3530
Impact of pegloticase on cardiovascular function in young-onset Type 2 Diabetes1Department of Radiology, Children's Hospital Colorado, University of Colorado Anschutz Medical Campus, Aurora, CO, United States, 2Institute of Medical Devices, Kangwon National University, Chuncheon, Korea, Republic of, 3Department of Pediatrics, Division of Endocrinology, University of Colorado School of Medicine, Aurora, CO, United States, 4Department of Bioengineering, University of Colorado Anschutz Medical Campus, Aurora, CO, United States
Synopsis
Keywords: Myocardium, Safety, Youth-onset T2D, CMR, 4D flow MRI
Motivation: Increasing prevalence of youth-onset type 2 diabetes (T2D) is a global concern and characterized by a higher risk for hyperuricemia, a strong risk factor for cardiovascular disease (CVD).
Goal(s): Studies have shown that serum uric acid (SUA) lowering in the general population may confer cardiovascular protection, but there have been no studies on its effectiveness in young adults with T2D.
Approach: Here, we hypothesized aggressive SUA lowering using single intravenous infusion dose of the uricase, pegloticase, will attenuate cardiac magnetic resonance imaging (CMR) markers of CVD in young adults with T2D.
Results: Unexpectedly, we documented impaired CMR-based global longitudinal strain after pegloticase infusion.
Impact: Our study demonstrates the impacts of a drug therapy to reduce serum uric acid in youth-onset T2D and its impact on cardiovascular function using CMR. A comprehensive examination of the cardiovascular effects of the therapy is required for youth-onset T2D.
Introduction
Youth-onset type 2 diabetes (T2D) is a global concern, accounting for approximately 41,600 new cases of T2D globally in 20211 and is expected to increase fourfold in the United States by 20502. People with youth-onset T2D are susceptible to a higher risk of cardiovascular disease (CVD) and progression3. Youth-onset T2D also exhibits a suboptimal response to current therapeutic approaches4. Identifying new therapeutic targets is critical to address the substantial health implications of youth-onset T2D.We previously found that 50% of males with youth-onset T2D have a high serum uric acid (SUA) level exceeding 6.8 mg/dL5. In a seven-year follow-up we also demonstrated that elevated SUA is associated with the development of hypertension and diabetic kidney disease, and it is also believed to contribute to the progression of cardiovascular disease6. While the effectiveness of reducing SUA in the general population has been investigated, there are no studies evaluating the efficacy of SUA lowering in youth-onset T2D. Therefore, we aim to explore the feasibility of lowering SUA in youth-onset T2D using pegloticase, an FDA-approved treatment for adults with chronic gout, and to test its impact on cardiovascular function.
Methods
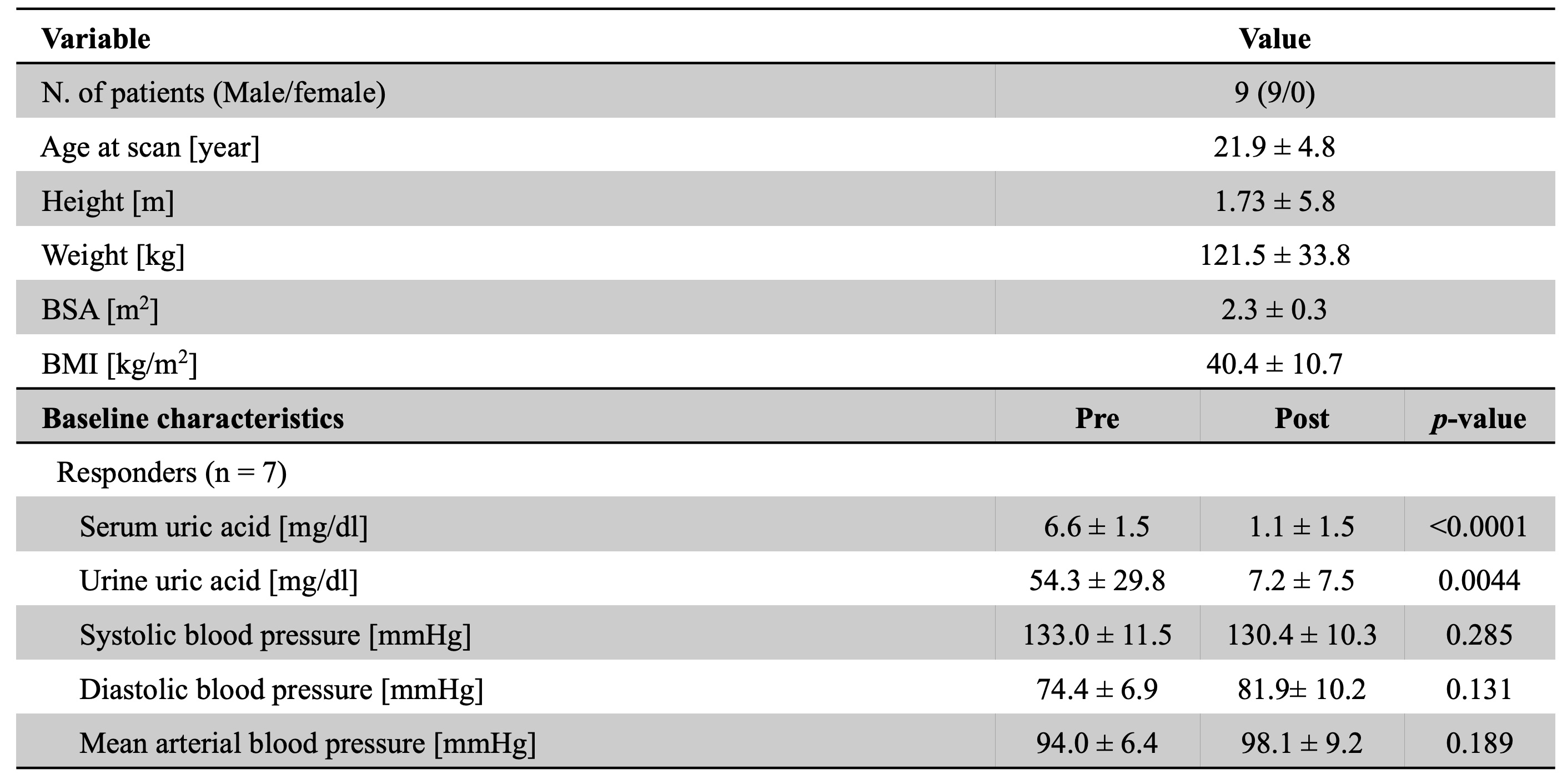
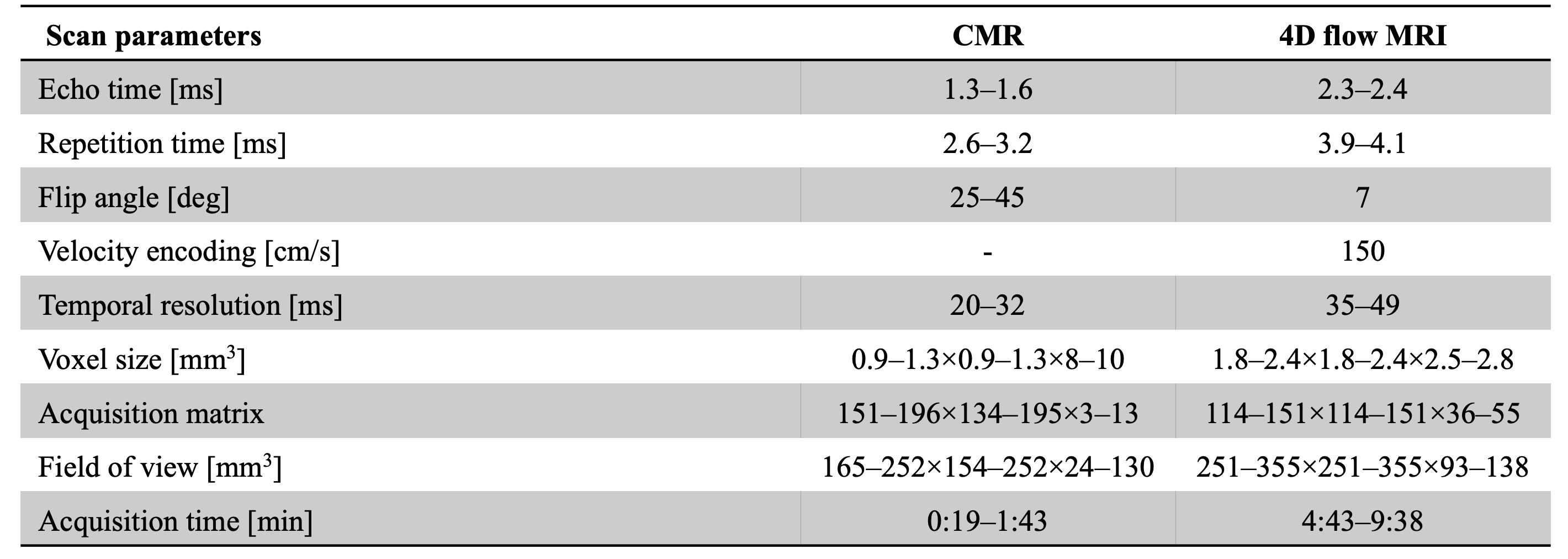
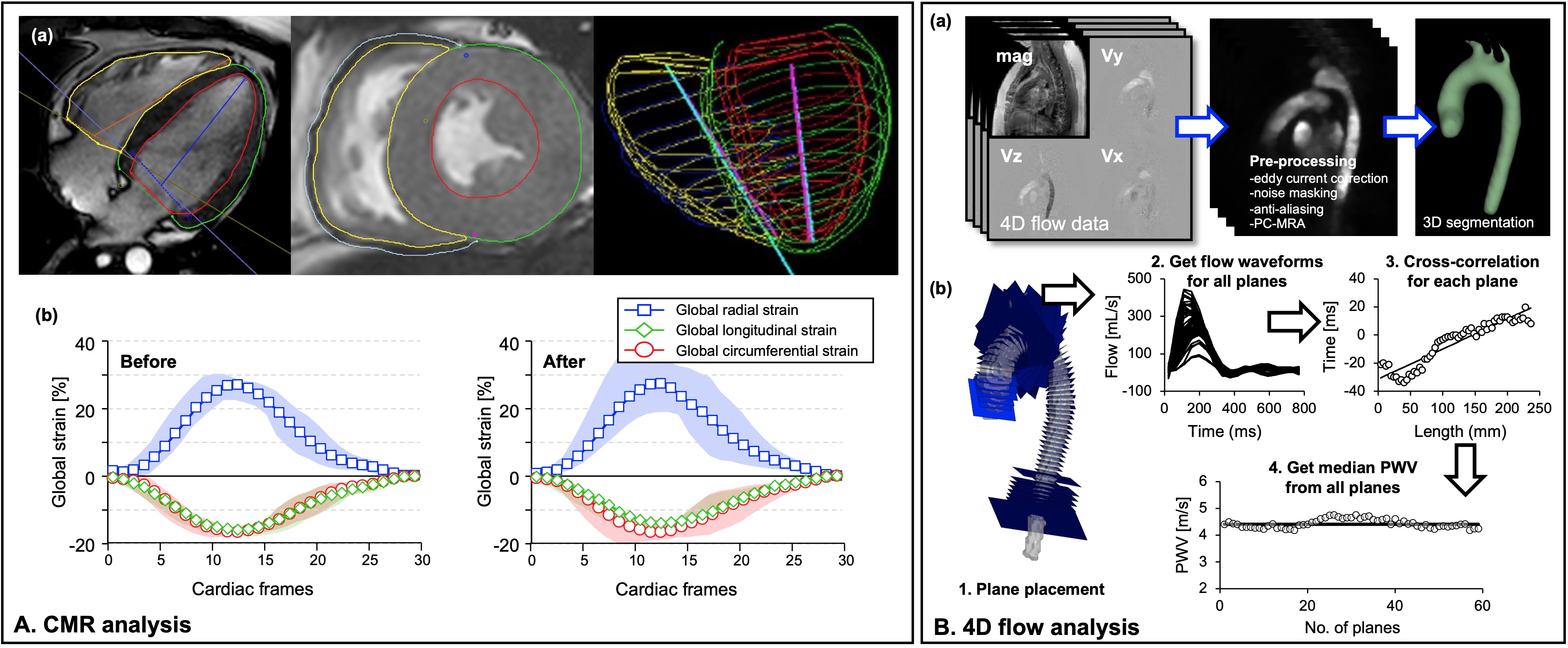
Ten young adults were prospectively recruited to undergo a single dose of intravenous pegloticase infusion (8 mg). Of these, one patient was excluded due to no follow-up MRI scan. The mean age of the participants were 23±5 years with a mean BMI 36±6 kg/m2; additional demographics shown in Table 1. Patients had no history of prior cardiovascular events, and they were asked to fast prior to their pre- and post-therapy study visits, which included urine and blood collections. Cardiac magnetic resonance imaging (CMR) and time-resolved three-dimensional flow sensitive CMR (4D flow MRI) images were acquired before pegloticase infusion and after one-week using a 3T Philips Ingenia MRI system (Philips Healthcare, Best, Netherlands; scan parameters in Table 2). Responders, defined as those who had a decreased SUA more than 3 mg/dL, were included in the results. Global function and strain changes were measured using time-resolved CMR, while pulse wave velocity (PWV) was obtained through 4D flow MRI analysis employing machine learning-based auto-segmentation7 (Fig. 1). Paired two-tailed t-test was performed to assess statistical significance between pre and post pegloticase infusion.Results
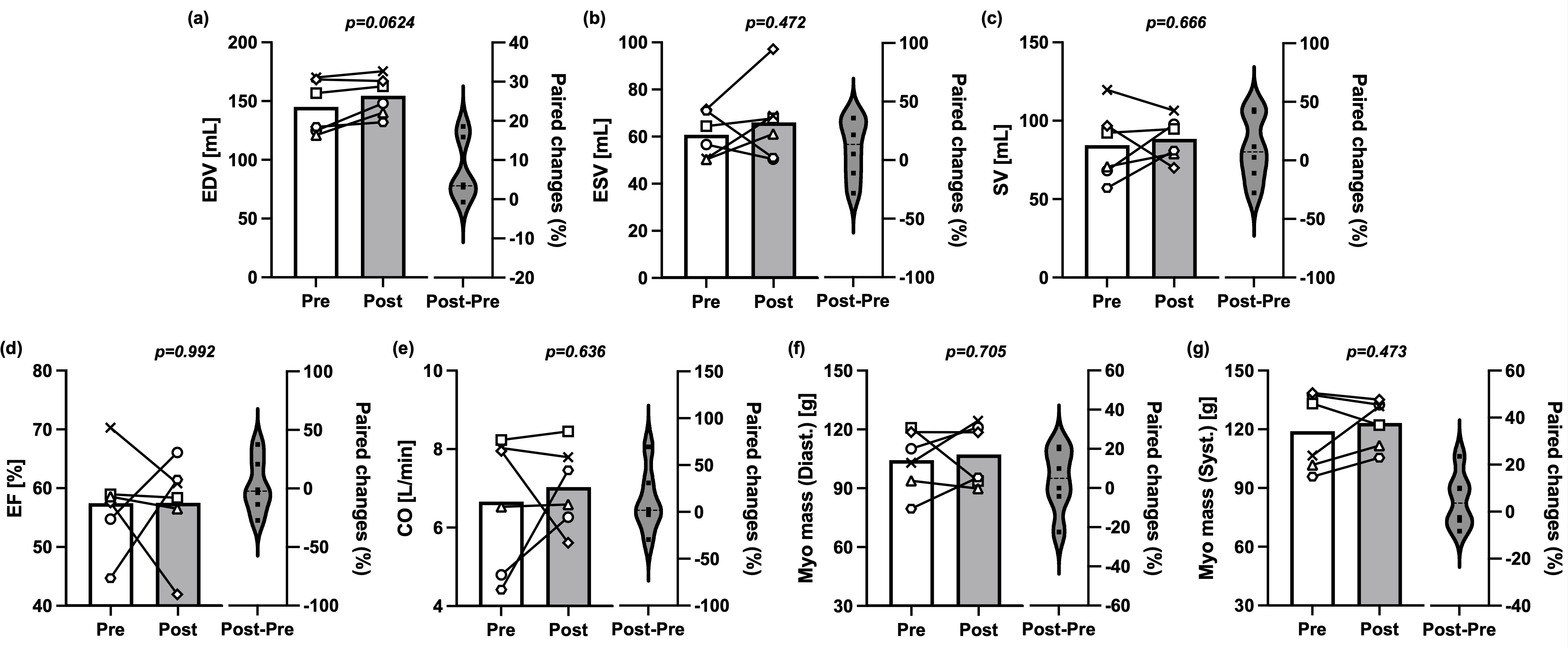
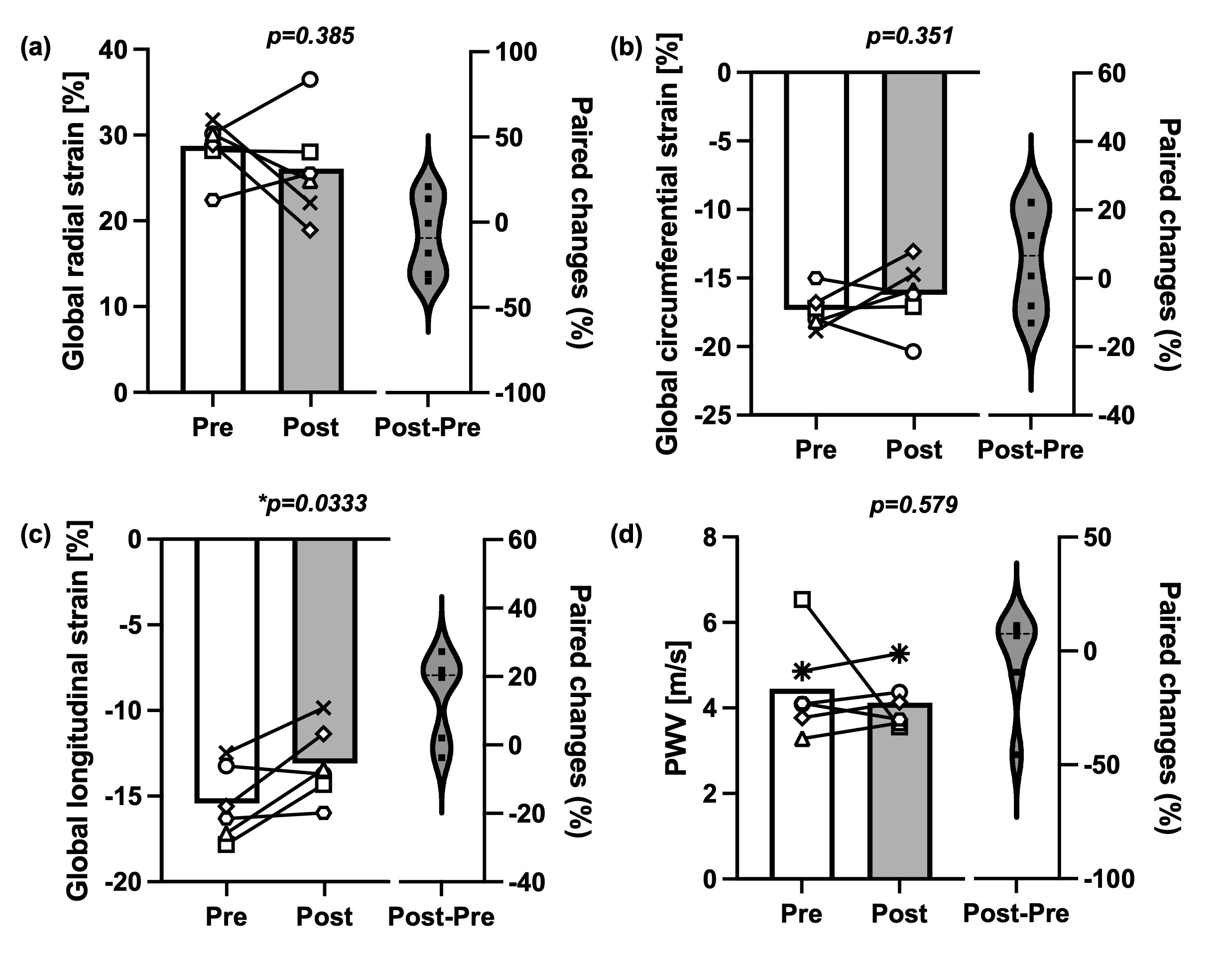
Out of nine patients, two from each imaging series (CMR or 4D flow) were further excluded due to low image quality or missing data. Pegloticase infusion significantly decreased SUA (p<0.0001); blood pressure did not change (Table 1). CMR results show that end-diastolic volume (EDV) trended toward an increase (p=0.06), while other volume-based indices were not significantly different (Fig. 2). The magnitude of global longitudinal strain (GLS) was significantly decreased, indicating a decrease in cardiac function (p=0.03) (Fig. 3). No significant differences were found for vascular stiffness as measured by PWV (p=0.58).Discussion
Pegloticase is highly effective at lowering SUA, but it is typically considered a last resort due to concerns about infusion reactions, the burden of the infusion process, and the potential risk for deleterious cardiovascular effects. Notably, heart failure and hospitalization have been reported during pegloticase therapy8.Our CMR results indicate an adverse, quantitative effect on cardiac function following pegloticase infusion, as measured by a decrease in magnitude of GLS, a CMR biomarker known for prognostic value in patients with heart failure9. In addition, we observed that diastolic blood pressure and EDV show trends toward an increase. This may be associated with the results of previous study indicating that impaired GLS has shown a strong correlation with pressure-volume relationship10.
It is noteworthy that pegloticase treatment is also known to decrease blood pressure in older patients with gout11. However, our study showed that the use of pegloticase infusion to rapidly and aggressively lower SUA levels in young adults with T2D impacted GLS. This discrepancy might be attributed to differences in age, hemodynamic or inflammatory mechanisms12. The results show the potential for using CMR for a comprehensive examination of the cardiovascular effects of pegloticase therapy.
We also found that vascular stiffness as measured by PWV was not affected by pegloticase infusion, despite many studies demonstrating increased PWV in patients with diabetes or hyperuricemia13,14. This result is supported by a previous study demonstrating that UA levels are not well correlated with PWV in patients with hypertension and hyperuricemia during a follow-up period of 3.8 years15.
Acknowledgements
KHIDI HI22C1915 (SP)
Horizon Pharma
Supported by NIH/NCATS Colorado CTSA Grant Number UM1 TR004399. Contents are the authors’ sole responsibility and do not necessarily represent official NIH views
References
1. Wu, H., et al. Worldwide estimates of incidence of type 2 diabetes in children and adolescents in 2021. Diabetes Research and Clinical Practice 185, 109785 (2022).
2. Perng, W., Conway, R., Mayer-Davis, E. & Dabelea, D. Youth-Onset Type 2 Diabetes: The epidemiology of an awakening epidemic. Diabetes Care 46, 490-499 (2023).
3. Shah, R.D., et al. Cardiovascular risk factor progression in adolescents and young adults with youth-onset type 2 diabetes. Journal of Diabetes and its Complications 36, 108123 (2022).
4. Arslanian, S., et al. Evaluation and management of youth-onset type 2 diabetes: a position statement by the American Diabetes Association. Diabetes care 41, 2648 (2018).
5. Bjornstad, P., et al. Serum Uric Acid (SUA), Urinary Albumin Excretion (UAE), and Hypertension (HTN) in Adolescents with Type 2 Diabetes (T2D) in the TODAY Study. Diabetes 67(2018).
6. Morikawa, N., et al. Serum urate trajectory in young adulthood and incident cardiovascular disease events by middle age: CARDIA study. Hypertension 78, 1211-1218 (2021).
7. Fujiwara, T., et al. Segmentation of the Aorta and Pulmonary Arteries Based on 4D Flow MRI in the Pediatric Setting Using Fully Automated Multi‐Site, Multi‐Vendor, and Multi‐Label Dense U‐Net. Journal of Magnetic Resonance Imaging 55, 1666-1680 (2022).
8. Guttmann, A., Krasnokutsky, S., Pillinger, M.H. & Berhanu, A. Pegloticase in gout treatment-safety issues, latest evidence and clinical considerations. Therapeutic advances in drug safety 8, 379-388 (2017).
9. Park, J.J., Park, J.-B., Park, J.-H. & Cho, G.-Y. Global longitudinal strain to predict mortality in patients with acute heart failure. Journal of the American College of Cardiology 71, 1947-1957 (2018).
10. Aikawa, T., et al. Impaired left ventricular global longitudinal strain is associated with elevated left ventricular filling pressure after myocardial infarction. American Journal of Physiology-Heart and Circulatory Physiology 319, H1474-H1481 (2020).
11. Johnson, R.J., Choi, H.K., Yeo, A.E. & Lipsky, P.E. Pegloticase treatment significantly decreases blood pressure in patients with chronic gout. Hypertension 74, 95-101 (2019).
12. Lytvyn, Y., et al. Renal and vascular effects of uric acid lowering in normouricemic patients with uncomplicated type 1 diabetes. Diabetes 66, 1939-1949 (2017).
13. Liu, J., et al. Relationship between carotid-femoral pulse wave velocity and uric acid in subjects with hypertension and hyperuricemia. Endocrine Journal 66, 629-636 (2019).
14. Elias, M.F., Crichton, G.E., Dearborn, P.J., Robbins, M.A. & Abhayaratna, W.P. Associations between type 2 diabetes mellitus and arterial stiffness: a prospective analysis based on the Maine-Syracuse study. Pulse 5, 88-98 (2018).
15. Maloberti, A., et al. Pulse wave velocity progression over a medium‐term follow‐up in hypertensives: Focus on uric acid. The Journal of Clinical Hypertension 21, 975-983 (2019).
Figures