3526
A 5D MRI Framework for Cardiac Motion Characterization in Radiation Therapy1Medical Physics, University of Wisconsin-Madison, Madison, WI, United States, 2Human Oncology, University of Wisconsin-Madison, Madison, WI, United States, 3Radiology, University of Wisconsin-Madison, Madison, WI, United States
Synopsis
Keywords: Hematology, Oncology, Radiotherapy, 5D, cardiac
Motivation: Current radiotherapy treatment planning does not account for cardiac substructure motion during the respiratory and cardiac cycle, thus leading to suboptimal treatment plans.
Goal(s): To develop a free breathing 5D MRI framework to characterize cardiac and respiratory motion of the heart for use in radiotherapy treatment planning.
Approach: A double gated (cardiac and respiratory) radial bSSFP acquisition and constrained reconstruction pipeline were implemented and motion and tested in five volunteers.
Results: Left ventricle centroid analysis showed 5D images provided significant motion characterization. Advanced reconstruction allows <5 min scan time.
Impact: The primary impact of this work will be on patients receiving thoracic radiotherapy. More accurate treatment planning and sparing of sensitive cardiac substructures will improve patient outcomes and reduce long term cardiotoxicities.
Introduction
Thoracic treatment plans in radiotherapy are based on mean dose delivered to the whole heart and do not account for cardiac substructures which may be affected differently1. In the long term, it can lead to radiation-induced cardiotoxicities such as congestive heart failure and myocardial infarction2. Typically, thoracic radiation therapy planning is based on Computed Tomography which has high spatial resolution but significantly reduced ability to visualize cardiac substructures. MRI has superior soft tissue contrast and thus is a promising modality for improved cardiac treatment planning. However, cardiac imaging is complicated by both cardiac and respiratory motion. Thus, accurate treatment planning needs to account for complex movement of the heart. To that end, we propose a 5D (3 spatial and 2 temporal) framework for whole-heart imaging that allows for accurate motion characterization throughout the cardiac cycle (CC) and respiratory cycle (RC).Methods
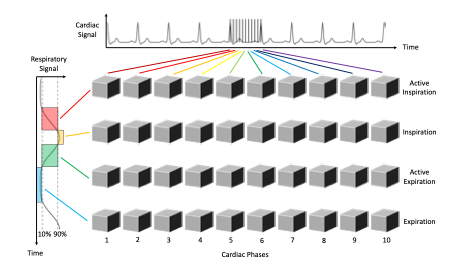
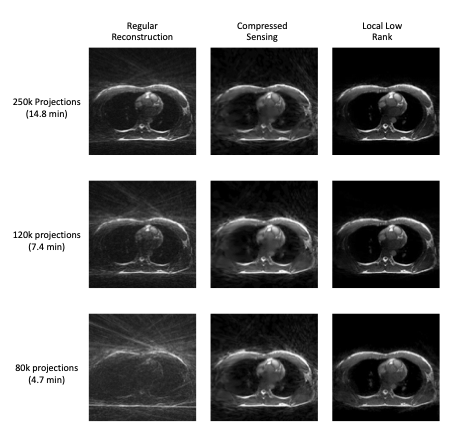
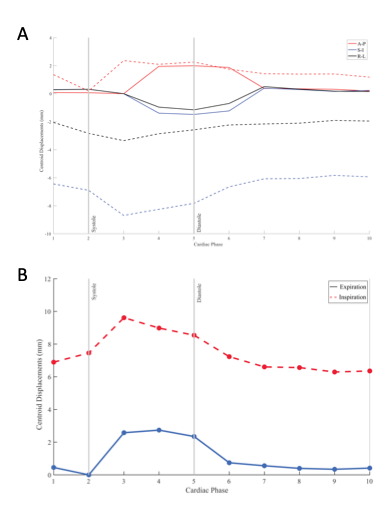
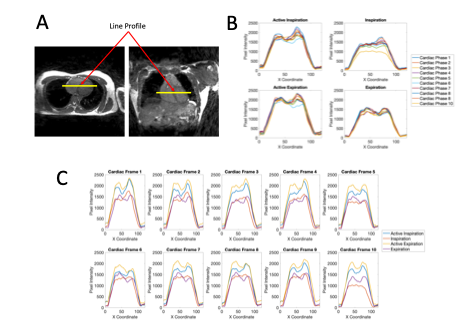
The primary component of the proposed 5D MRI framework is a highly undersampled 3D radial balanced Steady State Free Precession (bSSFP) sequence chosen for its superior blood to tissue contrast and flexible retrospective gating capabilities3. Radial projections were acquired in a 2D bit reversed view ordering to provide motion robustness and even spacing of projections4. Fractional echo readouts (80%) were utilized to further accelerate the acquisition. Cardiac and respiratory signals were recorded using a pulse oximeter (PPG) and respiration bellows respectively. Five healthy volunteers (age=22-26y) were scanned on a 1.5 T clinical system (SIGNA Artist, GE Healthcare, WI) using a 30-channel chest coil. Scan parameters include:TR/TE=3.4/0.9ms; flip=35°;image volume=(40cm)3;spatial resolution=(1.56mm)3 isotropic;# of projections=250,000;scan time=14min. Images were reconstructed offline using algorithms that support dual gating by binning projections according to their time stamp in the CC and RC5 (Figure 1). Cardiac phases were determined by calculating the mean RR interval of the PPG signal and dividing projections into 10 bins. Respiratory gating was performed using a 5 second sliding window threshold to divide the bellows waveform into four different phases: inspiration (top 10%), expiration (bottom 10%), active inspiration (middle 80%-upslope), and active expiration (80%-downslope). The acquisition and reconstruction framework also allowed for retrospective subsampling of the acquired projections to simulate a shorter scan time. Scan times of approximately 5 and 7 min were simulated and compared for image quality. Due to the high undersampling factor, iterative constrained reconstruction techniques were employed to improve image quality and remove undersampling artifacts. Standard reconstructions were compared against compressed sensing and a local low rank approach6. For quantitative analysis, motion was characterized in expiration and inspiration for a single case by segmenting the left ventricle (LV) through all 10 cardiac phases for each respiratory phase in treatment planning software (MIM Maestro). Centroids of the LV were calculated and displacements from a reference point in end systole, end-expiration were calculated. Additionally, a pixel intensity profile analysis was performed in a separate subject by measuring the change in pixel intensity across the CC and RC in a line segment crossing the center of the interventricular septum. Generated profiles were smoothed with a Gaussian filter to remove noise.Results
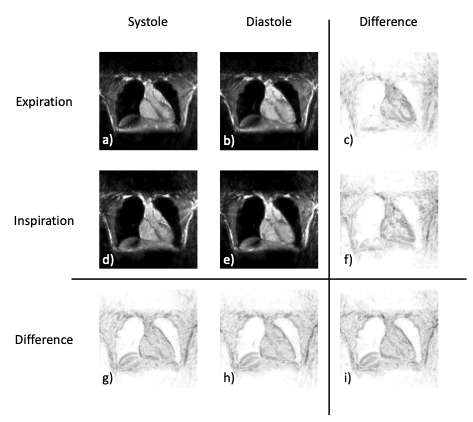
Figure 2 shows representative 5D images in systole, diastole, expiration, and inspiration. Images reconstructed from 3 different numbers of projections and 3 reconstruction techniques are compared in Figure 3 with the local low rank reconstruction proving to be the most robust, especially at lower scan times. Figure 4 shows the displacement of the LV centroid throughout the CC and RC. Figures 5B and 5C show the changes in pixel intensity across the RC and CC respectively. The dip in the plateau of the pixel intensity corresponds to the interventricular septum and illustrates its motion in the R-L direction.Discussion
With the proposed 5D MRI framework, we were able to successfully provide 3D volumetric images of the heart throughout the cardiac and respiratory cycles. The capabilities to track motion of cardiac structures was demonstrated for LV centroids and septal line profiles. While the initial scan duration was long, subsampling experiments demonstrated that shortening scan time to <5 min and using a local low rank reconstruction produces images of similar quality. Tissue contrast was satisfactory for large structure segmentation but limited in depicting finer structures such as the coronary arteries.Conclusion
This study demonstrates the feasibility of motion characterization of the heart through the cardiac and respiratory cycles using a 5-minute 5D radial bSSFP acquisition. The framework is an important first step for improved radiotherapy treatment planning in the thorax, especially for advanced image-guided therapy machines like MR-Linacs. Future work will include improving the visibility of cardiac substructures, self-gating, and quantitative motion validation.Acknowledgements
The authors wish to acknowledge the NIH (R01HL153720) for supporting this study, as well as GE Healthcare which provides research support to the University of Wisconsin.References
1. Siaravas KC, Katsouras CS, Sioka C. Radiation Treatment Mechanisms of Cardiotoxicity: A Systematic Review. Int J Mol Sci. 2023 Mar 27;24(7):6272. doi: 10.3390/ijms24076272. PMID: 37047245; PMCID: PMC10094086.
2. Morris ED, Aldridge K, Ghanem AI, Zhu S, Glide-Hurst CK. Incorporating sensitive cardiac substructure sparing into radiation therapy planning. 2020 J. Appl. Clin. Med. Phys., 21: 195-204. https://doi.org/10.1002/acm2.13037
3. Barger AV, Block WF, Toropov Y, Grist TM, Mistretta CA. Time-resolved contrast-enhanced imaging with isotropic resolution and broad coverage using an undersampled 3D projection trajectory. Magn Reson Med. 2002 Aug;48(2):297-305. doi: 10.1002/mrm.10212. PMID: 12210938.
4. Chan RW, Ramsay EA, Cheung EY, Plewes DB. (2012), The influence of radial undersampling schemes on compressed sensing reconstruction in breast MRI. Magn. Reson. Med., 67: 363-377. https://doi.org/10.1002/mrm.23008
5. Schrauben EM, Anderson AG, Johnson KM, Wieben O. Respiratory-induced venous blood flow effects using flexible retrospective double-gating. J Magn Reson Imaging. 2015 Jul;42(1):211-6. doi: 10.1002/jmri.24746. Epub 2014 Sep 11. PMID: 25210850.
6. Lustig M, Donoho DL, Santos JM, Pauly JM, "Compressed Sensing MRI," in IEEE Signal Processing Magazine, vol. 25, no. 2, pp. 72-82, March 2008, doi: 10.1109/MSP.2007.914728.
Figures