3533
Differentiation of cardiac inflammatory diseases by myocardial cine T2 mapping1Tokyo Women's Medical University, Tokyo, Japan, 2Philips Japan, Tokyo, Japan
Synopsis
Keywords: Inflammation, Infiltration, Cardiomyopathy
Motivation: Development of a non-contrast differential method for cardiac inflammatory disease
Goal(s): Accurate identification of cardiac sarcoidosis and myocarditis
Approach: Cardiac cine imaging to project T2 values using T2prep-based T2 mapping with dynamic multiple trigger-delay framework
Results: Diastolic cine T2 values (54.2msec.) discriminated cardiac sarcoidosis from myocarditis with an AUC of 0.879, sensitivity of 86%, and specificity of 77%.
Impact: This method is a new technique that captures changes in myocardial properties during the cardiac cycle without the use of contrast media.
Introduction
Cardiac sarcoidosis and myocarditis are typical cardiac inflammatory diseases that have reached the chronic stage. Both diseases are often associated with ventricular arrhythmias and a high risk of sudden death. Gadolinium contrast late enhanced MRI is conventionally used to differentiate between the two diseases, but their similar distribution often makes it difficult to distinguish between them. The perfusion pressure in the myocardium fluctuates with the cardiac cycle in parallel to left ventricular pressure. Changes in perfusion pressure are thought to alter the migration of water components in the myocardium and the degree of edema. They are thought to be related to the pathogenesis of cardiomyopathy, but effective biological imaging has not been established. We devised cine T2 mapping, which projects T2 values onto cardiac cine imaging, and examine whether it could be used to differentiate cardiac inflammatory diseases.Materials and Methods
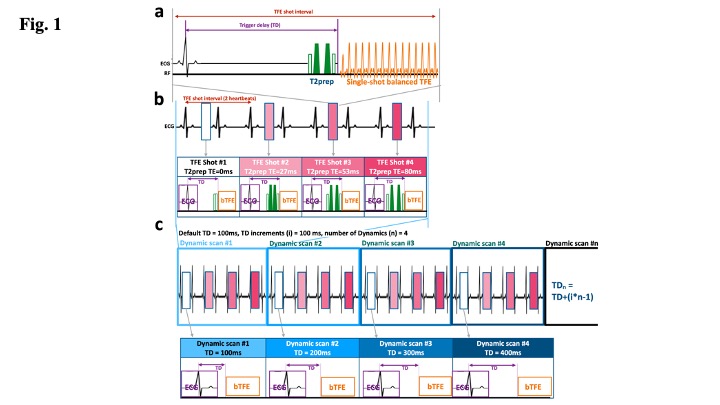
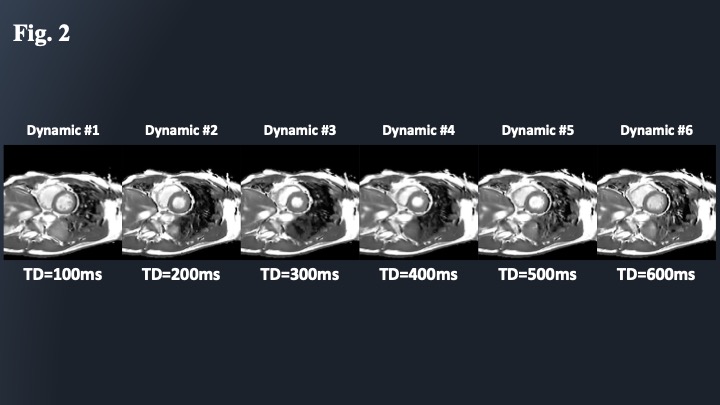
Thirteen patients with chronic myocarditis and 7 patients with cardiac sarcoidosis whose diagnosis was confirmed by myocardial biopsy were enrolled. All participants underwent MRI using a 3.0-Tesla whole-body imager (Ingenia 3 T Release 5.6; Philips Healthcare, Best, the Netherlands) equipped with a dual-source parallel resonance frequency (RF) transmission and 32-element D torso coil for RF reception. CMR protocol consisted of standard cine imaging, T1 mapping (modified Look-Locker inversion recovery sequence with a 3(3)5 scheme, MOLLI), T2 mapping (T2-prep), T2 Black-Blood, and late gadolinium enhancement (LGE).In addition, CINE T2 mapping with 6 frames per heartbeat was performed using multiple breath-hold T2prep-based single-shot balanced turbo-field echo T2 mapping with dynamic multiple trigger-delay framework (DynTD). DynTD is based on the dynamic scan procedure with variable trigger delay among different dynamic scans, resulting in different time-phase T2 maps in one scan. For generating the T2 map, four images with different T2-preparation times (TE = 0, 27, 53 and 80ms) were acquired with interleaved acquisition at the respective heartbeats. The repetition time (TFE shot interval) was set to 2 heartbeats. Furthermore, fast elastic image registration (FEIR) is applied to minimize motion-induced misalignment, which can mitigate small changes of in-plane heart movement by registering the source images before creation of the T2 maps (Fig. 1)1,2,3).In cine T2 mapping, a total of 6 heart phases of the maps were acquired (Fig. 2), and T2 maps of systolic and diastolic phases were visually selected and T2 values of both phases were measured and evaluated. T2 values were measured at the same locations in the conventional T2 map (T2-prep).Results and Discussion
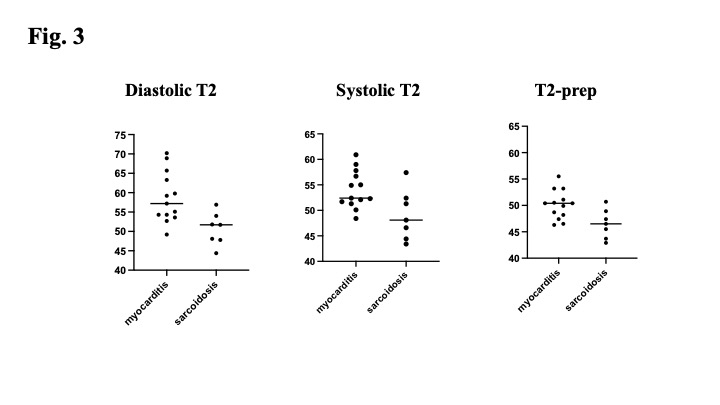
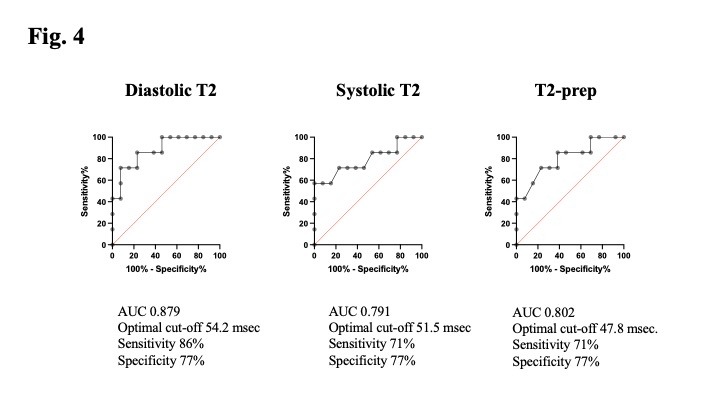
Both diastolic and systolic T2 values on the cine T2 map and T2 values on conventional T2 map were significantly higher in chronic myocarditis than in cardiac sarcoidosis (diastolic T2, 58.7±6.5 msec. versus 50.7±4.2 msec.; systolic T2, 54.1±3.7 msec. versus 49.1±4.9 msec.; conventional T2, 50.1±2.7 msec. versus 46.5±2.8 msec., respectively. p<0.05) (Fig. 3).The discriminatory power of ROC analysis using the optimal threshold was an area under the curve (AUC) 0.879, sensitivity 87%, and specificity 77% for diastolic T2 (54.2msec.), AUC 0.791, sensitivity 71%, and specificity 77% for systolic T2 (51.5msec.), and AUC 0.802, sensitivity 71%, and specificity 77% for conventional T2 (47.8msec.).Conclusion
Cine T2 mapping is a new noninvasive in vivo imaging technique for myocardial edema that provides an effective means of differentiating inflammatory cardiac diseases. The diastolic T2 value is a useful indicator for differentiating myocarditis from cardiac sarcoidosis.Acknowledgements
No acknowledgement found.References
1. Kato M, et al. Rapid multiple-breath-holds myocardial CINE T2mapping with dynamic multiple trigger delay acquisition. ISMRM 20232.
2. Kodaira, K, et al. Whole-heart simultaneous CINE T2mapping and coronary MR angiography. ISMRM 20233.
3. Nagao M, et al. Cine T2 mapping reveals cardiac cycle-dependent T2 variability in cardiomyopathy. ISMRM 2023
Figures