.V., et al. Clinical outcomes of surgical pulmonary valve replacement after repair of tetralogy of Fallot and potential prognostic value of preoperative cardiopulmonary exercise testing. Circulation. 2014.
[4] Gillies, R. J., et al. Radiomics: Images Are More than Pictures, They Are Data. Radiology. 2016.
[5] van Griethuysen JJM, et al. Computational radiomics system to decode the radiographic phenotype. Cancer Res. 2017.
[6] Riesenkampff, E., et al. Increased left ventricular myocardial extracellular volume is associated with longer cardiopulmonary bypass times, biventricular enlargement and reduced exercise tolerance in children after repair of Tetralogy of Fallot. J Cardiovasc Magn Reason. 2016.
Figures