3537
Pressure gradient before and after transcatheter pulmonary valve implantation for repaired tetralogy of Fallot: a new 4D flow MRI measurement1Tokyo Women's Medical University, Tokyo, Japan, 2Philips Japan, Tokyo, Japan
Synopsis
Keywords: Flow, Cardiovascular
Motivation: Estimating pressure gradients due to valvular disease using 4D flow MRI in repaired TOF
Goal(s): Identify the location and extent of the pressure gradient
Approach: new 4D flow MRI software for pressure gradient measurement
Results: In right heart catheter-defined pulmonary hypertension, this software showed a right ventricular outflow tract to pulmonary artery pressure gradient.
Impact: Whereas pressure gradients used to require invasive catheterization, our method is a noninvasive test that does not use contrast media. It also has the advantage of being able to locate the site of the pressure gradient.
Introduction
Tetralogy of Fallot (TOF) repair was once considered a curative procedure, but studies of long-term outcomes show that many patients develop sequelae 20 to 30 years after surgery, with about half requiring reoperation. Until recently, open chest surgery was the only treatment option, but recently a minimally invasive transcatheter pulmonary valve implantation (TPVI) procedure has been developed that is less invasive and results in shorter hospital stays1). TPVI is gaining popularity as a minimally invasive treatment, its indication must be carefully determined in cases of right ventricle (RV) pressure overload. Detection of pulmonary hypertension (PH) is necessary pre-treatment information, and is also important to monitor after TPVI. In this study, a new software dedicated to 4D flow MRI will measure the pressure gradient in the pulmonary artery from the right ventricular outflow tract and examine the concordance with the results of right heart catheter and changes before and after TPVI.Materials and Methods
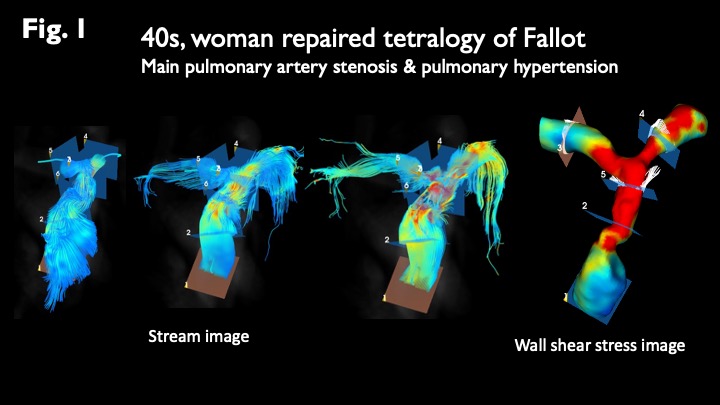
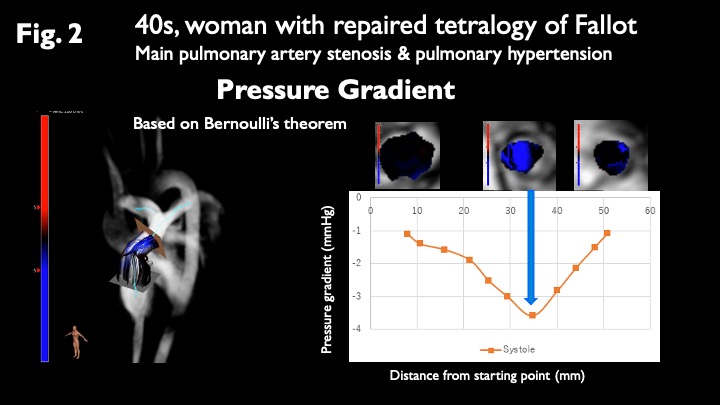
10 patients with repaired TOF scheduled for TPVI (mean age, 44 years) who underwent cardiac MRI and right heart catheterization were enrolled. All participants underwent MRI using a 3.0-Tesla whole-body imager (Ingenia 3 T Release 5.6; Philips Healthcare, Best, the Netherlands) equipped with a dual-source parallel resonance frequency (RF) transmission and 32-element D torso coil for RF reception. A flow-sensitive 3D gradient sequence with echo planar imaging (EPI), VENC 150–200 cm/s, and 14 frames/cycle was used as a 4D flow MRI. Free breathing was allowed and no respiratory motion compensation was performed. The 4D flow imaging and pressure gradient calculations were performed using a dedicated post-processing software for 4D flow MRI (ISP, Philips Healthcare, Best, the Netherlands).Stream images and wall shear stress images were reconstructed (Fig. 1) and pressure gradient were calculated (Fig. 2).Results and Discussion
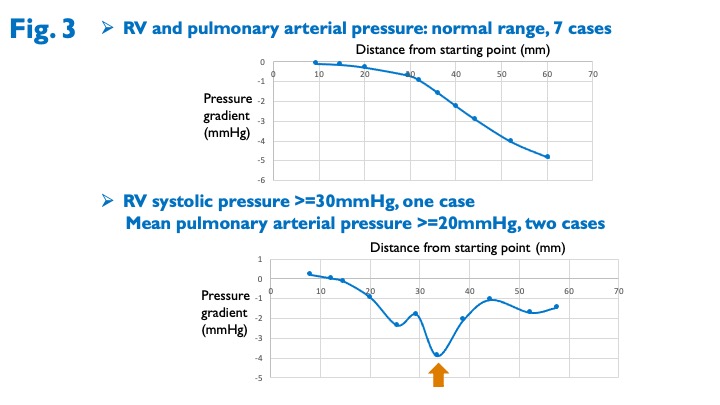
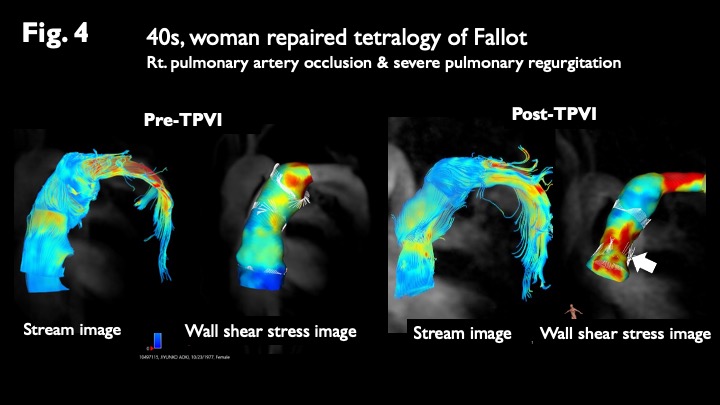
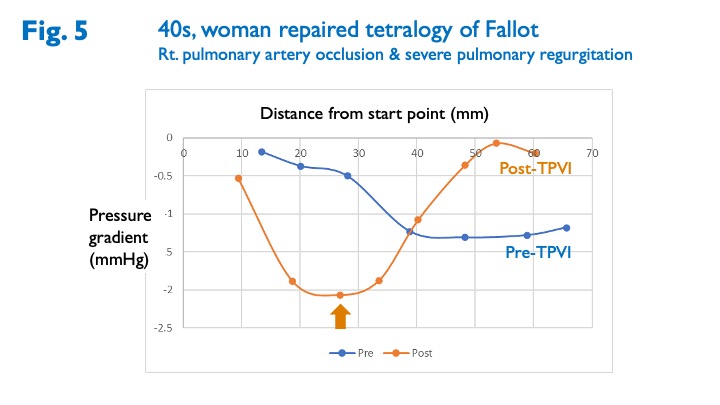
When pulmonary artery pressure is normal (n=7), the pressure gradient increases slowly with increasing distance from the starting point. In cases of pulmonary hypertension (n=3), a sudden drop in pressure occurs between the right ventricular outflow tract and the pulmonary artery bifurcation (Fig. 3). It has been demonstrated that a pressure gradient occurs in pulmonary hypertension. 4D flow imaging was also compared in three patients who underwent cardiac MRI before and after TPVI. In common with the three patients, pulmonary regurgitation and vortical flow disappeared after TPVI and wall shear stress was increased at the stenting site. A new in-stent pressure gradient developed in a case with increased wall shear stress over the entire length of the stent (Fig. 4 and 5). New pressure loading is a risk for right heart failure and requires further follow-up. Various cardiac function indices have been proposed from 4D flow MRI2, 3), but this is the first method to present absolute values of the pressure range.Conclusion
Dedicated 4D flow MRI pressure gradient measurements can be a noninvasive method to identify the site and degree of pressure gradient in the right ventricular outflow tract to the pulmonary artery in the remote postoperative period after repaired TOF. The presence or absence of a pressure gradient is important information for the indication of TPVI and postoperative monitoring.Acknowledgements
No acknowledgement found.References
1. L Bergersen et. al., JACC: Cardiovascular Interventions, 20172.
2. Shiina Y, et al. 4D flow MRI-derived energy loss and RV workload in adults with tetralogy of Fallot. Journal of Cardiology 2023. DOI: 10.1016/j.jjcc2023.10.0033.
3. Tsuchiya N, et al. Circulation derived from 4D flow MRI correlates with right ventricular dysfunction in patients with tetralogy of Fallot. Scientific Reports 2021; 11: 11623.
Figures