3519
Evaluating Subclinical Myocardial Injury in Systemic Lupus Erythematosus Patients Using CMR Feature Tracking1Longyan First Hospital Affiliated to Fujian Medical University, Longyan, China, 2Philips Healthcare, Shanghai, China, 3Philips Healthcare, Guangzhou, China
Synopsis
Keywords: Myocardium, Myocardium, SLE
Motivation: Early detection of myocardial injury in Systemic lupus erythematosus (SLE) patients is important.
Goal(s): Find a clinical biomarker for preclinical myocardial injury in SLE patients.
Approach: CMR-FT (Cardiac Magnetic Resonance Feature Tracking) technology and CVI 42 software were used to measure cardiac functional parameters and myocardial strain parameters for SLE patients with/without subclinical myocardial injury and healthy controls.
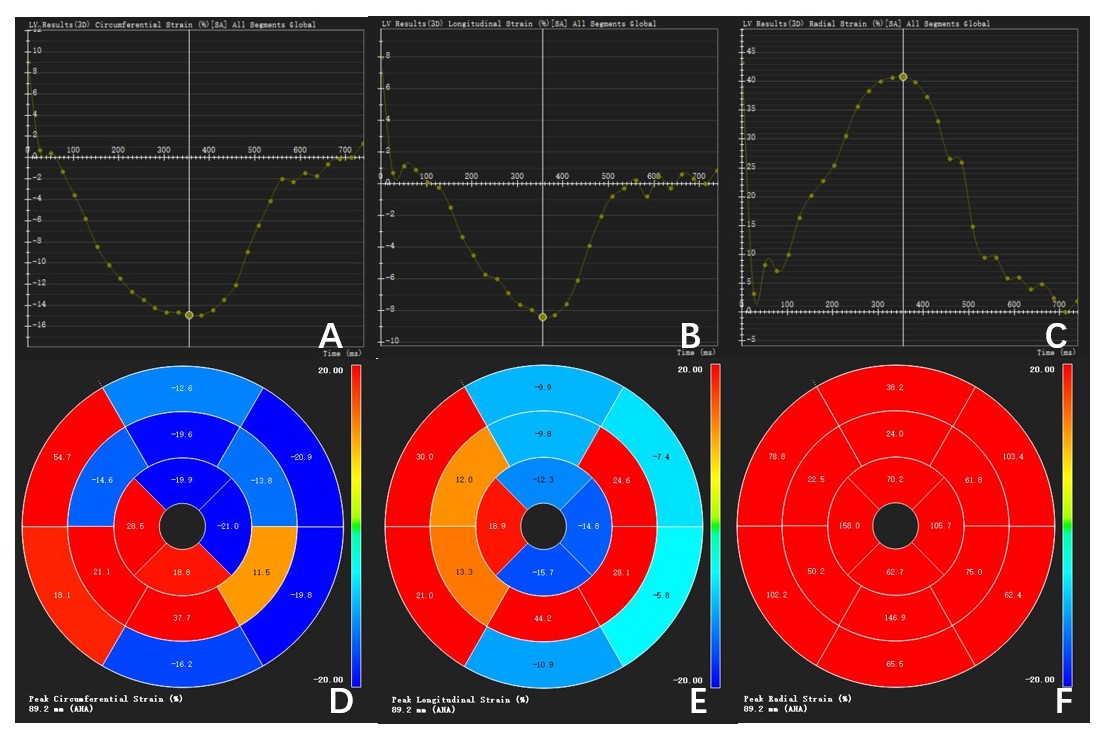
Results: Compared to the control group, the circumferential strain (CS) and longitudinal strain (LS) were found to be reduced in patients with subclinical myocardial injury in SLE. The CMR-FT technology was able to detect changes in myocardial strain before a decrease in ejection fraction occurred.
Impact: Early detection of myocardial injury in SLE patients and proactive treatment are important for improving patient outcomes. This study found that CMR-FT quantitative technique can identify subclinical myocardial damage in patients with SLE.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease that can affect multiple systems throughout the body [1]. In early autopsy studies, up to 80% of SLE patients were found to have myocarditis [2]. Another study revealed histological changes of myocarditis in 37% of deceased SLE patients, despite the absence of clinical manifestations of myocarditis [3].Myocardial fibrosis is a common cardiac manifestation in SLE patients, but clinical symptoms are often subtle. However, when severe myocarditis or refractory cardiomyopathy with heart failure occurs, the mortality rate is extremely high. Therefore, early detection of myocardial injury in SLE patients and proactive treatment are important for improving patient outcomes.
CMR-FT technology has shown high sensitivity and good consistency in identifying changes in cardiac function before a decrease in left ventricular ejection fraction (LVEF) occurs.
The aim of this study is to observe myocardial strain in patients with subclinical myocardial injury in SLE and investigate whether there are any detectable indicators that can suggest the occurrence of myocardial fibrosis.
Methods
This study prospectively included 33 clinically diagnosed SLE patients and 17 healthy control subjects.Philips Ingenia 3.0T MRI system with a 16-channel phased-array coil was used. Imaging sequences including short-axis, long-axis (2-chamber, 3-chamber, 4-chamber) cine, T1-weighted imaging , T2-weighted imaging with spectral attenuated inversion recovery (SPAIR), and late gadolinium enhancement (LGE). The specific parameters are summarized in Table 1. LGE was performed after bolus injection of gadopentetate dimeglumine at a dose of 0.1 mmol/kg and a flow rate of 4-5 ml/s via the elbow vein, followed by early and delayed enhancement short-axis scans at 2-3 minutes and 15 minutes, respectively, using an inversion recovery gradient echo sequence.
All images were imported into CVI 42 software. It can automatically identify end-diastole and end-systole and outline the endocardial and epicardial borders to calculate the required parameters (Table 2). The Strain module of the software was used to analyze myocardial strain, which automatically tracked displacement to quantify left ventricular myocardial motion, derived strain parameters are shown in Table 3.
Statistical analysis was performed using SPSS 23.0 software. Independent sample t-tests or chi-square tests were used for comparisons between two groups, while Kruskal-Wallis H test and Nemenyi test were used for comparisons among three groups. Pearson correlation analysis was conducted. P < 0.05 was considered as statistically significant.
Results
In the SLE subclinical myocardial damage group,the LVEDVI is higher than the healthy group,while the LVSVI is lower compared to the healthy group, with statistically significant differences (P = 0.03 and 0.04 respectively) (Table 2).There were remarkably differences in three groups for left ventricular CS and LS, as shown in Table 3. The peak diastolic circumferential strain rate (PCSR-D) and peak longitudinal strain rate (PLSR-D) are reduced in the SLE subclinical myocardial damage group compared to the control group, with statistically significant differences (P = 0.02 and 0.02 respectively), but there is no statistically significant difference compared to the SLE non-myocardial damage group (refer to Table 3).
Discussion
CMR-FT quantitative technique was utilized to evaluate the differences in left ventricular function between SLE patients and healthy individuals. Although the ejection fraction (EF)was normal and had no difference compared among the three groups, the LVEDVI and LVSVI were notable differences in SLE subclinical myocardial damage patients compared to the control group. This implies the possibility of impaired LV function in patients with SLE subclinical myocardial damage.Moreover, the CS and LS were lower in the subclinical myocardial damage group compared to the non-myocardial damage group and the healthy group. Additionally, the PCSR-D and PLSR-D were lower in the subclinical myocardial damage group compared to the healthy group, showing statistically significant differences. These findings are consistent with the results of previous studies conducted by Shen [4] and Zhang [5].
However, there were no significant differences in RS among the three groups. CMR-FT technique, by tracking myocardial strain in three directions, provides an objective reflection of both local and overall cardiac function [6].
Despite SLE patients having normal left and right ventricular EF, a reduction in left ventricular myocardial strain (CS, LS, PCSR-D, PLSR-D) has already been observed. This suggests that changes in myocardial strain may be detected earlier than changes in LVEF, indicating myocardial damage in SLE patients. These findings are consistent with previous research [7]. LVEF is influenced by volume and load conditions, which may not be sensitive enough to detect early left ventricular dysfunction.
Conclusion
The CMR-FT quantitative technique can identify subclinical myocardial damage in patients with SLE, and changes in circumferential strain (CS) and longitudinal strain (LS) are particularly helpful for diagnosis.Acknowledgements
This study was supported by Fujian Province Natural Science Foundation (Grant number 2021J011440).
References
[1]. Ercan, E., Magro-Checa, C., Valabregue, R., Branzoli, F., Wood, E. T., Steup-Beekman, G. M., et al. (2016). Glial and axonal changes in systemic lupus erythematosus measured with diffusion of intracellular metabolites. Brain, 139(5), 1447–1457. doi: 10.1093/brain/aww031. Epub 2016 Mar 11. PMID: 26969685; PMCID: PMC5006250.
[2]. Jain D and Halushka MK. Cardiac pathology of systemic lupus erythematosus. J Clin Pathol 2009; 62: 584–592.
[3]. Panchal L, Divate S, Vaideeswar P and Pandit SP. Cardiovascular involvement in systemic lupus erythematosus: an autopsy study of 27 patients in India. J Postgrad Med 2006; 52: 5–10; discussion 10.
[4]. Shen Jiayan, Feng Zehao, Wu Rui, Wu Lianming, Bu Jun, Jiang Meng. Correlation between myocardial strain and delayed myocardial reinforcement in systemic lupus erythematosus [J]. Chinese Journal of Medical Imaging, 2019,05:321-327.
[5]. Zhang Lisha, Yang Ruixue, Wang Lei, Gao Fabao. The value of diastolic peak strain rate based on cardiac magnetic resonance feature tracing imaging in hypertrophic cardiomyopathy with preserved ejection fraction and its relationship with cardiac troponin T [J]. Magnetic resonance imaging, 2022,12:45-50.
[6]. Augustine D, Lewandowski AJ, Lazdam M, et al. Global and regional left ventricular myocardial deformation measures by magnetic resonance feature tracking in healthy volunteers: comparison with tagging and relevance of gender[J]. J Cardiovasc Magn Reson, 2013,15(1):8-18.
[7]. Magne J, Cosyns B, Popescu BA, et al. Distribution and prognostic significance of left ventricular global longitudinal strain in asymptomatic significant aortic stenosis: an individual participant data Meta-analysis. JACC Cardiovasc Imaging, 2019, 12(1): 84-92.
Figures
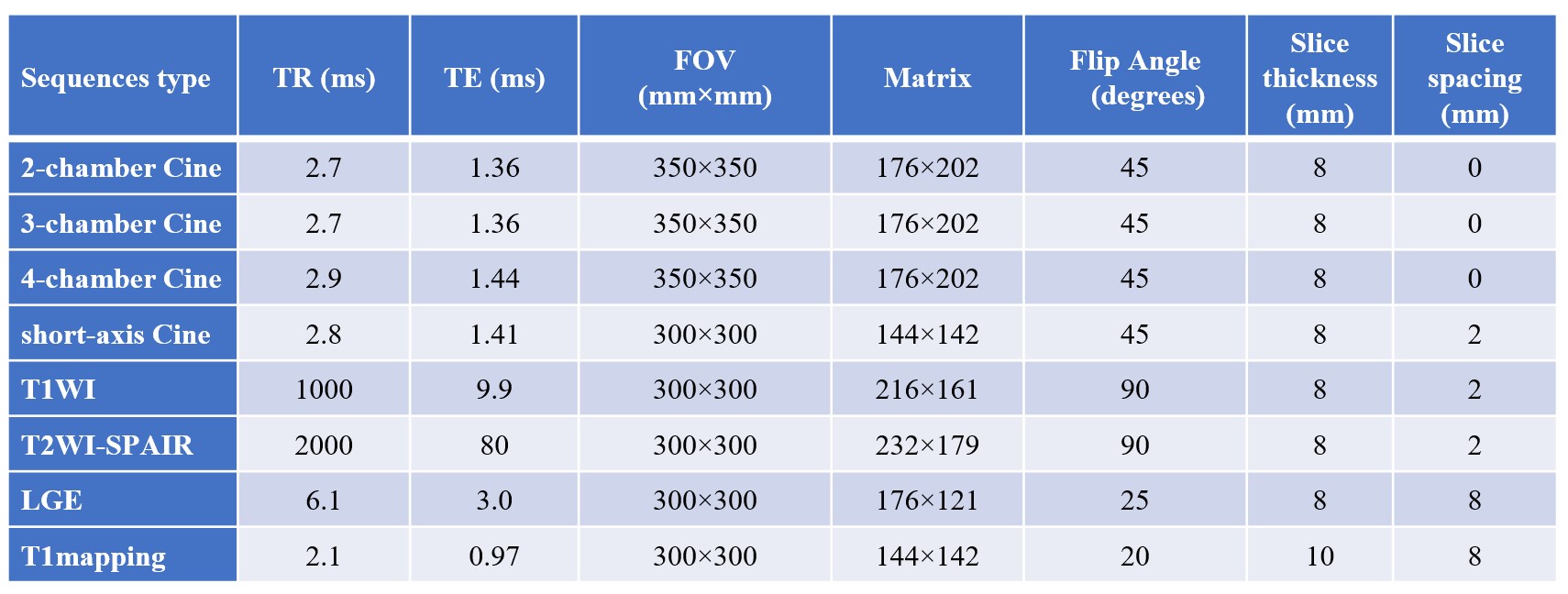
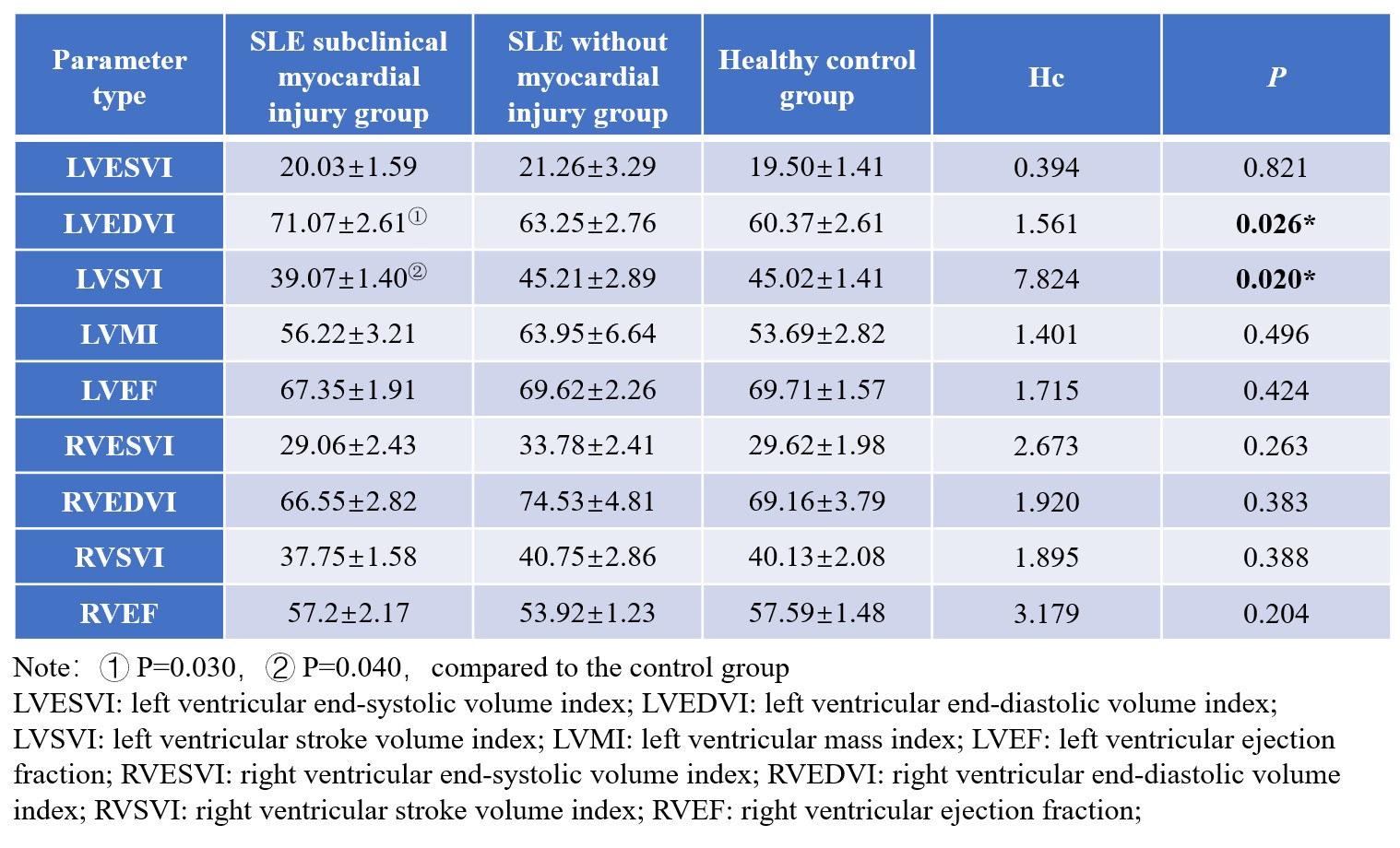
Table 2. Comparison of left and right ventricular function in the three groups
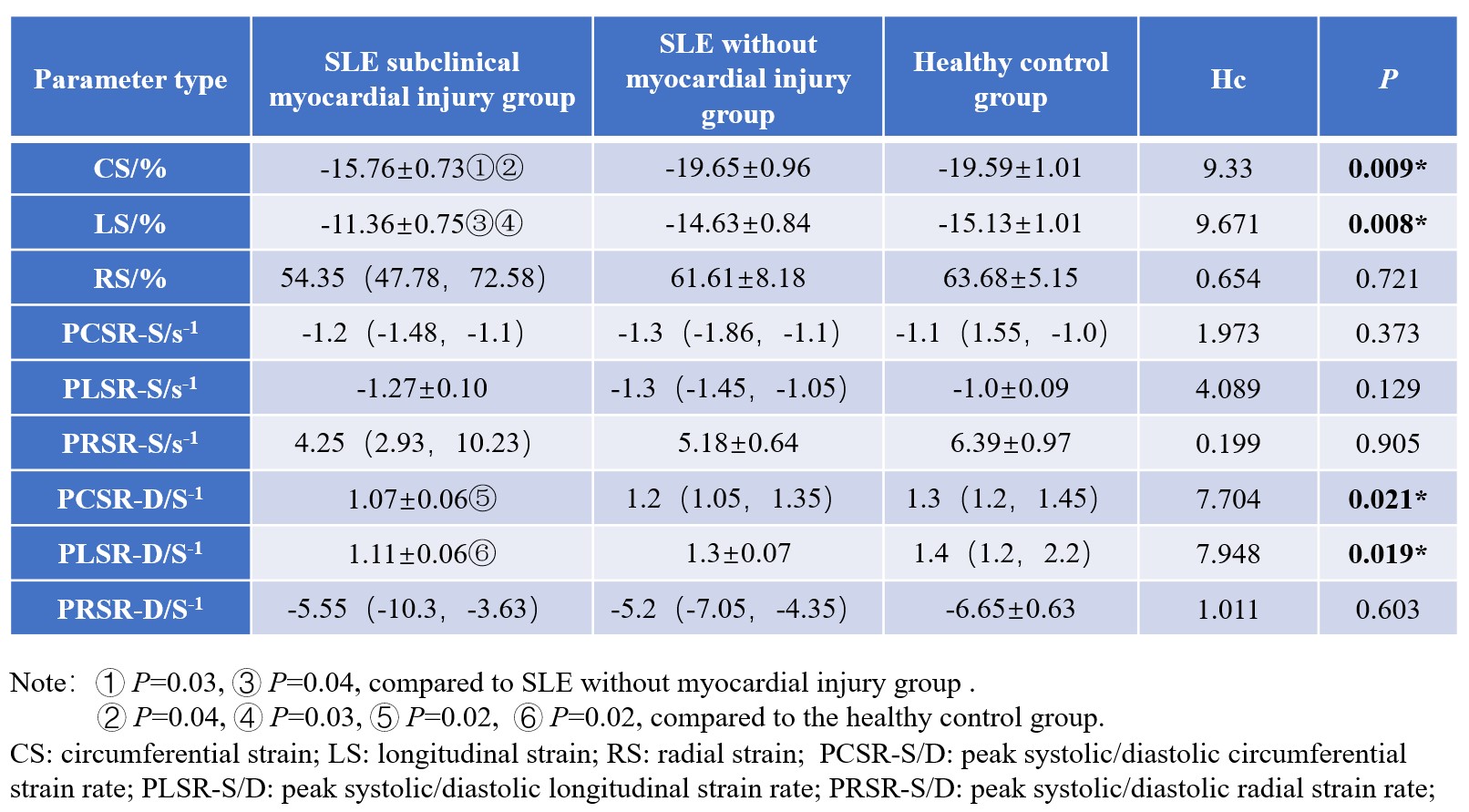
Table 3. Comparison of left ventricular myocardial strain parameters