3517
Prostate MRI at 7T using high-performance gradients and an 8Tx/16Rx RF array: a clinical feasibility study1CIBM Center for Biomedical Imaging, Lausanne, Switzerland, 2Animal Imaging and Technology, EPFL, Lausanne, Switzerland, 3Division of Radiology, Geneva University Hospital and University of Geneva, Geneva, Switzerland, 4Advanced Clinical Imaging Technology, Siemens Healthineers International AG, Lausanne, Switzerland, 5CIBM Center for Biomedical Imaging, Geneva, Switzerland, 6Human Neuroscience Platform, Fondation Campus Biotech Geneva, Geneva, Switzerland, 7Fondation Campus Biotech Geneva, Geneva, Switzerland, 8Department of Radiology, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland, 9LTS5, EPFL, Lausanne, Switzerland, 10Physikalisch-Technische Bundesanstalt (PTB), Braunschweig and Berlin, Germany, 11Institute of Radiology, University Hospital Erlangen and Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), Erlangen, Germany, 12Electrical Engineering and Information Technology, University of Applied Sciences – FH Aachen, Aachen, Germany, 13Rapid Biomedical, Rimpair, Germany, 14Siemens Healthineers, Erlangen, Germany, 15Division of Urology, Geneva University Hospital and University of Geneva, Geneva, Switzerland
Synopsis
Keywords: Prostate, Prostate, High-field MRI
Motivation: To better detect and delineate prostate cancer using ultrahigh field MRI.
Goal(s): To investigate if clinical prostate MRI at 7T using recent technological advances is feasible.
Approach: Prostate MRI was performed in 5 healthy volunteers using the latest generation of whole-body 7T MRI scanners incorporating enhanced gradient performance, advanced deep learning based image reconstruction and an 8Tx/16Rx torso array.
Results: High image quality with an unprecedented spatial resolution and a sharpness obtained at 7T outperformed those obtained at 3T even when time-matched sequences were acquired.
Impact: The preliminary data obtained from several volunteers provides a great encouragement to start clinical studies in prostate cancer patients.
Introduction
Prostate MRI at 7T holds the promise of an increased spatial resolution to better detect and delineate prostate cancer. So far, only few reports have investigated the potential of T2 and DWI which are the two main clinical MR sequences for prostate cancer (PCa) imaging at 7T. Using an external transmit/receive (TxRx) array, satisfactory to good quality T2 images of the prostate were obtained at the resolution of (0.75 x 0.75 x 3)mm3 in 17 PCa patients1 and in 9 volunteers, and 12 PCa patients after a time-consuming B1 shimming2. With the addition of an Rx-only endorectal coil, an increased resolution of (0.3 x 0.3 x 2)mm3 was possible in T2 images of 13 PCa patients3. Regarding DWI, a single study demonstrated good image quality of clinical utility in 11 over 12 PCa patients using an 8-channel Tx array and an endorectal Rx coil3. This small number of results indicates that prostate MRI at 7T remains a challenge. Therefore, the aim of our work was to investigate the clinical feasibility of prostate MRI at 7T using the latest generation of whole-body 7T MRI scanners incorporating enhanced gradient performance, advanced deep learning based image reconstruction and an 8Tx/16Rx torso array.Methods
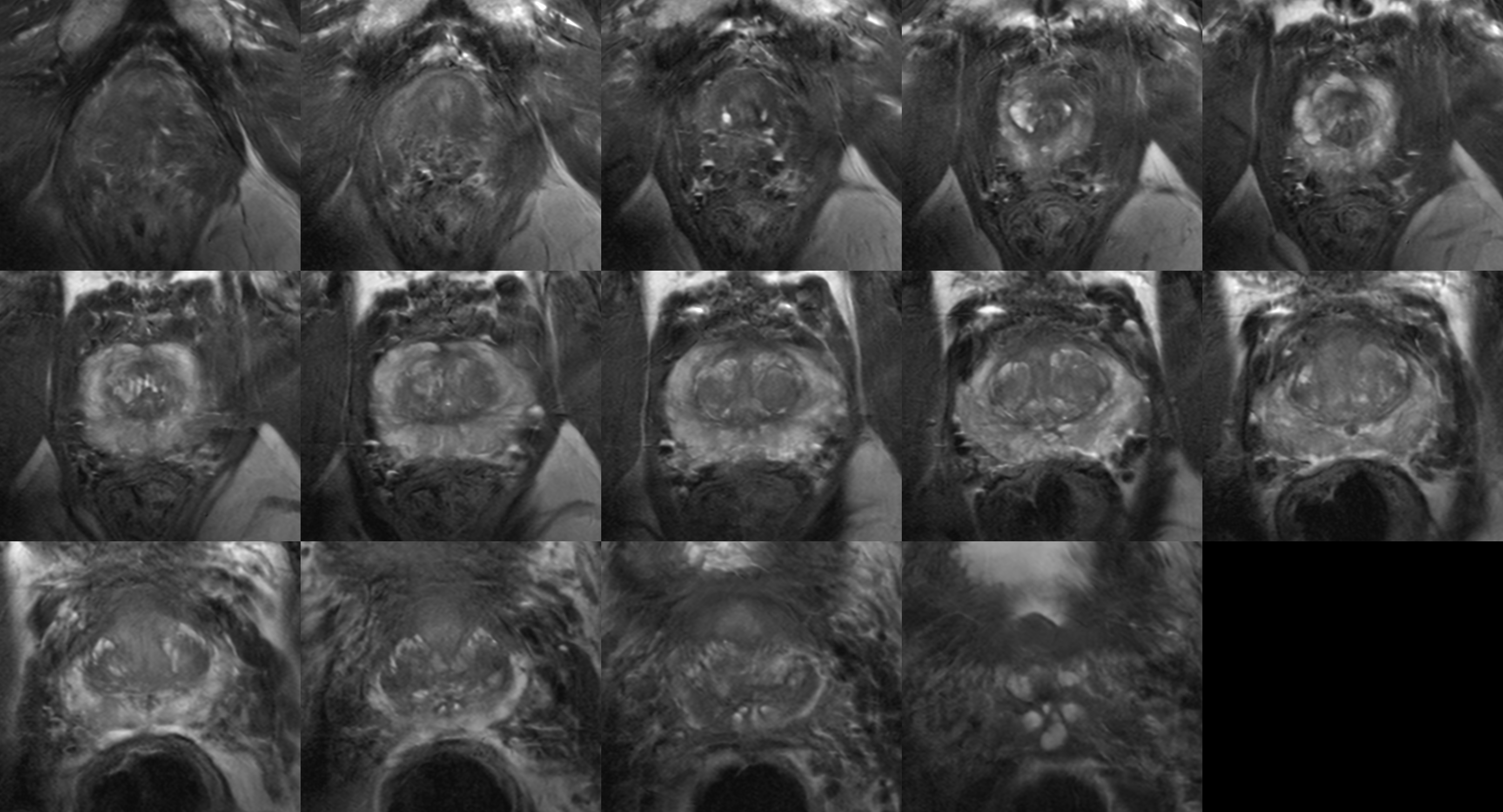
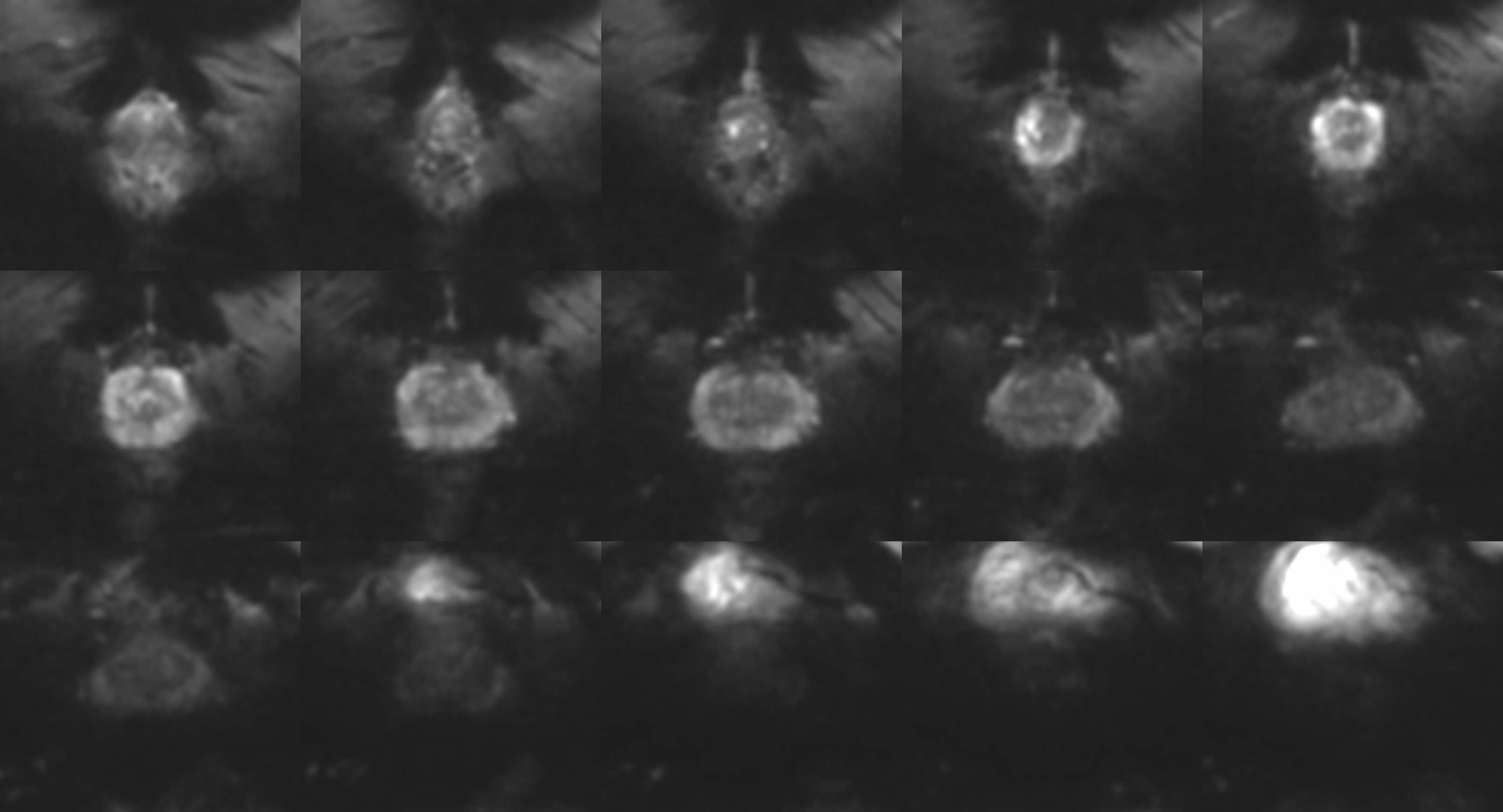
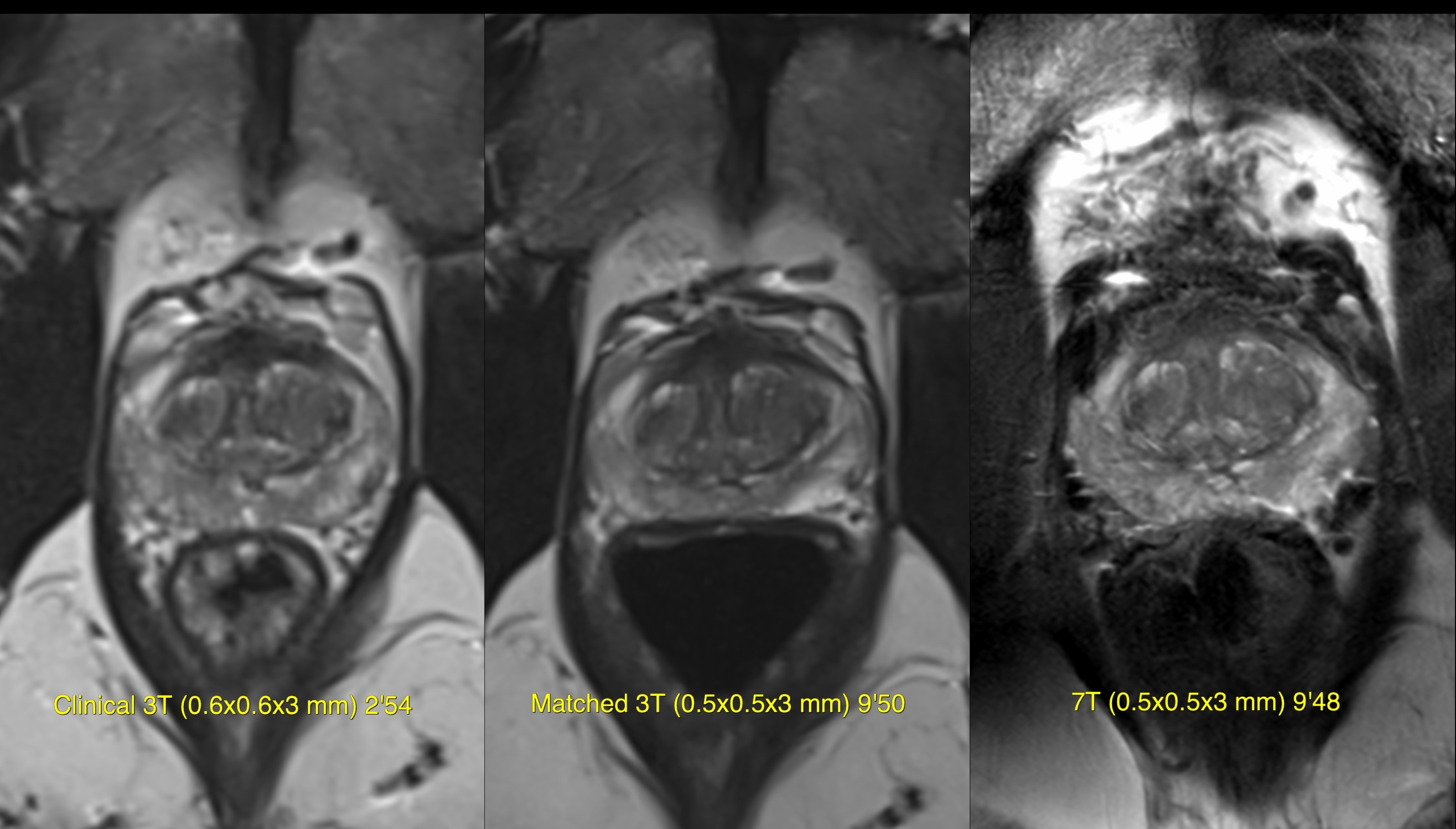
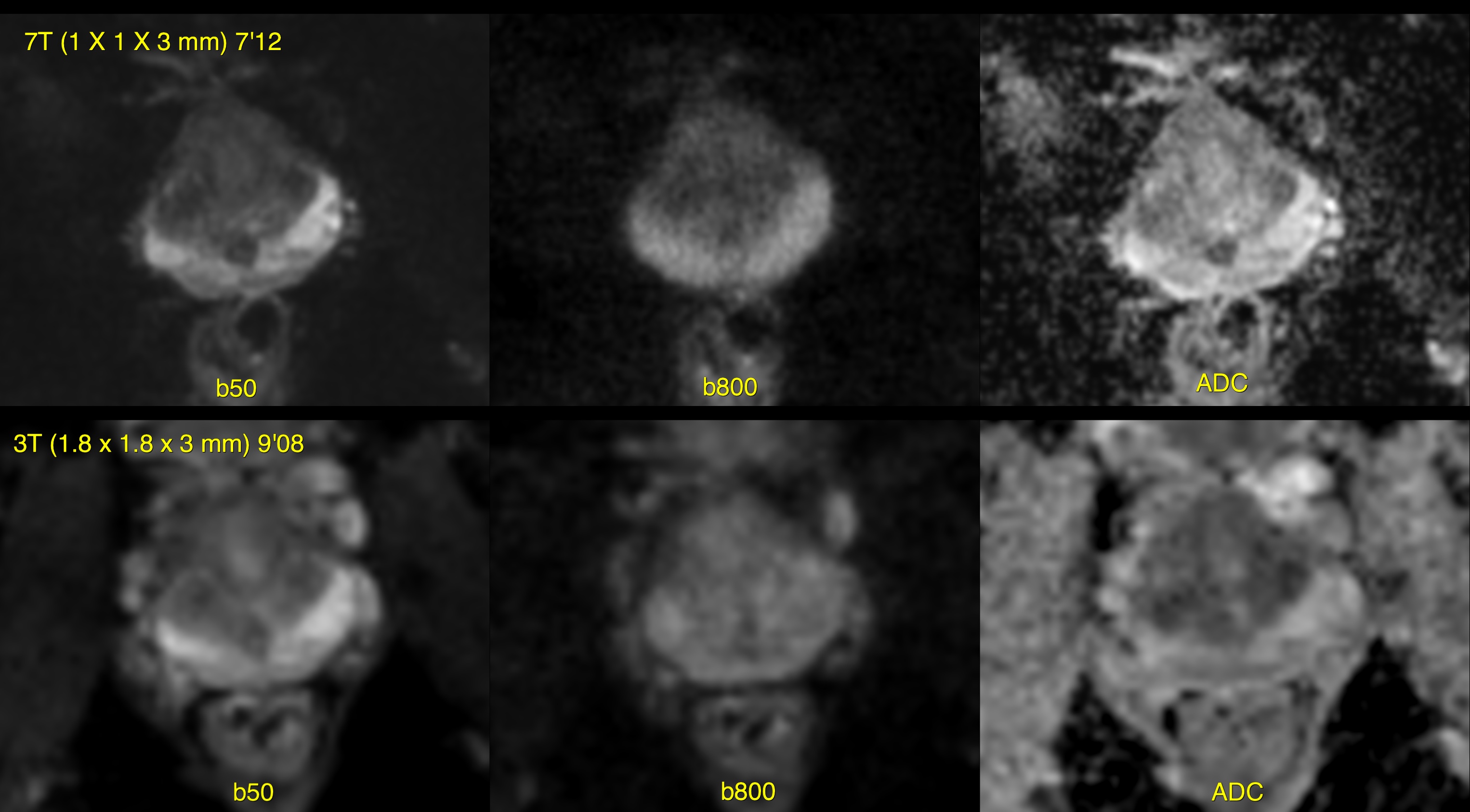
Healthy volunteers (n=5, 47 ± 10 years old) were scanned on a Siemens 7T (MAGNETOM Terra.X, Siemens Healthcare, Erlangen, Germany) with a gradient strength of 130 T/m at 250 mT/m/s with an 8Tx/16Rx RF coil array (Rapid Biomedical, Germany) as well as on a 3T MR scanner (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) with an 18-channel Rx only coil after an overnight fasting period for quality control tests. The following sequences were acquired at 7T: T2-TSE (TE = 87 ms, TR = 12100 ms, 0.5x0.5x3 mm3 acquired and 0.2x0.2x3 mm3 after interpolation, iPAT = 2 (axial plane) and iPAT = 4 (sagittal and coronal plane), deep resolve boost and sharp, deepRXE bias-field correction, 14 slices in 10:40 min and 6:12 min); Segmented resolve SE-DWI (TE=54 ms, TR=5740 ms, 5 shots, 1 x 1 x 3 mm3, 15 slices, in 9:58 min) and water excitation T1 3D-GRE (TE=4.5 ms, TR=12 ms, 1 x 1 x 2 mm3, in 4:05 min) using a vendor-provided B0 and B1 shim for prostate. Corresponding MR sequences were applied at 3T using the standard clinical parameters as well as increased resolution with time matching acquisition for the T2-TSE in the axial plane. Central and peripheral SNR (in the most homogeneous areas with ROI standard deviation as a noise measure) and qualitative blinded image analysis were performed by 4 radiologists to compare MR images between 7T and 3T.Results
High image quality was successfully obtained in all the volunteers at 7T. T2-TSE was applied with a TR of 12100 ms to resolve SAR restrictions. Homogeneous signal intensity was obtained for the T1- and T2-weighted images in the prostate although some signal drop was observed in the periprostatic fat in 2 volunteers (Fig. 1 and 2). No significant distortions were observed in DWI in all the directions (Fig. 3). In comparison to standard clinical acquisitions or even resolution and duration-matched acquisitions at 3T, 7T images demonstrated higher signal sensitivity and spatial resolution (Fig. 4 and 5). Using a 5 points Likert scale (from 1= worst to 5 = best), signal homogeneity of T2 images was graded 5 at 3T and 4.2 at 7T and image quality 3.3 at 3T and 4.2 at 7T. The SNR for 3T clinical T2, 3T matched T2 and 7T T2 images in the central zone, respectively the peripheral zone was 3.9±1.2, 5.3±1.8 and 8.4±4.1, respectively 7.2±2.5, 7.3±0.9 and 9.3±2.3. The signal ratio between the peripheral and central zones for 3T clinical T2, 3T matched T2 and 7T T2 images was 2.4±0.9, 2.4±0.7 and 1.8±0.5.Discussion
This work demonstrates for the first time that high-quality prostate MRI using a dedicated RF array and a 7T Terra.X system is feasible. High homogeneity of the signal intensity was observed for each volunteer, and it was achieved without the need of using subject-specific B1 shimming4. In addition, no endorectal RF coil was needed to obtain high quality T2 and DWI images with an unprecedented spatial resolution and a sharpness that outperform those obtained at 3T even when time-matched sequences were acquired.Conclusion
Clinical prostate MRI can benefit from recent advances in ultrahigh field MRI technology. The preliminary data obtained from several volunteers provides a great encouragement to start clinical studies in PCa patientsAcknowledgements
We acknowledge access to the facilities and expertise of the CIBM Center for Biomedical Imaging, a Swiss research center of excellence founded and supported by Lausanne University Hospital (CHUV), University of Lausanne (UNIL), Ecole polytechnique fédérale de Lausanne (EPFL), University of Geneva (UNIGE) and Geneva University Hospitals (HUG). We also acknowledge access to the facilities and expertise of the Fondation Campus Biotech Geneva.References
1. E. K. Vos, M. W. Lagemaat, J. O. Barentsz, J. J. Futterer, P. Zamecnik, H. Roozen, S. Orzada, A. K. Bitz, M. C. Maas, T. W. Scheenen, Image quality and cancer visibility of T2-weighted magnetic resonance imaging of the prostate at 7 Tesla. Eur Radiol 24, 1950-1958 (2014).
2. M. C. Maas, E. K. Vos, M. W. Lagemaat, A. K. Bitz, S. Orzada, T. Kobus, O. Kraff, S. Maderwald, M. E. Ladd, T. W. Scheenen, Feasibility of T2 -weighted turbo spin echo imaging of the human prostate at 7 tesla. Magn Reson Med 71, 1711-1719 (2014).
3. M. W. Lagemaat, B. W. Philips, E. K. Vos, M. J. van Uden, J. J. Futterer, S. F. Jenniskens, T. W. Scheenen, M. C. Maas, Feasibility of Multiparametric Magnetic Resonance Imaging of the Prostate at 7 T. Invest Radiol 52, 295-301 (2017).
4. G. J. Metzger, C. Snyder, C. Akgun, T. Vaughan, K. Ugurbil, P. F. Van de Moortele, Local B1+ shimming for prostate imaging with transceiver arrays at 7T based on subject-dependent transmit phase measurements. Magn Reson Med 59, 396-409 (2008).
Figures