3529
Cardiovascular magnetic resonance-derived left ventricular hemodynamic force among patients with systemic lupus erythematosus1Department of Radiology, Xiangya Hospital Central South University, Changsha, Hunan, China., Changsha, China, 2Department of Radiology, Xiangya Hospital Central South University, Changsha, Hunan,, China., Changsha, China, 3Scientific Marketing, Siemens Healthineers Ltd., Wuhan, China, Wuhan, China, 4MR Collabration, Siemens Healthineers, Los Angeles, USA, Los Angeles, CA, United States
Synopsis
Keywords: Heart Failure, Cardiovascular
Motivation: Cardiovascular involvement in systemic lupus erythematosus (SLE) patients is common and serious; early and accurate identification of the cardiac dysfunction is crucial.
Goal(s): Our goal was to investigate the potential role of hemodynamic force (HDF) in early recognizing impaired cardiac function in SLE.
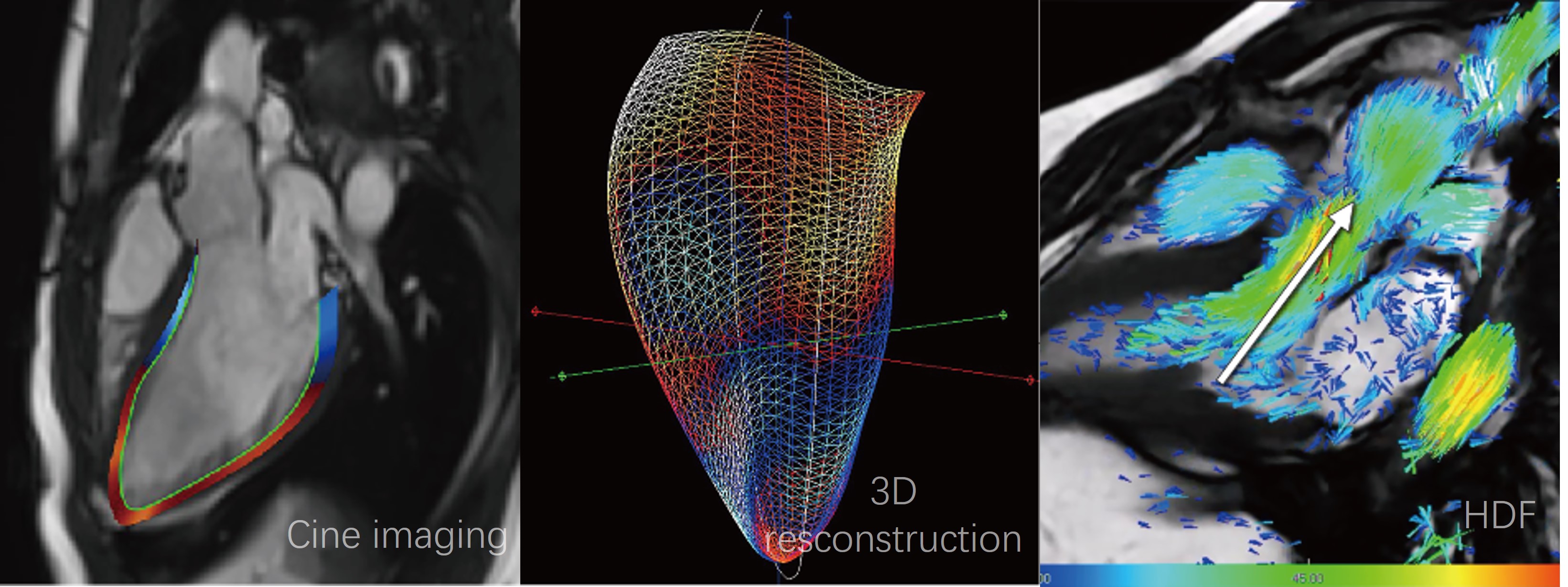
Approach: Left ventricular (LV) HDF and strain analysis were performed based on long-axis cine imaging using feature-tracking in 36 SLE patients and 34 healthy volunteers.
Results: The force ratio between transverse and longitudinal direction was larger in SLE patients with no difference of strain analysis, indicating that the orientation of HDF altered in LV.
Impact: This study demonstrated that HDF analysis can early detect systolic dysfunction in SLE in advance of significant decrease of LV EF, which may contribute to the early diagnosis of cardiac involvement and prognosis improvement of patients.
INTRODUCTION
Cardiovascular disease is a major cause of morbidity/mortality in patients with systemic lupus erythematosus (SLE)1. Since left ventricular (LV) ejection fraction (EF) can be preserved in the early stages of SLE, LV dysfunction should be assessed with more sensitive techniques. LV strain analysis and hemodynamic force (HDF) may be valuable in detecting subtle changes in LV mechanics; the value of HDF in SLE is unknown. Therefore, the aim of our study is to evaluate LV strain and HDF from cardiovascular magnetic resonance (CMR) cines in SLE patients.METHODS
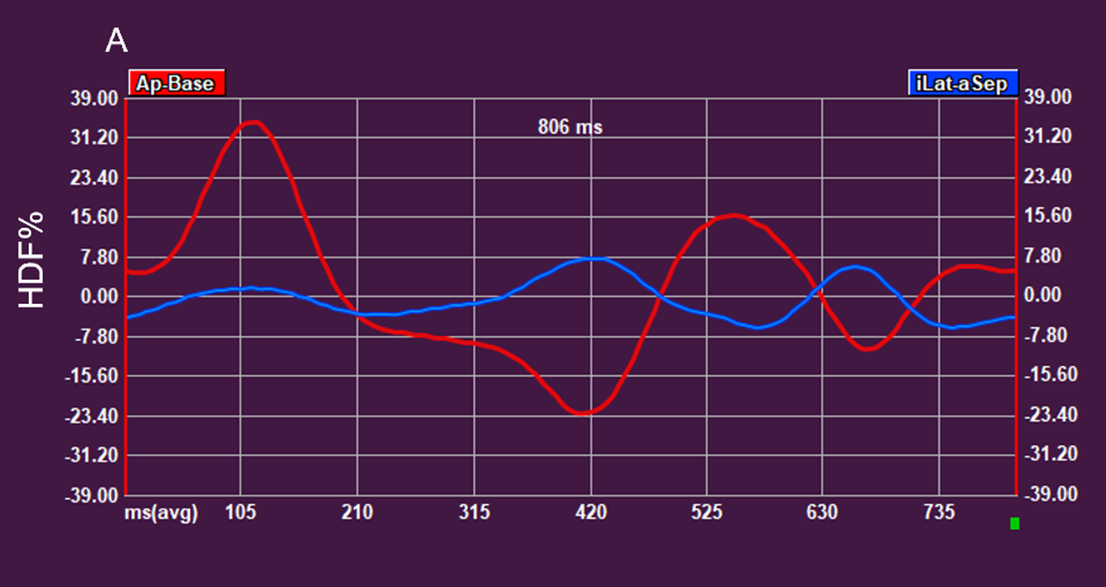
In this retrospective study, 36 SLE patients (20 patients with preserved EF (pEF) who were defined as LV EF ≥ 55%) and 34 healthy volunteers underwent CMR imaging. LV HDF was computed from a formulation with myocardial movement and velocity of the reconstructed 3D-LV (derived from long-axis cines using feature-tracking)2. To facilitate comparison between patients with different LV sizes, HDF is converted to percentage numbers by dividing the blood density and the acceleration of gravity. HDF assessment included the “apical-basal” (longitudinal) and “lateral-septal” (transverse) forces during systole and diastole, respectively, “apical-basal” force during the entire heartbeat and the systolic peak. The force ratio was calculated between transverse force and longitudinal force. LV global longitudinal strain (GLS) and global circumferential strain (GCS) were also measured using CMR feature tracking technique.RESULTS
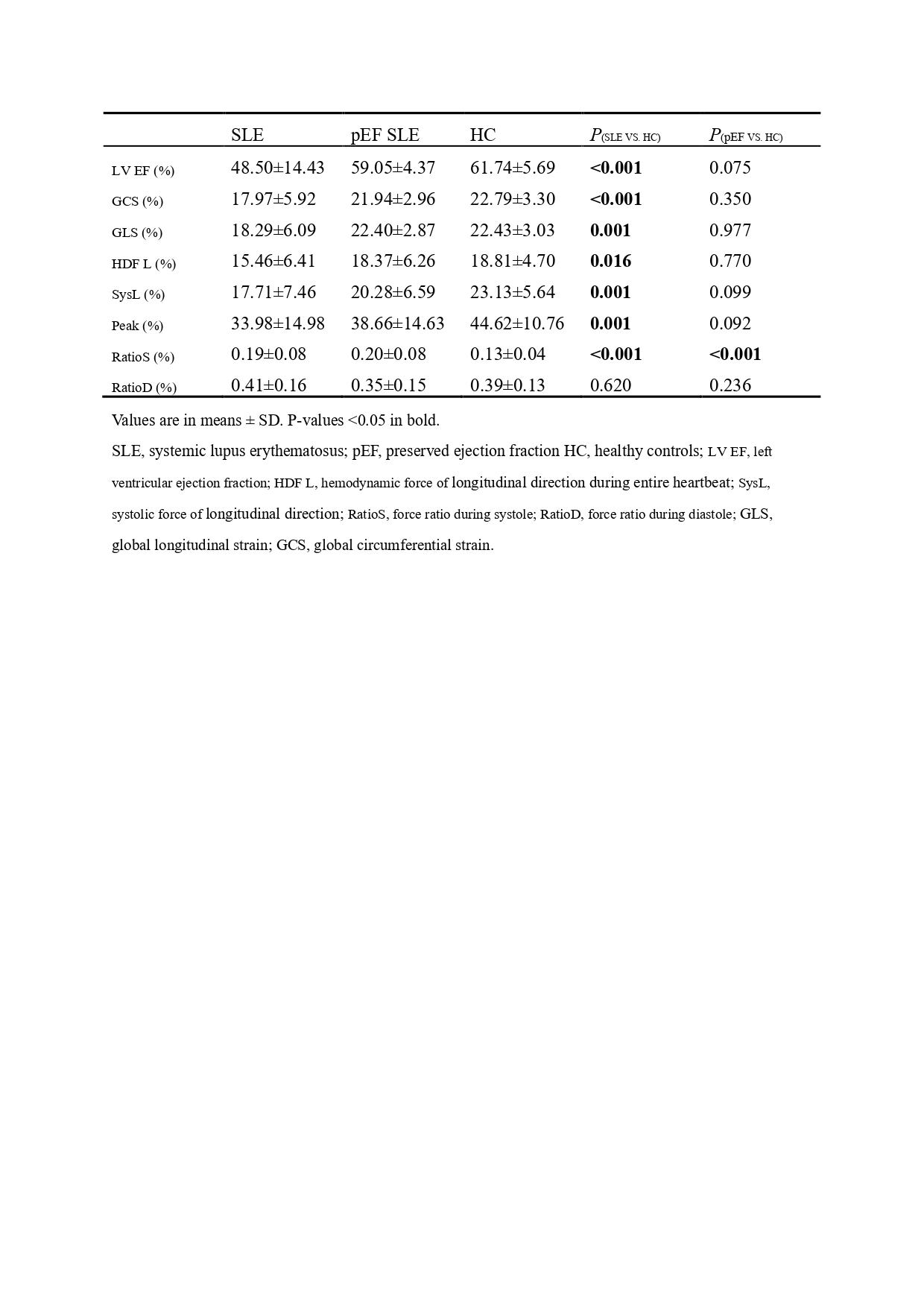
Compared to healthy volunteers, the force ratio during systole was higher in SLE patients (0.19±0.08% vs. 0.13±0.04%, P< 0.001); and the systolic function was impaired depicted by (i) lower LV EF (48.50±14.43% vs. 61.74±5.69%, P< 0.001) and (ii) lower systolic force (17.71±7.46% vs. 23.13±5.64%, P< 0.01) and systolic peak (33.98±14.89% vs. 44.62±10.76%, P< 0.01) and (iii) lower GCS (17.97±5.92% vs. 22.79±3.30%, P< 0.001) and GLS (18.29±6.09% vs. 22.43±3.03%, P< 0.01). In pEF SLE patients, the force ratio during systole was still higher (0.19±0.08% vs. 0.13±0.04%, P< 0.001) while no significant difference in strain analysis was found.DISCUSSION
HDF is the global force of cardiac motion acquired by integrating the intraventricular pressure gradient over the entire ventricle and thus may detect subtle heart injury before a significant decline of EF. In the spatial reference system, HDF is decomposed into three inter-perpendicular vectors in the left ventricle3. As the longitudinal force is nearly consistent with the blood flow during ejection, the force ratio can represent the extent of HDF deviating from the functional direction. In this study, we demonstrated that the LV HDF orientation was altered in pEF SLE patients when there was no obvious abnormality of LV strain analysis.CONCLUSION
LV systolic function impairment can be demonstrated by the alteration of HDF ratio in pEF SLE patients, HDF could therefore potentially be used as an early marker for LV functional assessment.Acknowledgements
noneReferences
1. Miner JJ, Kim AH. Cardiac manifestations of systemic lupus erythematosus. Rheum Dis Clin North Am. 2014;40:51-60. doi: 10.1016/j.rdc.2013.10.003IF: 2.3 Q4
2. Pedrizzetti G, Arvidsson PM, Toger J, Borgquist R, Domenichini F, Arheden H, Heiberg E. On estimating intraventricular hemodynamic forces from endocardial dynamics: A comparative study with 4D flow MRI. J Biomech. 2017;60:203-210. doi: 10.1016/j.jbiomech.2017.06.046IF: 2.4 Q3
3. Arvidsson PM, Toger J, Carlsson M, Steding-Ehrenborg K, Pedrizzetti G, Heiberg E, Arheden H. Left and right ventricular hemodynamic forces in healthy volunteers and elite athletes assessed with 4D flow magnetic resonance imaging. Am J Physiol Heart Circ Physiol. 2017;312:H314-H328. doi: 10.1152/ajpheart.00583.2016IF: 4.8 Q1
Figures