3527
Value of feature-tracking myocardial strain analysis in evaluation patients with immune checkpoint inhibitor (ICI) associated myocarditis1Department of Radiology, Peking University First Hospital, Beijing, China, 2Philips Healthcare, Beijing, China
Synopsis
Keywords: Myocardium, Heart, Immune checkpoint inhibitor; Myocarditis; Cardiac magnetic resonance; Feature-tracking; Strain
Motivation: Myocarditis is a potentially fatal complication of immune checkpoint inhibitors (ICI). More diagnostic tools are needed beside enzymes.
Goal(s): Data on CMR characteristics of ICI myocarditis is limited, especially the new strain analysis.
Approach: The study compared the cardiac functional and stain parameters between patients with ICI associated myocarditis and controls. The parameters included LVEF, CO, CI, EDV/BSA, ESV/BSA, and SV/BSA, incidence rate of myocardial edema and LGE, LS, CS, RS (global and segmental).
Results: For patients with ICI associated myocarditis, LVEF, ESV/BSA, CS (basal, mid, apical and global) and LS (mid, apical and global) may be effective parameters to identify myocardial injury.
Impact: Some CMR strain parameters and cardiac function indicators significantly impaired, which may be helpful for early detection and to evaluate treatment effectiveness of ICI associated myocarditis.
INTRODUCTION
ICI associated myocarditis is a immune-related adverse event that is characterized by a high mortality rate1. More diagnostic and surveillance tools are needed beside myocardial enzymes2,3. CMR is a non-invasive imaging method that has established criteria for the diagnosis of myocarditis4. But data on CMR characteristics of ICI associated myocarditis is limited, especially the new strain analysis based on feature-tracking (FT) technique5.The purpose of this study is to investigate CMR manifestations and the diagnostic value of myocardial strain analysis in patients with suspected acute ICI associated myocarditis.
METHODS
1. Patients. The study population consisted of patients with defined acute ICI associated myocarditis and control subjects. Subjects of ICI associated myocarditis diagnosed in our center from January 1, 2019 to September 30, 2023 were retrospectively collected. The diagnosis of acute myocarditis was made by myocardial biopsy or clinical diagnosis. Patients with history of heart disease such as myocardial infarction, myocarditis were excluded.2. CMR scan. CMR scans were performed on a 3.0 Tesla MR system (Ingenia, Philips Healthcare) with a cardiac phased-array coil. For functional and strain analysis ECG-gated steady-state free precession cine images were obtained in short axis, four-chamber, three-chamber and two-chamber views. Conventional sequences are included as T2 STIR, EGE and LGE.
3. Image analysis. Two physicians experienced in CMR (K.Z. and W.L., 10 and 15 years experience in cardiac MRI) analysed the data and performed the measurements. All readers were blinded to the patient information. Cardiac functional and stain analysis were performed using CVI42 software including LVEF, CO, CI, EDV/BSA, ESV/BSA, and SV/BSA. The presence of focal myocardial oedema on T2 STIR and non-ischemic lesions on LGE images was visually assessed by consensus agreement by the two readers. For strain analysis, longitudinal strain and strain rate values were derived from four-chamber, three-chamber and two-chamber view cine images. Circumferential and radial strain rate measurements were derived from the basal, mid-ventricular, and apical sections of short axis cine images.
4. Statistical analysis. Statistical analysis was performed using SPSS Statistics 27.0. Parameters are presented as mean±standard deviation or as absolute frequency. The independent two-sample Student t test was used for comparison if data comply with normal distribution. While Mann-Whitney U test was used for comparison if data does not conform to normal distribution.
RESULTS
A total of 52 subjects were included in this study (26 patients with myocarditis and 26 controls). Age, sex, and BMI did not differ significantly. Among the 26 myocarditis patients, 2 cases were confirmed by endocardial biopsy and 24 cases were confirmed by clinical data. Clinical characteristics were given in Table 1. Distribution of malignancies is shown in Table 2. The proportion of patients with normal LVEF (≥50%) was 88.5% (23/26). The incidence rate of myocardial edema was 30.8% (8/26) and the incidence rate of LGE was 42.3% (11/26). Data on LGE included its localization (septal, inferior, lateral, or anterior), and pattern (subepicardial, subendocardial, midwall, or transmural) was shown in Table 3. For LVEF, CO, CI, EDV/BSA, ESV/BSA, and SV/BSA between the two groups (Table 4), LVEF and ESV/BSA were significantly different in the myocarditis group compared to the control group: LVEF (P=0.018), ESV/BSA (P=0.048). For strain analysis (Table 5), LS_Basal showed no obvious different (P=0.206), while LS_Mid, LS_Apical and LS_Global reduced significantly in patient with ICI when compared with healthy group (P=0.002, 0.001, 0.002). All the peak systolic circumferential strain analysis (CS_Global , CS_Basal, CS_Mid, CS_Apical) were significantly lower (P=0.045, 0.006, 0.007, 0.006). But there were no significantly different between these two groups in radial direction (all P>0.05).DISCUSSION
The location with a higher proportion of LGE was at the basal wall which are similar with previous literatures6,7. Relatively low occurrence rate of high signal in T2 STIR and LGE suggest caution in reliance on the Lake Louise criteria based on LGE and T2-STIR for the exclusion of ICI-associated myocarditis. In our study, reduced LVEF and increased left ventricular end-systolic volume indicate of impaired cardiac systolic function due to the myocardial injury. Only a few studies have focused on the cardiac strain analysis in patients with ICI-associated myocarditis. Our results were similar to those of previous studies which CS and LS parameters can be more valuable than RS parameters5,8. For segmental strain, there were difference between the 2 groups for CS_Basal, CS_Mid, CS_Apical, LS_Mid, LS_Apical. This indicates the reduction in CS and LS is not partial.CONCLUSION
For patients with ICI-associated myocarditis, LVEF, ESV/BSA, peak systolic circumferential strain (basal, mid, apical and global) and peak systolic longitudinal strain (mid, apical and global) may be effective parameters to identify myocardial injury.Acknowledgements
No acknowledgement found.References
1. Brown TJ, Mamtani R, Bange EM. Immunotherapy Adverse Effects. JAMA Oncol. 2021;7(12):1908.
2. Addison D, Neilan TG, Barac A, et al. Cardiovascular Imaging in Contemporary Cardio-Oncology: A Scientific Statement From the American Heart Association. Circulation. 2023;148(16):1271-1286.
3. Biersmith MA, Tong MS, Guha A, et al. Multimodality Cardiac Imaging in the Era of Emerging Cancer Therapies. J Am Heart Assoc. 2020;9(2):e013755.
4. Friedrich MG, Sechtem U, Schulz-Menger J, et al. Cardiovascular magnetic resonance in myocarditis: A JACC White Paper. J Am Coll Cardiol. 2009;53(17):1475-1487.
5. Luetkens JA, Schlesinger-Irsch U, Kuetting DL, et al. Feature-tracking myocardial strain analysis in acute myocarditis: diagnostic value and association with myocardial oedema. Eur Radiol. 2017;27(11):4661-4671.
6. Cadour F, Cautela J, Rapacchi S, et al. Cardiac MRI Features and Prognostic Value in Immune Checkpoint Inhibitor-induced Myocarditis. Radiology. 2022;303(3):512-521.
7. Zhang L, Awadalla M, Mahmood SS, et al. Cardiovascular magnetic resonance in immune checkpoint inhibitor-associated myocarditis. Eur Heart J. 2020;41(18):1733-1743.
8. Awadalla M, Mahmood SS, Groarke JD, et al. Global Longitudinal Strain and Cardiac Events in Patients With Immune Checkpoint Inhibitor-Related Myocarditis. J Am Coll Cardiol. 2020;75(5):467-478.
Figures
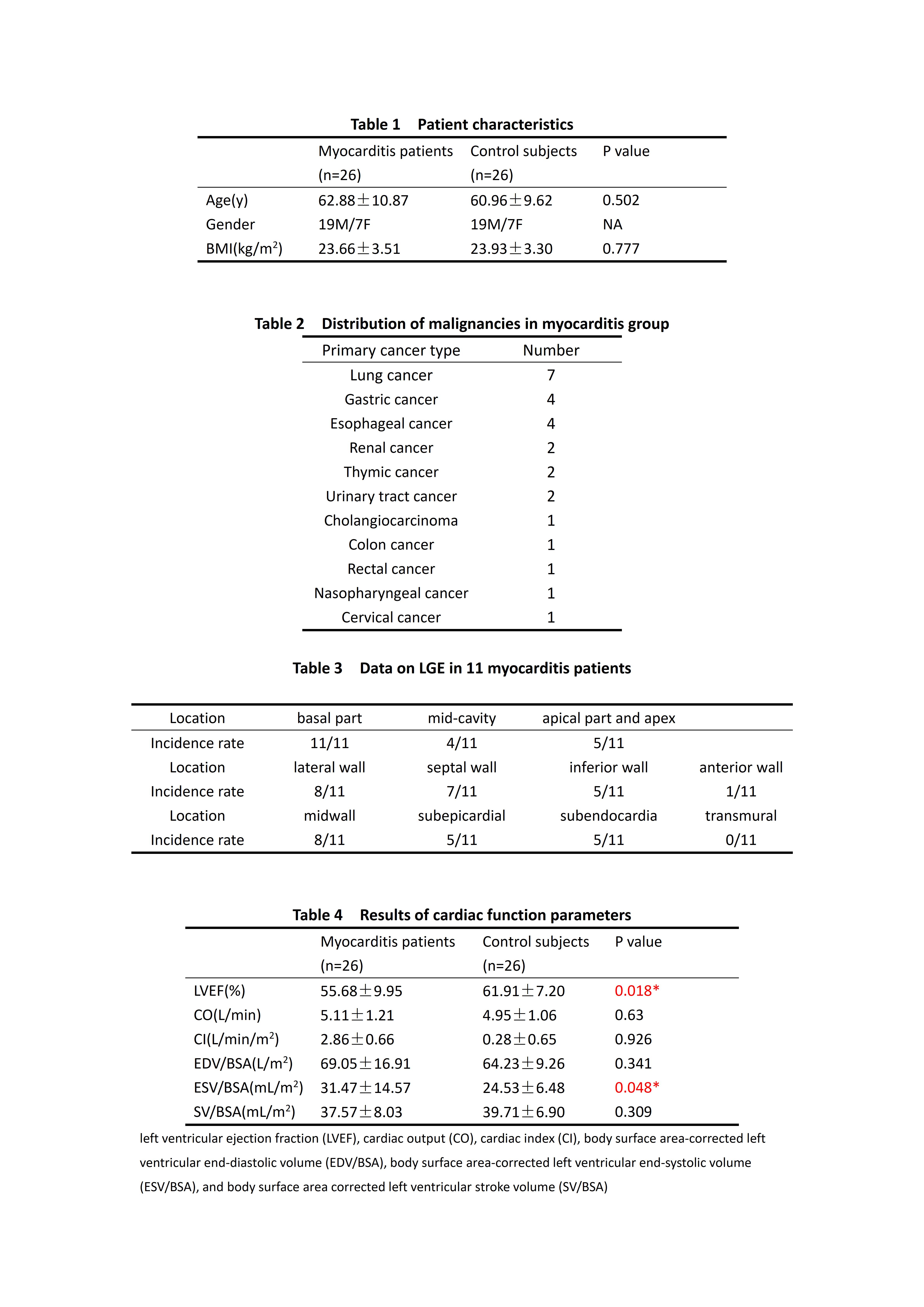
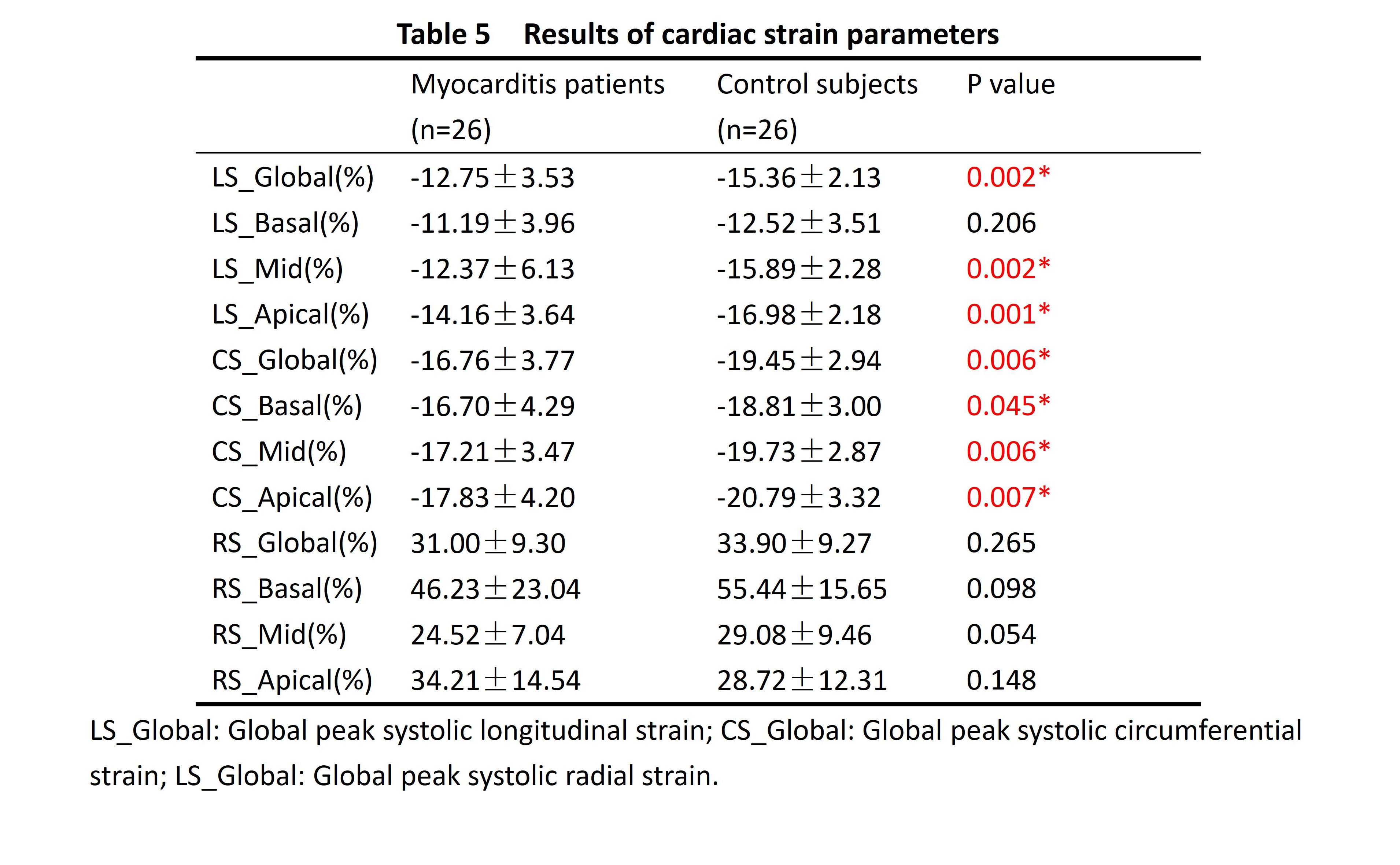
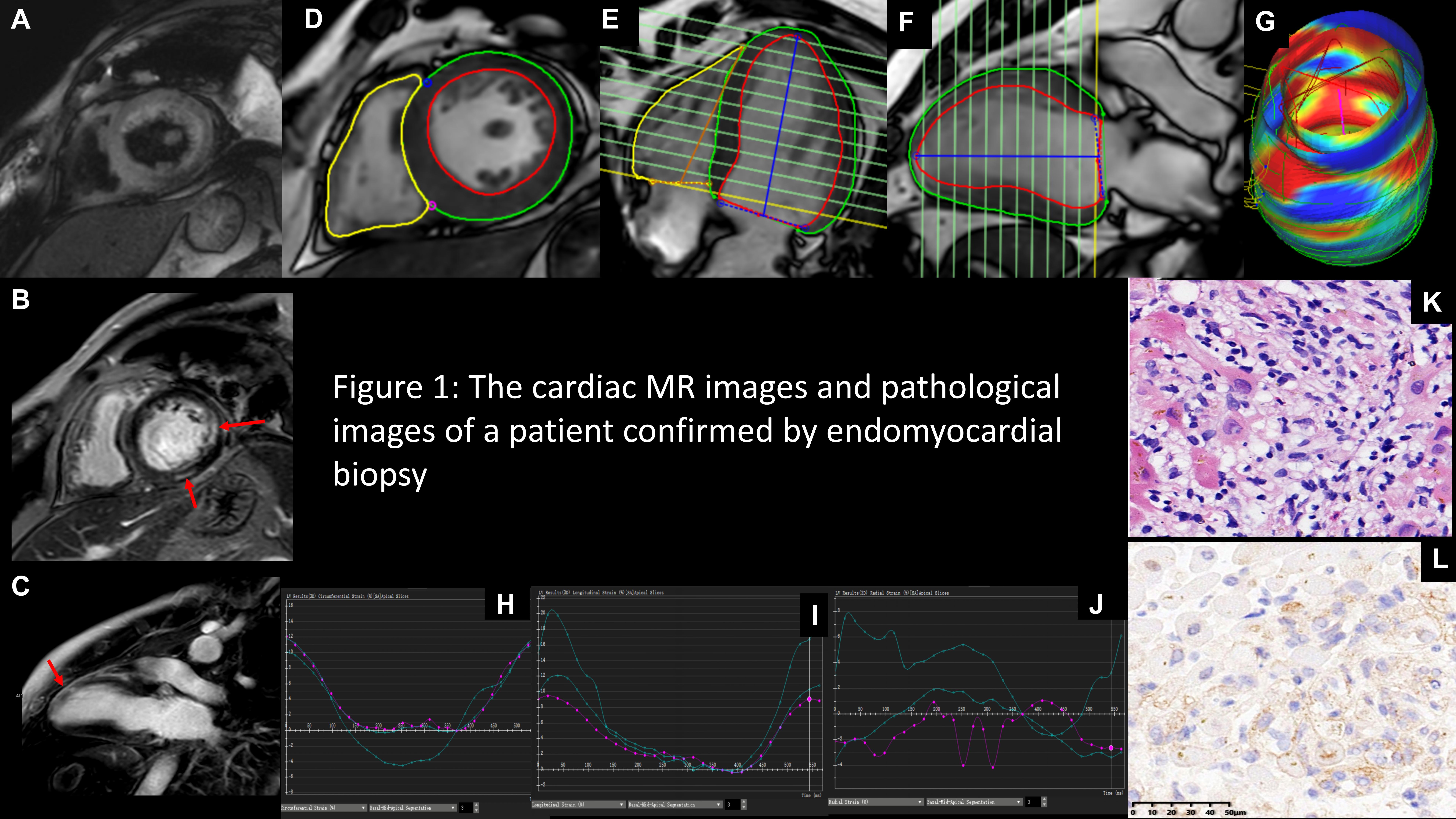
Figure 1: A: Left ventricular short axis T2 STIR image: no obvious signs of edema. B-C: Left ventricular short and long axis LGE image: Multiple patchy delayed enhancement can be seen in the myocardium. D-F: Cine images in short axis, four-chamber and two-chamber views for FT strain analysis. G: A 3D image containing strain information. H-J: CS, LS and RS curves in different parts (Basal, Mid, Apical). K-L: Pathological section by endomyocardial biopsy confirmed the diagnosis of ICI associated myocarditis.