3538
Comparing 3D Cardiovascular MR Angiography with 3D bSSFP Whole Heart Imaging in Congenital Heart Diseases: A REACT Study1Pediatric Cardiology, University of Texas South Western, Dallas, TX, United States
Synopsis
Keywords: Vascular, Cardiovascular, Congenital Heart Disease (CHD)
Motivation: 3-Dimensional Whole Heart balanced Steady-State-Free-Precession (3D bSSFP) MR imaging is reliable for congenital heart disease (CHD) assessment, but field inhomogeneity-induced banding artifacts limit its utility.
Goal(s): This study assesses a 3D Whole Heart approach utilizing a modified REACT technology to enhance image quality for cardiac cardiovascular anatomy compared to conventional 3D bSSFP imaging.
Approach: Eleven patients were compared for image quality, vessel diameters and contrast-to-noise ratios.
Results: Modified REACT improves cardiovascular imaging in CHD particularly of the pulmonary veins and the aorta compared to traditional 3D bSSFP imaging
Impact: Visualizing cardiovascular structures like pulmonary veins in CHD patients can be challenging due to off-resonance effects. A modified REACT sequence with triggering overcomes these imaging difficulties providing improved image quality compared to 3D bSSFP.
Background
The EKG-triggered and respiratory navigator-gated 3D bSSFP cardiac magnetic resonance imaging enables complete evaluation of the cardiovascular anatomy in patients with CHD. Nonetheless, its vulnerability to off-resonance effects can lead to a decline in image quality, particularly when dealing with extensive fields of view or high magnetic field strengths [1]. To address this limitation, different techniques were developed including an interleaved T2 preparation-inversion recovery method described by Ginami et al. [2] A variation of this, REACT shows great promise in obtaining high-quality angiograms without the need for respiratory or cardiac gating within a reasonable timeframe. As a three-dimensional, non-contrast-enhanced cardiac MRA method, it is independent of flow dynamics [3]. This technique delivers high-quality images and an equivalent level of diagnostic confidence compared to high-resolution contrast-enhanced steady-state CMRA in a challenging cohort of young children with complex CHD [4]. It also enables reliable imaging of entire thoracic vasculature in the same cohort [5]. This study aims to evaluate cardiac structures and great vessels using a 3D whole heart approach exploiting REACT technology with respiratory gating and EKG triggering compared to the conventional 3D bSSFP whole heart imaging in pediatric patients with CHD.Method
All scans were performed on a clinical whole body 1.5 T CMR system (Ingenia Philips Healthcare, Best, Netherlands). The protocol included a modified REACT sequence and a standard 3D SSFP sequence. For the REACT sequence, a T2-prepulse and IR prepulse were combined with a mDIXON technique. REACT imaging was based on a modified approach which includes EKG triggering in mid-diastole and respiratory navigator gating which were added to the original REACT sequence. The 3D single-phase SSFP sequence is respiratory-gated and ECG-triggered at the end of diastole with a SPIR fat saturation prepulse to null fat and a T2 prepulse to improve the myocardium to blood pool tissue contrast. Eleven (6 male and 5 female, mean age:15.1 range 7-21) children with CHD who underwent both 3D single phase whole heart imaging and mREACT-CMRA were retrospectively identified. Cardiac structures and great vessels were analyzed for contrast-to-noise ratio and image quality. First, two experienced pediatric cardiologists assessed image quality visually independently according to the five-point system [6], and then consensus grades were given. Aortic arch, right ventricular outflow tract, and pulmonary arteries cross-sectional measurements were taken and compared between two MR imaging sequences. Categorical data were compared by using the Wilcoxon test and normally distributed variables were compared by using a t-test.Results
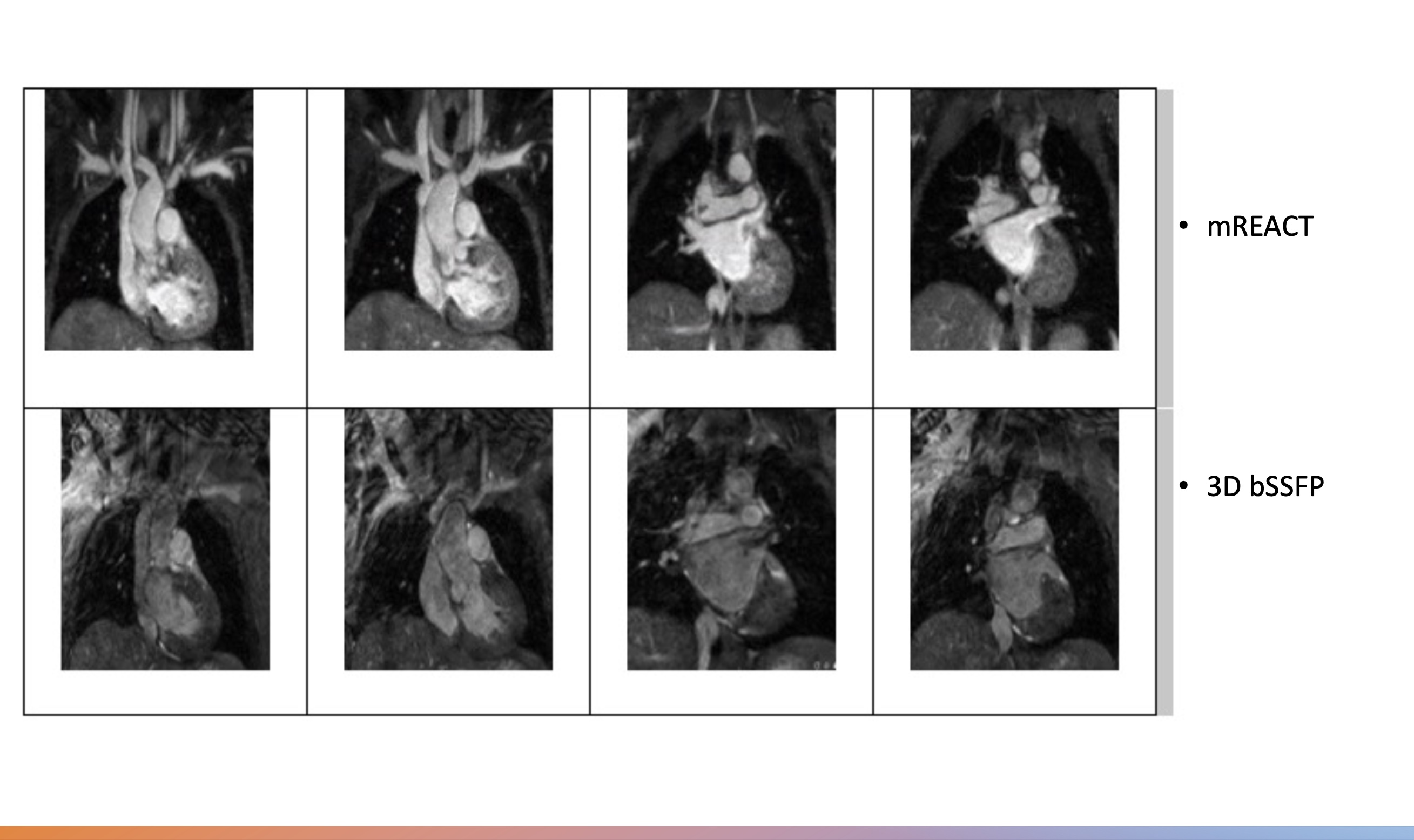
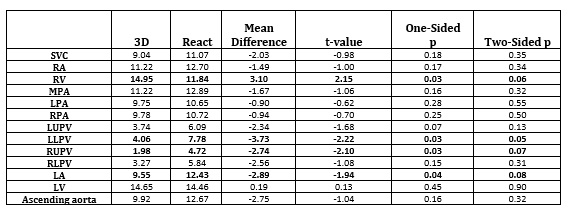
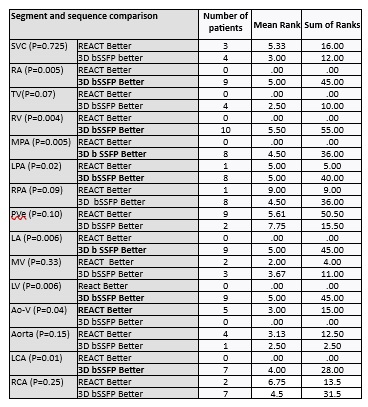
Mean CNR ratios differed significantly between the REACT sequence and the 3D bSSFP Whole heart for various cardiac structures. Specifically, the REACT sequence exhibited higher CNR ratios in the right upper pulmonary vein (4.7 vs. 1.9), left lower pulmonary vein (7.8 vs. 4.1), and left atrium (11.4 vs. 9.3), all with p<0.05. In contrast, the 3D whole heart pulse sequence showed significantly greater CNR in the right ventricle (14.9 vs. 11.8, p=0.03). (Table 1) When it came to image quality, the image quality of 3D whole heart imaging was better at the right atrium (total rank, 45 vs 0 p=0.00), right ventricle (total rank 55 vs 0, p=0.00), main pulmonary artery (total rank 36 vs 0 p=0.00), left pulmonary artery (total rank 40 vs 5 p=0.02), left atrium (total rank 45 vs 0, p=0.00), left coronary artery (total rank 28 vs 0, p=0.01). Whereas, the REACT sequence demonstrated superior image quality compared to 3D WH for the aortic valve (15 vs 0, p=0.04). REACT sequence was also better than the 3D WH pulse sequence at pulmonary veins (50.5 vs 15.5, p=0.10) and ascending aorta (12.5 vs 2.5, p=0.15) but these were not statistically significant.(Figure 1 and Table 2)Importantly, all cross-sectional measurements remained similar between the two sequences.
Conclusion
In this study involving patients with CHD, a 3D Whole Heart approach incorporating REACT technology, enhanced with EKG triggering and respiratory navigator gating, delivered high image quality for the aortic valve, ascending aorta, and pulmonary veins. Additionally, it yielded precise cross-sectional measurements for vascular structures compared to standard 3D bSSFP CMRA.Acknowledgements
No acknowledgement found.References
1. Çukur T, Lee JH, Bangerter NK, Hargreaves BA, Nishimura DG. Non-contrast-enhanced flow-independent peripheral MR angiography with balanced SSFP. Magn Reson Med. 2009;61(6):1533-1539. doi:10.1002/mrm.21921
2. Milotta G, Ginami G, Cruz G, Neji R, Prieto C, Botnar RM. Simultaneous 3D whole-heart bright-blood and black blood imaging for cardiovascular anatomy and wall assessment with interleaved T2prep-IR. Magn Reson Med. 2019;82(1):312-325. doi:10.1002/mrm.27734
3. Yoneyama M, Zhang S, Hu HH, et al. Free-breathing non-contrast-enhanced flow-independent MR angiography using magnetization-prepared 3D non-balanced dual-echo Dixon method: A feasibility study at 3 Tesla. Magn Reson Imaging. 2019;63:137-146. doi:10.1016/j.mri.2019.08.017
4. Isaak A, Mesropyan N, Hart C, et al. Non-contrast free-breathing 3D cardiovascular magnetic resonance angiography using REACT (relaxation-enhanced angiography without contrast) compared to contrast-enhanced steady-state magnetic resonance angiography in complex pediatric congenital heart disease at 3T. Journal of Cardiovascular Magnetic Resonance. 2022;24(1). doi:10.1186/s12968-022-00895-9
5. Isaak A, Luetkens JA, Faron A, et al. Free-breathing non-contrast flow-independent cardiovascular magnetic resonance angiography using cardiac gated, magnetization-prepared 3D Dixon method: assessment of thoracic vasculature in congenital heart disease. Journal of Cardiovascular Magnetic Resonance. 2021;23(1). doi:10.1186/s12968-021-00788-3
6. Mcconnell M V, Khasgiwala VC, Savor& BJ, et al. Comparison of Respiratory Suppression Methods and Navigator Locations for MR Coronary Angiography.; 1997. www.ajronline.org
Figures