3534
3D image-navigator based Whole-Heart Imaging at 0.55T: comparison to 1.5T1School of Biomedical Engineering and Imaging Sciences, King’s College London, London, UK, London, United Kingdom, 2Royal Brompton Hospital, Guy's and St Thomas' NHS Foundation Trust, London, United Kingdom, 3Institute for Biological and Medical Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile, Santiago, Chile, 4School of Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile., Santiago, Chile, 5School of Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile, Santiago, Chile, 6Millennium Institute for Intelligent Healthcare Engineering, Chile, Santiago, Chile, 7Technical University of Munich, Germany; Institute of Advanced Study, Munich, Germany, Munich, Germany
Synopsis
Keywords: Vascular, Cardiovascular, low-field, congenital heart disease
Motivation: Low-field MRI is promising to enhance equity in medical care and accessibility for obese, claustrophobic patients and patients with implanted electronic devices. The investigation of the performance of 3D whole-heart imaging at low-field is still limited.
Goal(s): To implement and evaluate a free-breathing image-navigator based framework for 3D whole-heart imaging with isotropic resolution at 0.55T.
Approach: A 3D whole-heart free-breathing framework including image-based navigation, respiratory motion-correction reconstruction and patch-based denoising was implemented at 0.55T. The diagnostic performance of 3D whole-heart imaging was evaluated versus its counterpart at 1.5T.
Results: 3D whole-heart imaging at 0.55T offers good image and diagnostic quality, comparable to 1.5T.
Impact: This study demonstrates that high-quality 3D whole-heart imaging can be achieved at 0.55T showing comparable image and diagnostic quality to the current clinical standard in both healthy subjects and clinical patients, paving the pathway for affordable and accessible MRI.
Background
3D whole-heart imaging is an established modality for the anatomical assessment of the cardiothoracic vasculature and is currently clinically performed at 1.5T and 3T [1]. Nevertheless, its application is restricted to large, urban, academic medical centers in high-income countries. Additional limitations include challenges for severely obese and claustrophobic patients and for the growing number of patients with cardiac implanted electronic devices [2]. Recent developments in low-field (<1T) MRI technology have opened new opportunities to address some of these challenges [3]. A 3D whole-heart free-breathing framework including image-based navigation, respiratory motion-corrected reconstruction and patch-based denoising was implemented at 0.55T [4]. In this study, we assessed whether this approach was able to provide diagnostic images that were clinically comparable to those acquired at 1.5T with a similar framework.Methods
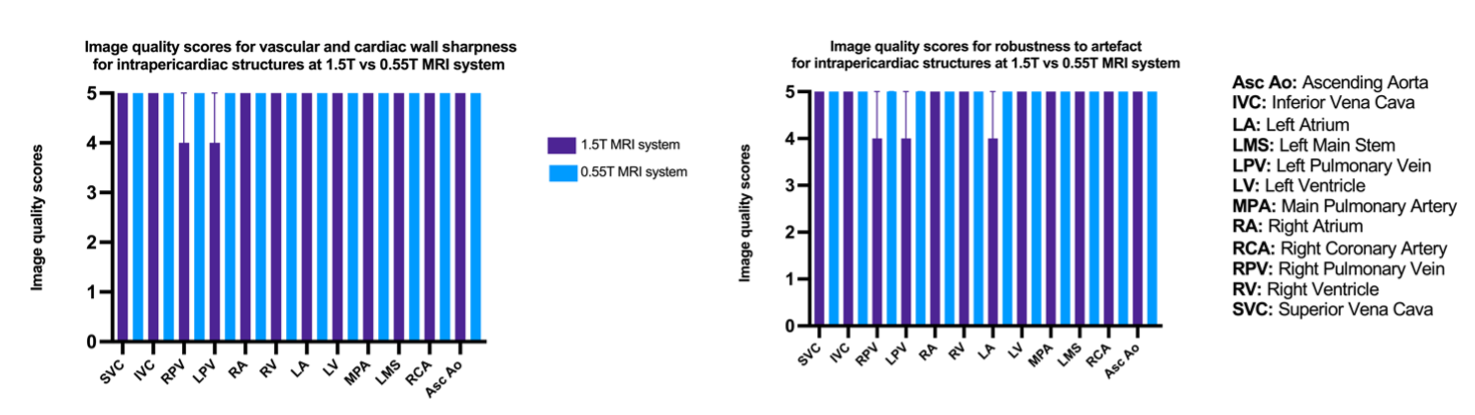
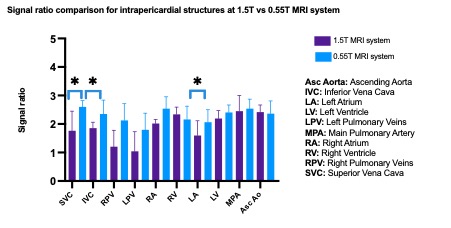
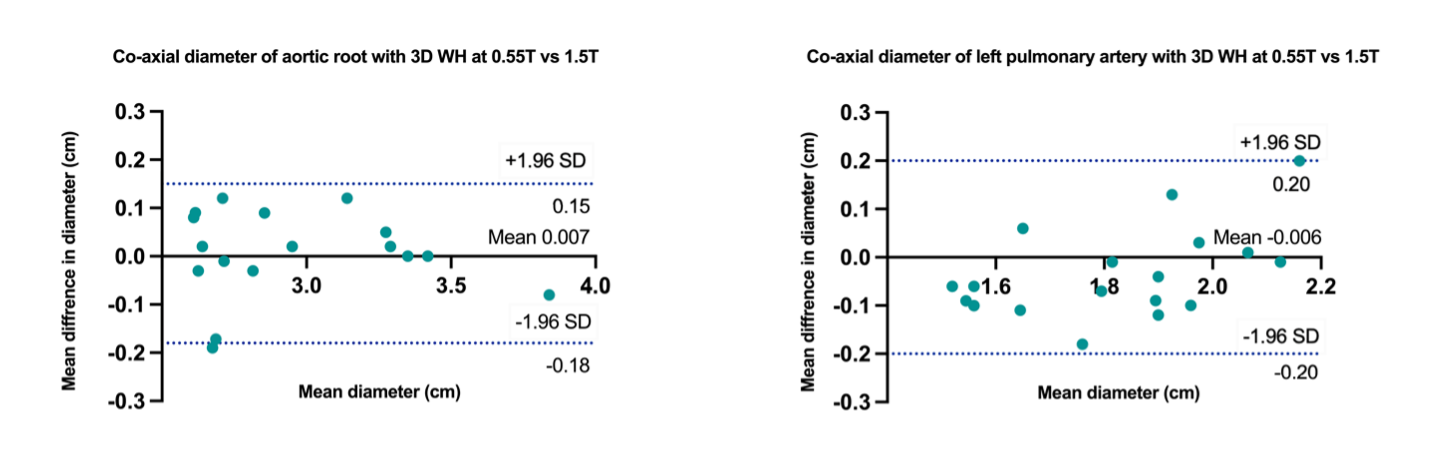
Ten healthy subjects and two patients with adult Congenital Heart Disease (mean age 30±2 years, 7 female) were scanned with an ECG-triggered, free-breathing 3D T2prep-bSFFP research sequence, acquired with image-based navigation (iNAV) for respiratory non-rigid motion correction and low-rank based denoising (3D-PROST) [5,6] at 0.55T and 1.5T (MAGNETOM Free.Max and MAGNETOM, Aera, Siemens Healthineers, Erlangen, Germany). Acceleration was a 3-fold for the healthy volunteers and 4-fold for the patients, both with undersampled variable-density Cartesian trajectory with spiral profile order [7]. Imaging parameters at 0.55T include: FOV = 312 x 312 x 120 mm, TE/TR = 2.65/ 5.3 ms, T2-prep duration = 50 ms, fat sat flip-angle = 180o, bandwidth: 800 Hz/Px. Imaging parameters at 1.5T include: FOV: 400x300x72-108 mm, T2-prep duration = 40ms, TE/TR = 1.7/3.4 ms, fat sat flip-angle = 130o, bandwidth = 919 Hz/px. Both acquisitions were performed with a resolution of 1.5 mm3, flip-angle = 90o and in coronal orientation. There was up to 60-day interval for the healthy volunteers and less than 14-days interval for the patients. A six-channel and 18-channel anterior coils were employed at 0.55T and 1.5T respectively, in combination with the respective spine coil. Diagnostic quality of the intrapericardial structures with regards to sharpness of vascular borders and robustness to artefacts was assessed and compared between the 0.55T and 1.5T acquisitions using a 1-5 Likert scale [(1: non-diagnostic, 5: excellent depiction of cardiac/vascular borders, ≥3: diagnostic), (1: non-diagnostic, severe artifact, 5: minimal artifact, ≥3: diagnostic)]. The signal ratio between blood and myocardium was computed in the respective intrapericardial structures. Comparison for the image quality scores and the signal ration was performed with a paired Wilcoxon-signed-rank test to assess statistical differences. Bland-Altman plots were used to assess the agreement and bias in aortic root and left pulmonary artery co-axial measurements.Results
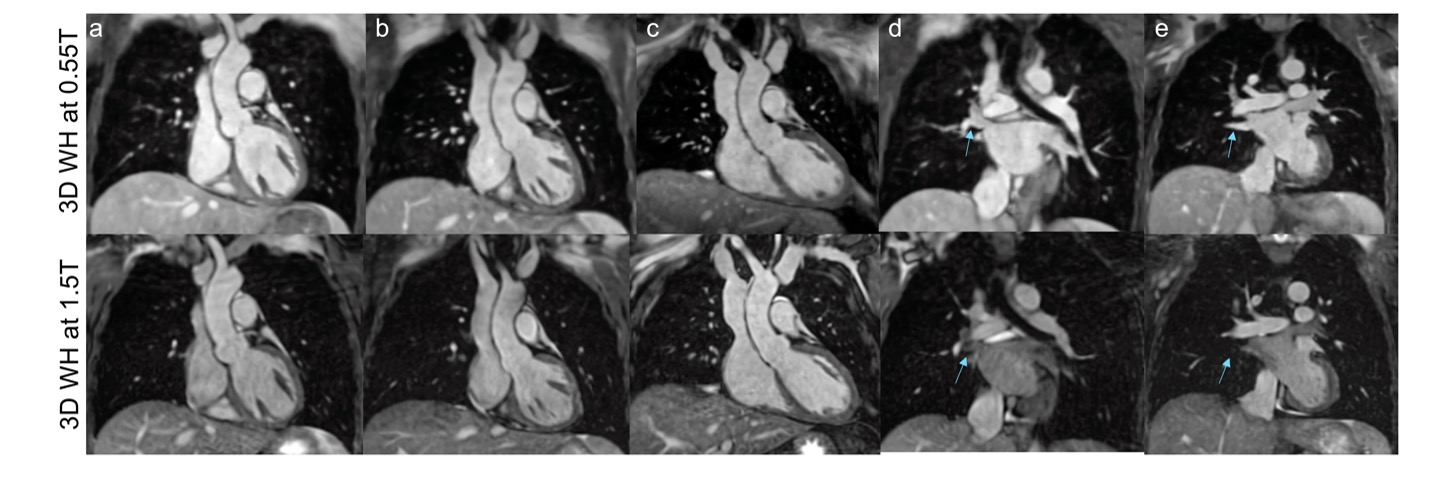
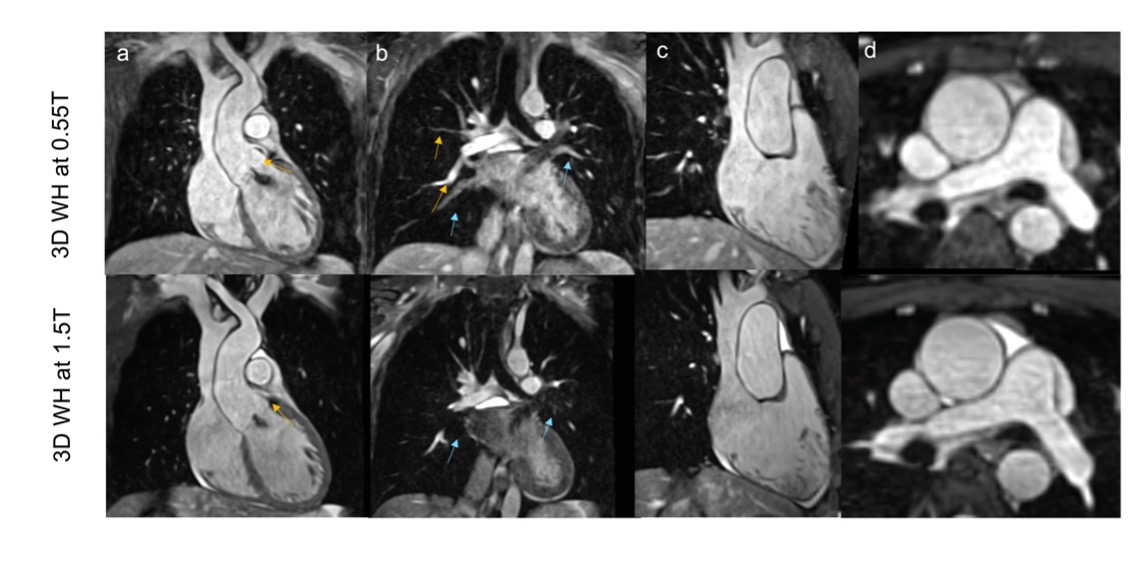
Scan time was shorter at 1.5T, 4.3(4.1, 4.4) min vs 5.1(4.9, 5.4) min, p=0.04. Good image quality and good quality depiction of all cardiac segments was achieved with the proposed framework at 0.55T for both healthy subjects and patients. In particular, off-resonance artefacts near high-susceptibility anatomy such as the lungs were attenuated at 0.55T (Fig. 1 & 2). Image quality scores were comparable between the two approaches for all the intrapericardiac structures (Fig. 3). Signal ratio comparison demonstrated comparable results with both approaches for all structures, except the pulmonary veins and left atrium where the proposed approach at 0.55T was superior (Fig. 4). Narrow limits of agreement were found between the 0.55T and the 1.5T vascular measurements (Fig. 5).Discussion
The proposed motion corrected free-breathing 3D whole-heart imaging sequence at 0.55T can achieve diagnostic image quality that is adequate, and often superior to 1.5T for the intrapericardial structures, in healthy subjects and adult patients with congenital heart disease, albeit with slightly longer scan time. This was partly due to longer TR in view of limited gradient performance and the longer RF duration, which was applied to enable higher flip angles to enhance SNR. At the same time reduced susceptibility and greater homogeneity, improved the delineation certain cardiovascular structures and holds promise for further acceleration, utilising advanced low-rank based reconstruction techniques.Conclusion
Future validation in a large cohort of patients with complex anatomy, where off-resonance and flow-related artefacts are more pronounced is warranted to facilitate further understanding of its clinical potential and potential clinical integration.Acknowledgements
The authors acknowledge financial support from: (1) BHF RG/20/1/34802 (2) EPSRC EP/V044087/1 (3) ANID Millennium Institute iHEALTH, ICN2021_004; Fondecyt 1210637 and 1210638; Basal Funding, IMPACT, FB210024 and (6) the Technical University of Munich – Institute for Advanced Study.References
1. Greil G et al. 3D Whole Heart Imaging for Congenital Heart Disease. Front Pediatr. 2017;5:36. Published 2017 Feb 27. doi:10.3389/fped.2017.00036.
2. Miller JD et al. Implantable Electronic Cardiac Devices and Compatibility With Magnetic Resonance Imaging. J Am Coll Cardiol. 2016;68(14):1590-1598. doi:10.1016/j.jacc.2016.06.068.
3. Campbell-Washburn et al. Low-field MRI: A report on the 2022 ISMRM workshop. Magn Reson Med. 2023; 90(4): 1682-1694. doi: 10.1002/mrm.29743.
4. Castillo-Passi C et al. Whole-Heart Cardiovascular Magnetic Resonance Angiography (CMRA) with iNAV-based Non-Rigid Motion-Corrected Reconstruction at 0.55T In: ISMRM 2023.; 3-8June 2023;Toronto.
5. Bustin A et al.Five-minute whole-heart coronary MRA with sub-millimeter isotropic resolution, 100% respiratory scan efficiency, and 3D-PROST reconstruction. Magn Reson Med, 2019. 81(1): p. 102-115.
6. Fotaki A et al. Efficient non-contrast enhanced 3D Cartesian cardiovascular magnetic resonance angiography of the thoracic aorta in 3 min. J Cardiovasc Magn Reson, 2022. 24(1): p. 5.
7. Prieto C et al. Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. J Magn Reson Imaging, 2015. 41(3): p. 738-46.
Figures