3524
Multiparametric Cardiovascular MR in Non-hospitalized COVID-19 Infection Subjects: An Intra-individual Comparison Study1Diagnostic Radiology, Jinling Hospital, Medical School of Nanjing University, Nanjing, China, 2MR Research, GE Healthcare, Bei Jing, China
Synopsis
Keywords: Inflammation, Infiltration, Heart
Motivation: To evaluate the prevalence of cardiac involvement in mild, non-hospitalized, recovered COVID-19 patients
Goal(s): investigate the changes of cardiac structure and function by comparing multiparametrical cardiac MR
Approach: This prospective study enrolled 39 unhospitalized COVID-19 patients.
Results: Four patients had the same late gadolinium enhancement (LGE) pattern at baseline and repeated CMR and 5 female patients had myocardial T2 ratio >2 but with normal T2 value in post-COVID-19 CMR. All other CMR parameters were in normal ranges before and after COVID-19 infection.
Impact: This knowledge has an important role in can help alleviate wide social concern on COVID-19 related myocarditis.
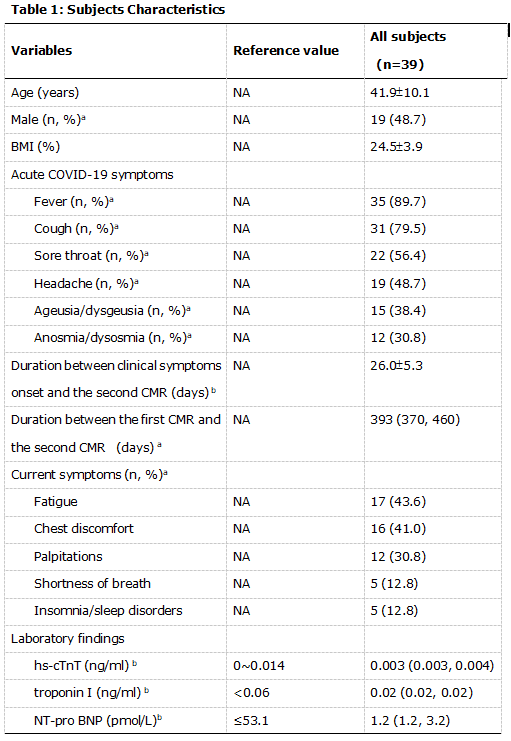
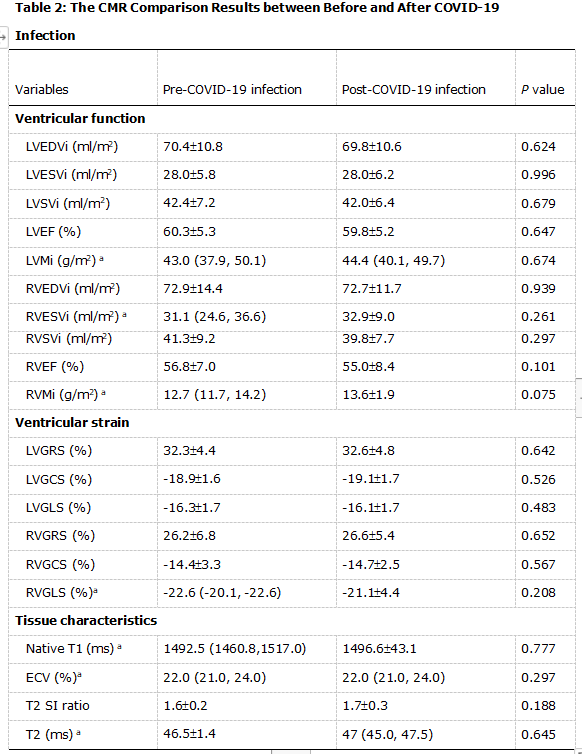
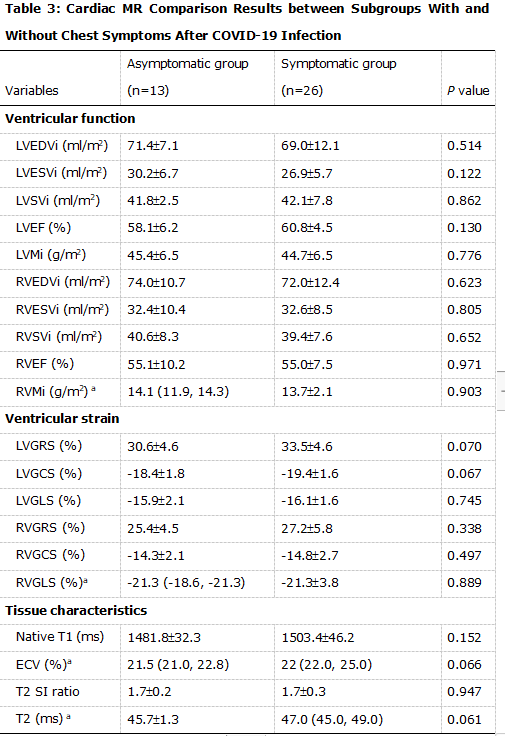
MethodsAll volunteers have no history of COVID-19 infection demonstrated by polymerase chain reaction (PCR) tests 2-4 times each month from 2021 to 2022. 39 volunteers mentioned above who infected with COVID-19 confirmed by PCR or antigen detection in December 2022 were willing to participate repeated cardiac MR examination. Inclusion criteria were: no history of COVID-19 infection, COVID-19 infection confirmed by PCR or antigen detection before the second cardiac MR examination. Exclusion criteria were: contraindications to cardiac MR, image data loss of the first cardiac MR examination, inadequate image quality of cardiac MR examinations for cardiac MR analysis owing to artifacts.This study was approved by the institutional review board of our hospital and written informed consent was obtained from all the participants.All participants underwent baseline and follow-up cardiac MR examinations on the same 3-Tesla scanner (GE Healthcare) . The cardiac MR scanning protocols consisted of: 1) 2-chamber, 3-chamber, 4-chamber and short-axis cine imaging 2) black blood T2-weight imaging 3) native T1 and T2 mapping 4) post-contrast T1 mapping 5) late gadolinium enhancement (LGE) imaging. LGE imaging was performed 10-15 mins after intravenous administration of gadolinium-based contrast agent (Beilu Pharmaceutical, Beijing, China) using a myocardial delayed enhancement sequence in long-axis and short-axis views. All cardiac MR images were analyzed with CVI 42 software (Canada) by an experienced cardiovascular radiologist with 12 years of experience in cardiac MR was blinded to the participants’ clinical manifestation and laboratory profiles. Myocardial edema was assessed by calculated the ratio between myocardial signal intensity (SI) to skeletal muscle SI. Left ventricle (LV) and right ventricle (RV) functional parameters were automatically calculated after drawing endocardial and epicardial contours. In the end-diastolic frame, automatically tracked throughout the cardiac cycle to obtain biventricular strain parameters, including global radial peak strain (GRS), global circumferential peak strain (GCS), and global longitudinal strain (GLS). Statistical analysis were performed using SPSS version 23.0 (SPSS Inc. USA). Continuous variables were reported as means and standard deviations when they were normally distributed and expressed as medians and interquartile ranges when they were non-normally distributed. Paired group comparisons were performed using the paired samples t-test or the Wilcoxon Signed Rank test for parametric and non-parametric data, respectively. T-test and Mann-Whitney U test were used to compare the means with normal distribution and non-normal distribution, respectively. P<0.05 was regarded as the level for statistical significance.ResultsPatients’ characteristics and blood test results are shown in Table 1. The comparisons of cardiac MR results between before and after COVID-19 infection are presented in Table 2. All the cardiac MR parameters including cardiac structure, function, native T1, native T2 and ECV were not significantly different between before and after COVID-19 infection (Figure 1). LGE was minimally detectable in 4 participants in both pre- and post-COVID-19 infection cardiac MR scans with the same location and pattern. The cardiac MR results after COVID-19 infection between symptomatic group and asymptomatic group (Table 3). DiscussionTo This intra-individual cardiac MR comparison study demonstrated that in non-hospitalized COVID-19 patients with normal myocardial enzyme, the cardiac structure and function after COVID-19 infection are similar to those before COVID-19 infection, no matter with or without mild symptoms, which indicated no measurable myocardial injury in these patients. This can alleviate wide social concern on COVID-19 infection related myocarditis. More importantly, it is relevant to diagnose COVID-19 infection related myocardial injury by combining multiple cardiac MR parameters and clinical measures and compare with historical cardiac MR images, which may reduce misdiagnosis.ConclusionIn conclusion, our intra-individual comparison multipara metric cardiac MR study demonstrated that mild non-hospitalized COVID-19 participants had no measurable cardiac structure and function abnormalities on cardiac MR.
Acknowledgements
NoReferences
1. Shi S, Qin M, Shen B, et al (2020) Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA Cardiol 5:802-810.
2. Rudski L, Januzzi JL, Rigolin VH, et al (2020) Multimodality imaging in evaluation of cardiovascular complications in patients with COVID-19: JACC scientific expert panel. J Am Coll Cardiol 76:1345-1357. 3. Phelan D, Kim JH, Elliott MD, et al (2020) Screening of potential cardiac involvement in competitive athletes recovering from COVID-19: An expert consensus statement. JACC Cardiovasc Imaging 13:2635-2652.
4. Task Force for the management of COVID-19 of the European Society of Cardiology (2022) ESC guidance for the diagnosis and management of cardiovascular disease during the COVID-19 pandemic: part 2-care pathways, treatment, and follow-up. Cardiovasc Res 118:1618-1666.
5. Puntmann VO, Carerj ML, Wieters I, et al (2020) Outcomes of cardiovascular magnetic resonance imaging in patients recently recovered from coronavirus disease 2019 (COVID-19). JAMA Cardiol 5:1265-1273.
6. Erdol MA, Ozbay MB, Yayla C, et al (2021) Cardiac involvement in MRI in young population after COVID-19: A single tertiary center experience. Echocardiography 38:1327-1335.
7. Çakmak Karaaslan Ö, Özilhan MO, Maden O, Tüfekçioğlu O (2022) Prevalence of cardiac involvement in home-based recovered coronavirus disease 2019 (COVID-19) patients: a retrospective observational study. Ir J Med Sci 191:2057-2062.
8. Kawel-Boehm N, Hetzel SJ, Ambale-Venkatesh B, et al (2020) Reference ranges ("normal values") for cardiovascular magnetic resonance (CMR) in adults and children: 2020 update. J Cardiovasc Magn Reson 22:87.
9. Berry C, Mangion K (2021) Cardiovascular complications are uncommon in healthcare workers with mild or asymptomatic COVID-19 Infection. JACC Cardiovasc Imaging 14:2167-2169.
Figures
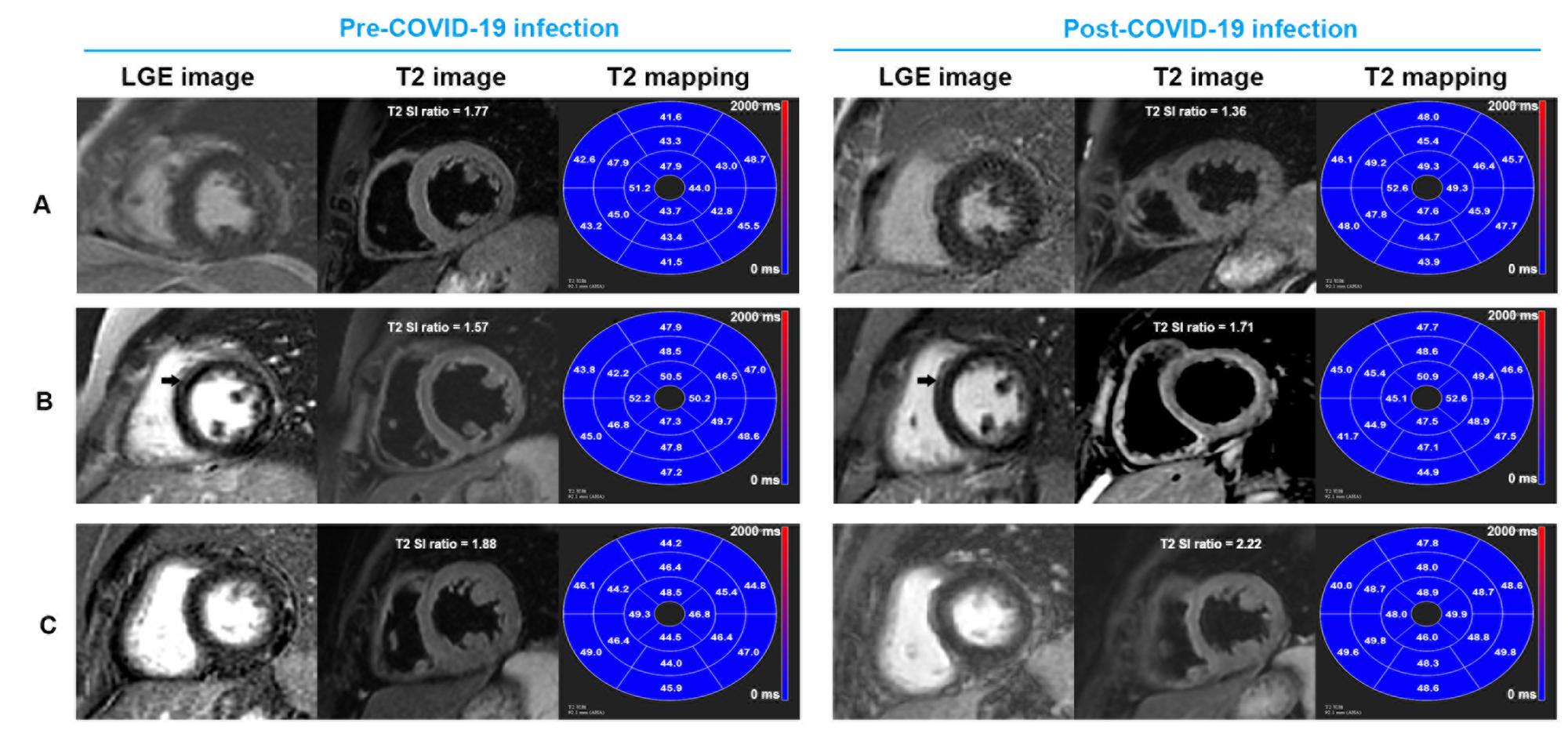
A, A 52-year-old man. He had normal LGE image, black blood T2 weight image and T2 values before COVID-19 infection and at 27 days after COVID-19 infection
B, A 30-year-old woman. Subepicardial LGE (arrow) was found in the septal segments of left ventricle in both before COVID-19 infection and at 31 days after COVID-19 infection. The T2 SI ratio and native T2 value were in normal range.
C, A 59-year-old woman. He had normal LGE and negative native T2 value (49 ms) but elevated T2 SI ratio (2.22) at 31 days after COVID-19 infection.