3512
Magnetic Resonance Elastography to Identify Prostate Phenotypes of Lower Urinary Tract Symptoms1Radiology, Urology, University of Michigan, Ann Arbor, MI, United States, 2University of Wisconsin School of Medicine and Publich Health, Madison, WI, United States, 3University of Wisconsin, Madison, WI, United States, 4University of Michigan, Ann Arbor, MI, United States
Synopsis
Keywords: Prostate, Elastography, MRE, Lower Urinary Tract Symptoms, Shear Stiffness, LUTS
Motivation: There is a critical need for significant improvements in image-based assessment of the prostate in men with lower urinary tract symptoms (LUTS).
Goal(s): To develop non-invasive image-based biomarkers that will optimize clinical management of men with LUTS.
Approach: Quantify transition zone complex shear modulus (henceforth ‘stiffness’) with transperineal magnetic resonance elastography (pMRE) at 90Hz and 100Hz.
Results: Mean periurethral TZ stiffness increases with frequency (3.0clip_image006.png">0.4kPa).
Impact: Transperineal pMRE is technically feasible, generates volumetric whole prostate quantitative parametric maps that can differentiate zonal prostate anatomy. Periurethral TZ stiffness, measured with pMRE, may be a clinically useful biomarker for identifying discrete phenotypes of LUTS.
Introduction
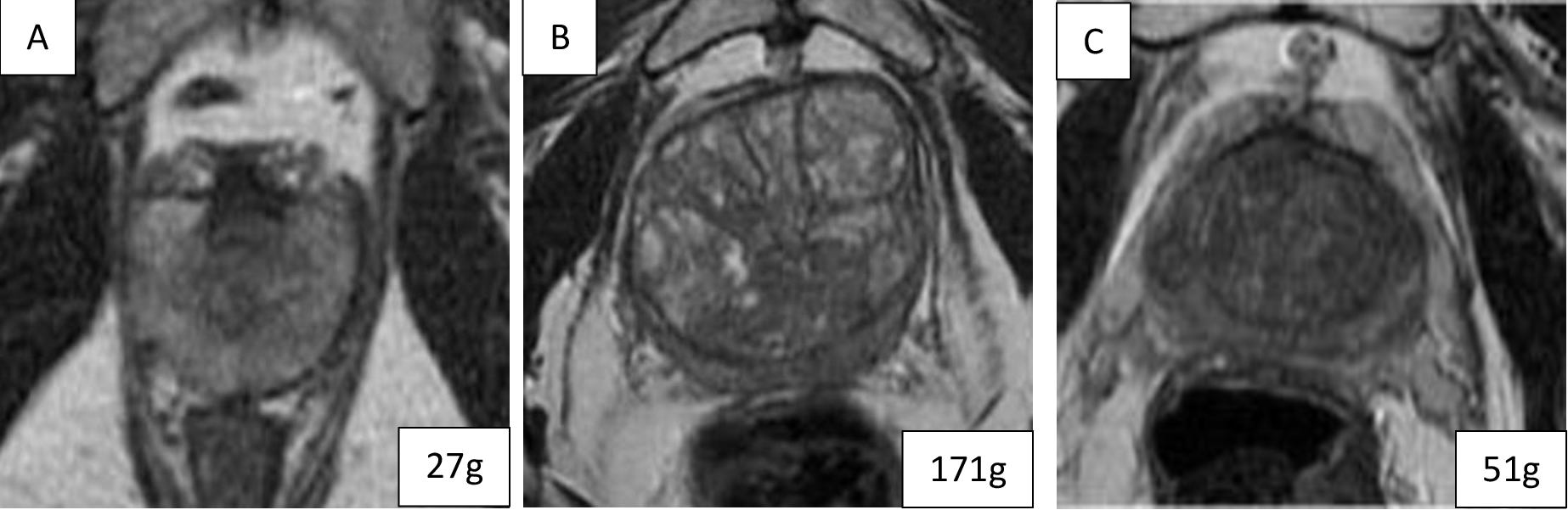
The prevalence of lower urinary tract dysfunction (LUTD), frequently attributed to benign prostatic hyperplasia (BPH), increases with age and ranges from 50-75% of men over 50. Without effective treatment, LUTD can lead to bladder dysfunction, acute urinary retention, and death. Stromal and glandular hyperplasia, inflammation, and fibrosis throughout the transition zone (TZ) are associated with BPH. These histologic changes alter the local tissue properties and cause increase in prostate size and progressive thickening of the prostate capsule (Figure 1). Increase in prostate size and the spatial relationship of the histologic changes relative to the urethra likely alter flow dynamics across the prostatic urethra, contribute to bladder remodeling and ultimately LUTS1-2. Magnetic resonance elastography (MRE) can interrogate the in-vivo mechanical properties of tissue. Combining mpMRI and prostate MRE (pMRE) may provide a robust and reproducible 3D map of the prostate that simultaneously quantifies prostate and TZ volume, spatial heterogeneity of TZ histology and the corresponding impact of these histologic changes on periurethal, zonal and whole gland prostate stiffness.Materials and Methods
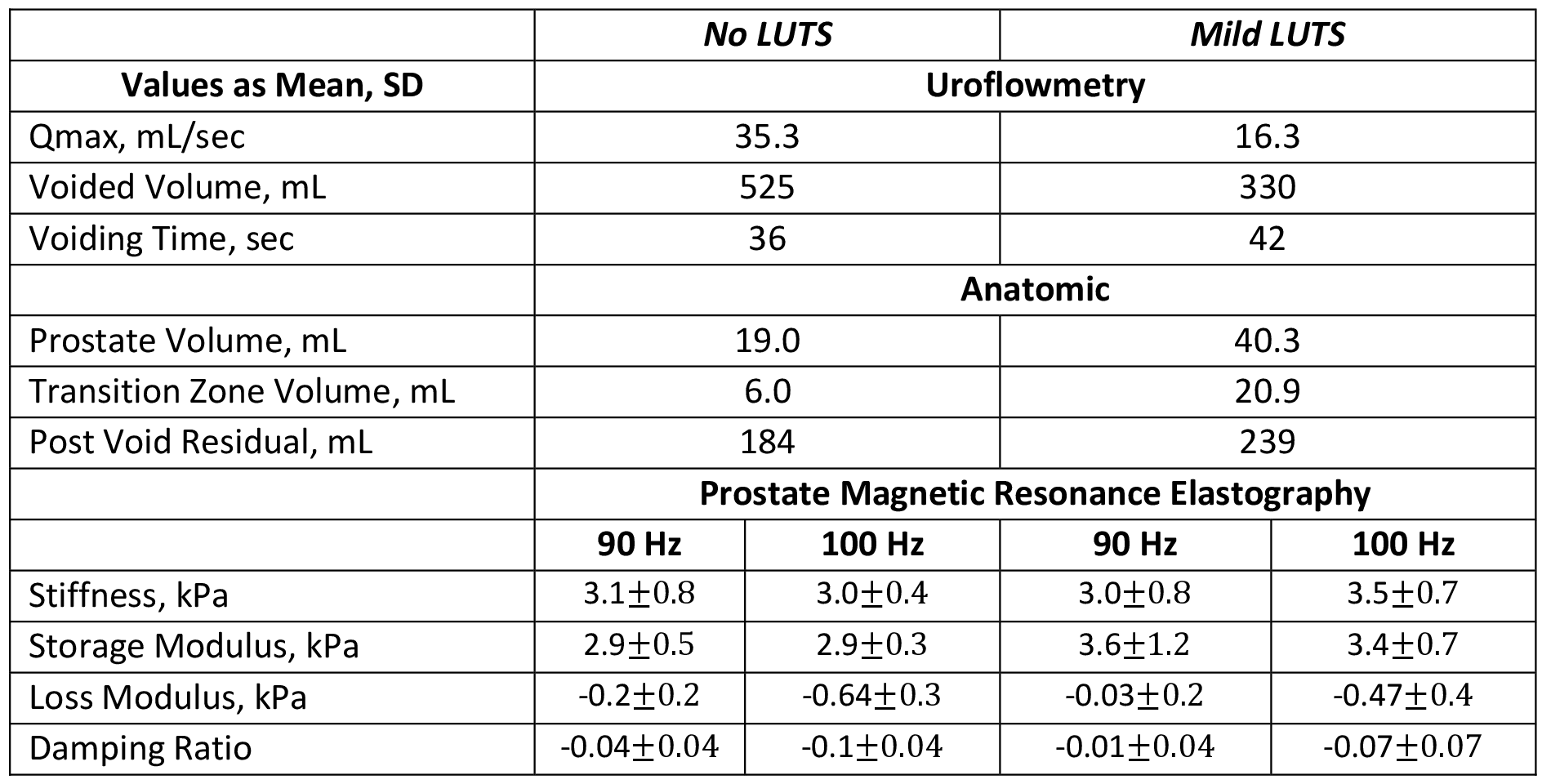
Study Design Subjects without and with LUTS were recruited to participate in this ongoing prospective clinical trial. Biometric data, symptom index scores, medications/herbal therapies and uroflowmetry were recorded. mpMRI including pMRE (3.0T Premier, GE Healthcare, Waukesha, WI, USA) was performed with subjects in the supine position using the integrated body coil and anterior 32-channel array coil (AIR, GE Healthcare, Waukesha, WI, USA). Acquisitions included axial, sagittal and coronal T2 TSE, axial diffusion weighted imaging (DWI) (b800 and b1500) with apparent diffusion coefficient (ADC) maps, axial pre- and dynamic post-contrast enhancement (DCE) T1 FSPGR. Magnetic Resonance Elastography Prior to mpMRI, a prototype passive driver was secured to the perineum and connected to a commercially available active driver (Resoundant Inc., Rochester, MN, USA). Axial 3D pMRE3 (no breath holds) was performed at 90 and 100Hz vibration frequencies with the following parameters: FOV=30cm, TE/TR=57.6-74.0ms/1600ms, flip angle=90, slices=18, slice thickness=2.9mm, slice gap=0, matrix=96x96, BW=256Hz, averages=1, acceleration=2. Wave images were processed with a 3D direct-inversion algorithm. Three quantitative parametric maps for viscoelastic properties were generated: complex shear modulus (|G*|), storage modulus (G’) and loss modulus (G”). The damping ratio4 (z=G”/2G’) was calculated. Following mpMRI and MRE, a tolerability questionnaire was completed by the subject. Image and Statistical Analysis MRI and pMRE images were analyzed offline by an experienced analyst and GU radiologist. Prostate and TZ volume and postvoid residual (PVR) were quantified on axial (prostate) and sagittal (bladder) T2 TSE with 3D software (Materialise Mimics, Leuven, BE). A free-form region-of-interest (ROI) was drawn in the TZ around the urethra, at the level of the verumontanum (midgland) and prostate base (slice immediately below the bladder neck) on the axial T2 TSE and copied to the three quantitative maps. Demographic, biometric, uroflowmetry, anatomic and prostate viscoelastic properties measured during pMRE were summarized descriptively. Continuous variables were expressed as mean standard deviation or median and interquartile range (IQR).Results and Discussion
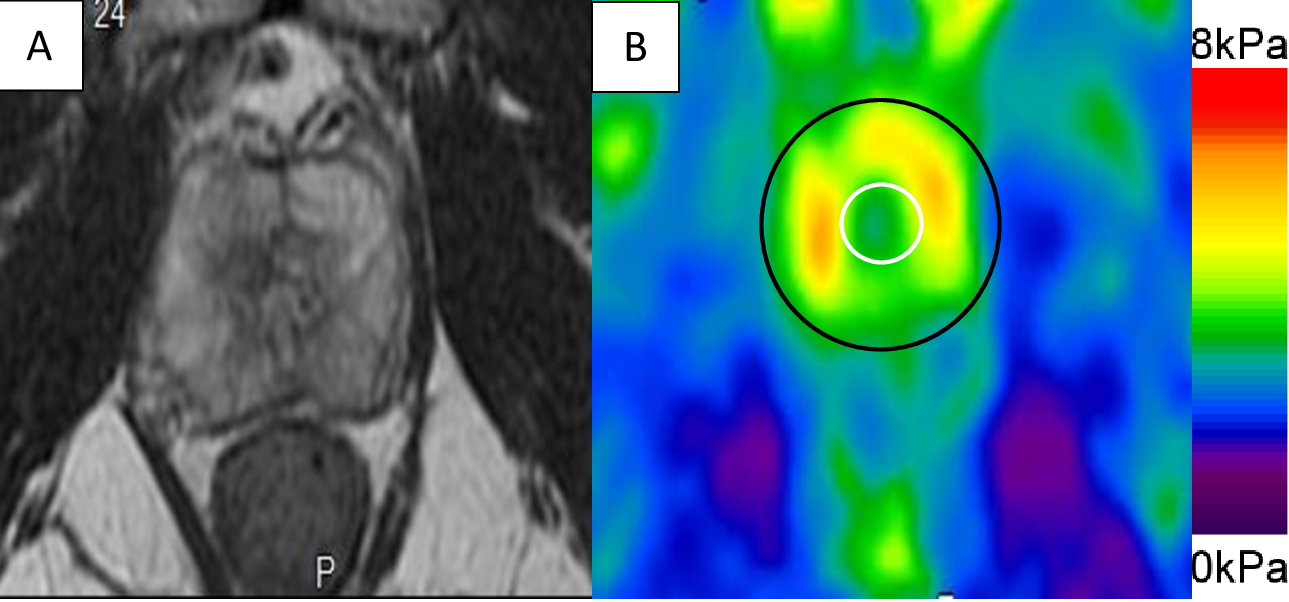
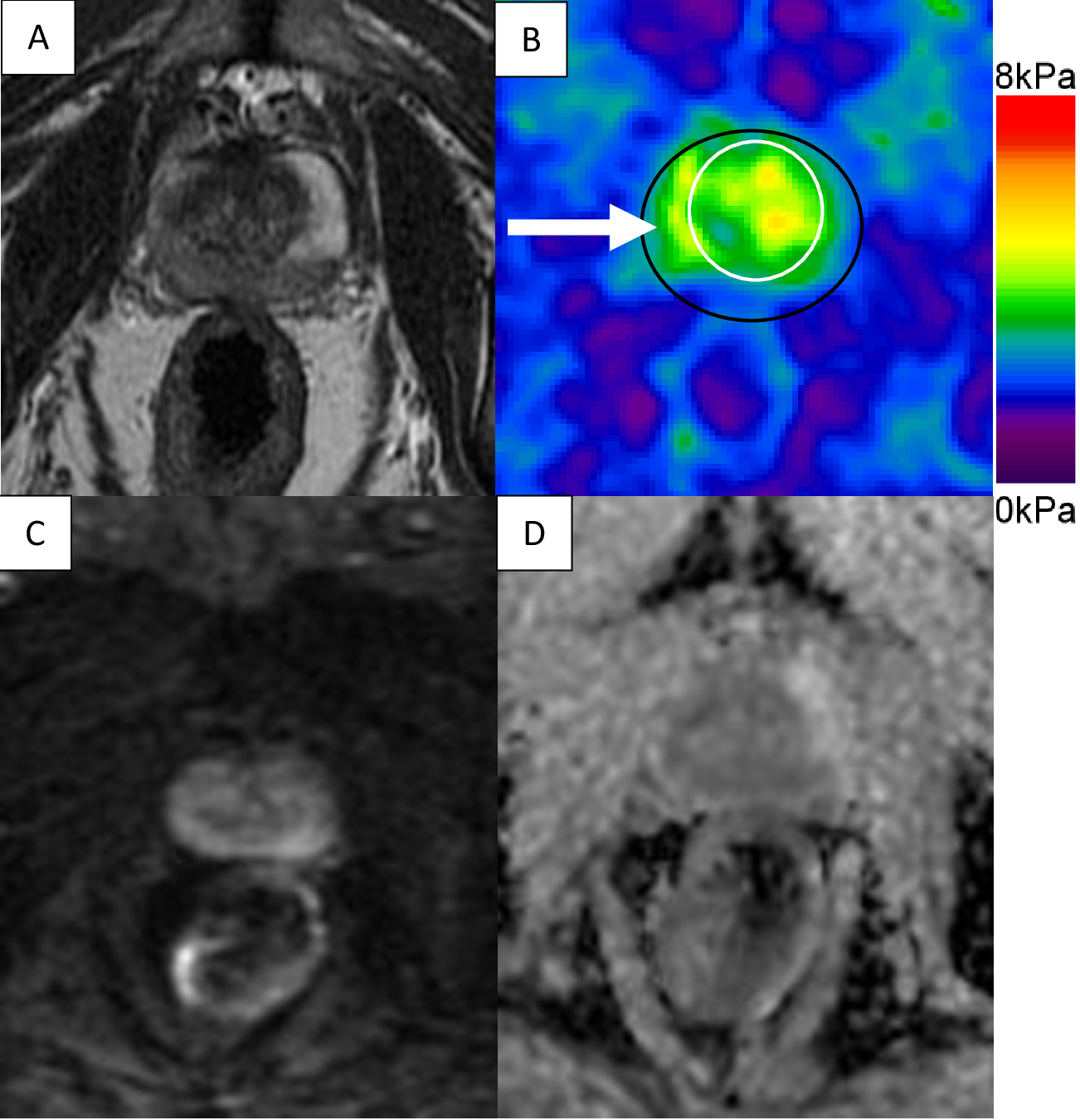
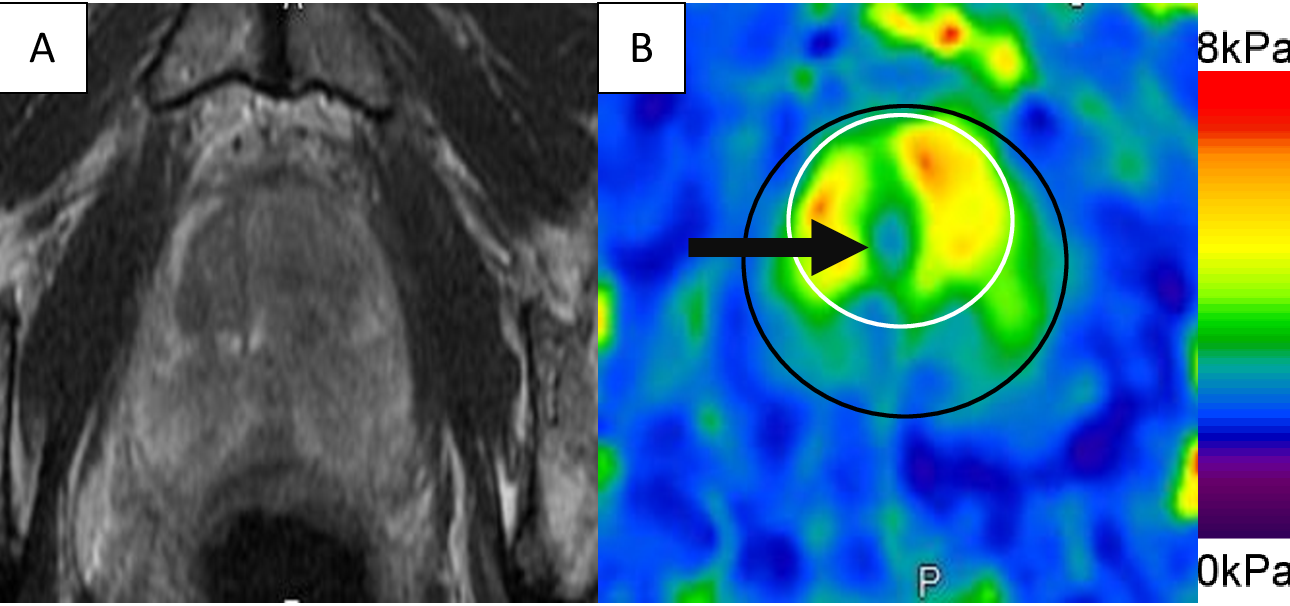
Ten subjects (n=5 without LUTS, n=5 with mild LUTS (AUA-SI£7) had a mean age (SD) of 39.316.9 and mean BMI (SD) of 26.94.5. Mean Qmax and voided volume were lower and voiding time longer for subjects with LUTS (Table 1). Subjects with LUTS were older (51.4 vs 27.2 years) and had higher mean prostate and TZ volumes and PVR. These data suggest that the anatomic and histologic changes that occur in the prostate are associated with alteration in bladder function even in mildly symptomatic men. pMRE was successful and well-tolerated in all subjects (Figures 2-4). As expected, the mean stiffness of the periurethral TZ increased with frequency (3.0vs 3.3kkPa). Mean TZ stiffness was higher in the midgland compared to the base at both frequencies (90Hz: 2.9 vs 2.4kPa, 100Hz: 3.20.6vs 2.80.4kPa). Mean stiffness of the TZ (base+midgland) was higher in subjects with LUTS at 100Hz but similar at 90Hz (Table 1). These data demonstrate the spatial heterogeneity of tissue stiffness surrounding the prostatic urethra. Stiffer tissues, such as fibrosis, may be contributing to limited urethral opening with the resulting increased pressure transmitted to the bladder, leading to bladder remodeling and LUTS. The mean storage and loss modulus were higher and damping ratio lower in subjects with LUTS at both frequencies (Table 1). These spatial differences in elasticity (storage) and viscosity (loss) combined with stiffness and mpMRI may improve our ability to non-invasively characterize the histology of the TZ and characterize prostate phenotypes of LUTS.Conclusion
Transperineal pMRE is technically feasible, generates volumetric whole prostate quantitative parametric maps that may be a clinically useful biomarker for identifying discrete phenotypes of LUTS.Acknowledgements
Research reported in this work was supported by the National Institutes of Health under grant number U54 DK104310 and the Society of Abdominal Radiology under the Morton A. Bosniak Research Award. We are grateful for the inkind support and expertise of Dr. Richard Ehman and Dr. Kay Pepin.References
1. McConnell JD, Roehrborn CG, Bautista OM, et al. The long-term effect of doxazosin, finasteride and combination therpay on clinical progression of benign prostatic hyperplasia. N Engl J Med. 2003 Dec 18;349(25):2387-98.
2. Fusco F, Creta M, DeNunzio C, et al. Progressive bladder remodeling due to bladder outlet obstruction: A systematic review of morphologic and molecular evidence in humans. BMC Urol. 2018 Mar 9;18(1):15.
3. Yali Q, Middleton MS, Loomba R, et al. Magnetic resonance elastography biomarkers for the detection of histologic alterations in nonalcoholic fatter liver disease in the absence of fibrosis. Eur Radiol. 2021 Nov;31(11):8408-19.
4. Manduca A, Bayly PJ, Ehman RL, et al. MR elastography: Principles, guidelines, and terminology. Magn Reson Med. May;85(5):2377-90.
Figures