3523
Using cardiac MRI quantification in identifying subtle cardiac structural and functional changes in patients with liver cirrhosis.1Second Clinical Medical College of Guangzhou University of Traditional Chinese Medicine, Guangzhou,China, China, 2Department of Radiology, The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, Guangdong, Guangzhou, China, China, 3MR Research Collaboration, Siemens Healthineers, Guangzhou, China, Guangzhou, China, China
Synopsis
Keywords: Inflammation, Infiltration, Quantitative Imaging
Motivation: Patients with liver cirrhosis often have heart-related physiological and pathological changes.
Goal(s): The aim of this study is to investigate the effectiveness of using multiple parameters for cardiac MRI quantification in identifying subtle cardiac structural and functional changes in patients with liver cirrhosis.
Approach: Cardiac MRI methods were employed, along with Mann-Whitney U tests and Spearman correlation analyses for Statistical analyses.
Results: Our results indicated that MRI showed an increase in myocardial fibrosis parameters, and there was a positive correlation between liver T1 relaxation time and myocardial T1 relaxation time.
Impact: This study could lead to improved understanding of heart diseases associated with cirrhosis, helping to create better diagnostic and treatment plans, ultimately improving patients' quality of life.
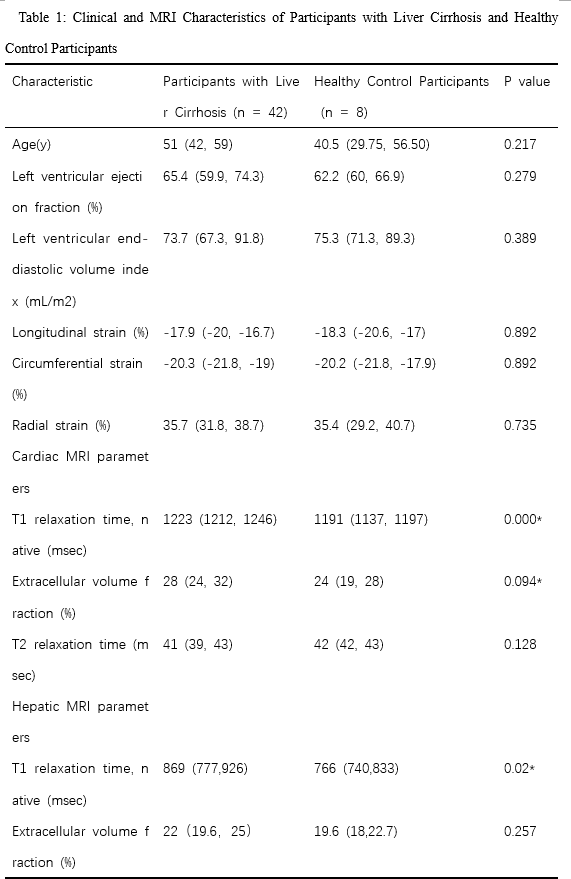
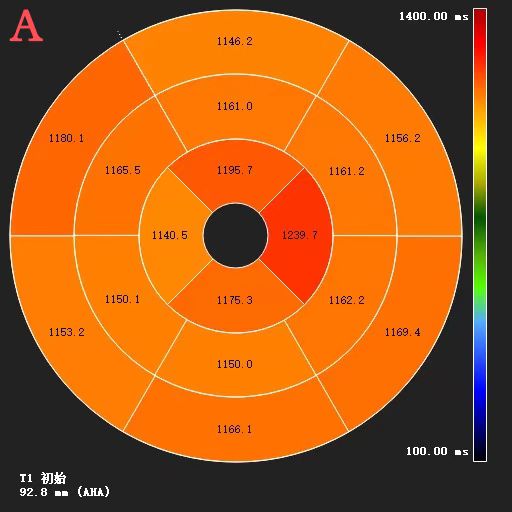
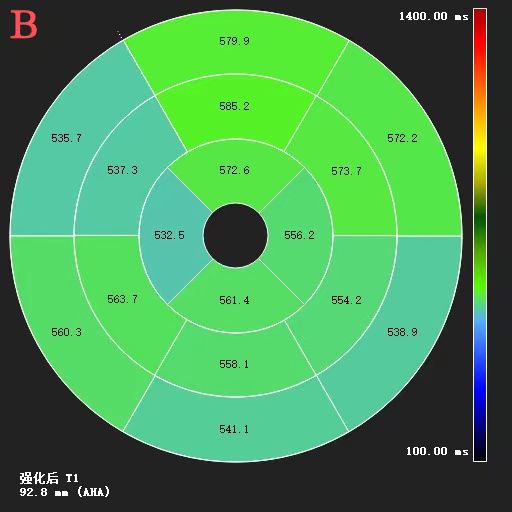
Methods: A total of 50 cirrhosis patients (median age: 49.5 years old; interquartile range:42.3-50; 26 men) were enrolled in this study including 42 patients with Liver Cirrhosis and 8 patients with Healthy Control Participants. Combined cardiac and hepatic examinations were performed during a single scan for each participant with a clinical whole-body 3T system (MAGNETOM Prisma, Siemens Healthineers, Erlangen, Germany) with an 18-channel body coil. Cardiac scan protocol included electrocardiogram-gated steady-state free-precession cine images (short-axis, four chamber, and two-chamber views). Average left ventricular longitudinal, circumferential, and radial strain values were assessed. Myocardial T1 and T2 mapping were obtained in end-diastole in apical, midventricular, and basal short-axis orientation. The acquisition parameters of Myocardial T1 mapping were as following: voxel size = 1.4x1.4x10 mm3, TE/TR= 1.12/279.48 ms; flip angle=35 deg; slice thickness=10mm, free-breathing scanning. All Myocardial mapping images were reconstructed in CVI 4.2 software (Circle, Calgary, Ontario, Canada). The T1, ECV and T2 mapping values of each segment were measured on basal, middle and apical short axis sections according to the American Heart Association 17-segment model (excluding apical). (Figure 1). Myocardial and hepatic T1 maps were acquired 10 and 12 minutes after contrast material injection, respectively. The mean of the six ROl measurements was the patient's liver T1 mapping. The hematocrit level was evaluated directly before MRI scanning to calculate the ECV[7]. Cardiac quantitative magnetic resonance parameters and hepatic mapping parameters were compared by Mann-Whitney U-test between Participants with Liver Cirrhosis groups and Healthy Control Participants groups. Spearman correlation analysis was used to test correlations between continuous variables. The level of statistical significance was set to P<0.05.
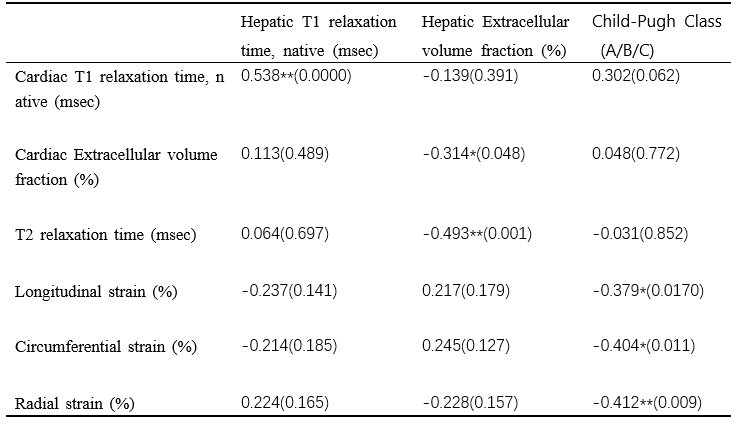
Results: Mann-Whitney U test indicated that precontrast liver mapping, precontrast Myocardial mapping and myocardial extracellular volume had significant difference between these two groups (Table 1). Correlation analysis showed that Myocardial T1 relaxation times (r = 0.538, P < 0.001) were all moderately positive correlated with precontrast liver T1 mapping. There were Negative correlations between Myocardial T1 relaxation times and hepatic ECV (r = -0.493, P = 0.001). hepatic ECV correlated with myocardial ECV (r = -0.314, P = 0.048) (Table 2). Discussion: Our study used heart and liver MRI to reveal signs of myocardial focal and diffuse myocardial fibrosis, supporting subclinical myocardial histopathological changes in patients with advanced liver disease. Myocardial T1 mapping in patients with liver cirrhosis was significantly increased (1223 msec vs 1191 msec; P<0.001). Our results are consistent with previous cardiac MRI studies that myocardial fibrosis may play an important role in the development of CCM. Correlation analysis showed that Myocardial T1 relaxation times were all moderatly positive correlated with precontrast liver T1 mapping (r=0.538,P<0.001)、Child-Pugh Class (A/B/C) (r=0.302 ,P=0.062). It is suggested that there is a relationship between the clinical grade of liver disease and cardiac fibrosis and inflammation. Myocardial fibrosis in patients with liver cirrhosis may be caused not only by high cardiac load, but also by liver-related mechanisms.In our study, there was no significant change in myocardial ECV in patients with liver cirrhosis (p=0.094). On the contrary, Lee et al reported a pattern of greater myocardial ECV in 32 patients with liver cirrhosis that decreased 1 year after transplantation[8]. The main reason is our sample size was small, so additional confirmatory analyses are needed before the results of this exploratory study can be generalized.
Acknowledgements
We sincerely thank to all the participants in this studyReferences
- Leal-Alvarado T M, Escalante-Sandoval I, Gálvez-Romero J L, et al. Physiopathological and diagnostic aspects of cirrhotic cardiomyopathy[J]. Archivos de cardiología de México, 2020, 90(2): 154-162.
- Myers R P, Lee S S. Cirrhotic cardiomyopathy and liver
transplantation[J]. Liver Transplantation, 2000, 6(S1 S1): S44-S52.
- Izzy M, VanWagner L B, Lin G, et al. Redefining cirrhotic cardiomyopathy for the modern era[J]. Hepatology, 2020, 71(1): 334-345.
- Francque S M, Van Der Graaff D, Kwanten W J. Non-alcoholic fatty liver disease and cardiovascular risk: Pathophysiological mechanisms and implications[J]. Journal of hepatology, 2016, 65(2): 425-443.
- Myers R P, Lee S S. Cirrhotic cardiomyopathy and liver transplantation[J]. Liver Transplantation, 2000, 6(S1 S1): S44-S52.
- Messroghli D R, Moon J C, Ferreira V M, et al. Clinical recommendations for cardiovascular magnetic resonance map** of T1, T2, T2* and extracellular volume: a consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI)[J]. Journal of Cardiovascular Magnetic Resonance, 2017, 19(1): 1-24.
- Isaak A, Praktiknjo M, Jansen C, et al. Myocardial fibrosis and inflammation in liver cirrhosis: MRI study of the liver-heart axis[J]. Radiology, 2020, 297(1): 51-61.
- Lee YB, Lee J-H. Cirrhotic cardiomyopathy: an independent prognostic factor for cirrhotic patients. Clin Mol Hepatol 2018;24(4):372–373.
Figures