3510
Diffusion-prepped fast spin echo sequence for prostate MR to overcome distortion and signal loss in diffusion weighted imaging1Radiology, Stanford University, Stanford, CA, United States, 2Bioengineering, Stanford University, Stanford, CA, United States, 3Electrical Engineering, Stanford University, Stanford, CA, United States
Synopsis
Keywords: Prostate, Artifacts
Motivation: Clinically utilized diffusion weighted imaging (DWI), an essential part of prostate MRI, relies on echo planar imaging (EPI) and is prone to geometric distortion and signal loss due to susceptibility from rectal gas and metal hip prostheses.
Goal(s): To improve the robustness of prostate DWI in the setting of field inhomogeneities from hip prostheses and rectal gas.
Approach: Prospective study of 10 patients undergoing prostate MRI with diffusion prepped fast spin echo (FSE) sequence, as well as single-shot and multi-shot DW-EPI, comparing prostate measurements.
Results: We show feasibility of using a diffusion prepped FSE sequence in prostate MR with decreased distortion and artifact.
Impact: A diffusion prepped fast-spin echo sequence avoids distortion and signal loss from susceptibility artifacts seen with echo planar imaging, and is a feasible method to obtain robust diffusion weighted imaging of the prostate.
Introduction
Prostate cancer is the most common male cancer, with 1.4 million new cases reported globally in 20201. MRI has become a key element in the screening and diagnosis of prostate cancer, and diffusion weighted imaging (DWI) is central to the specificity of these prostate MRI examinations2. However, clinically utilized DWI sequences are based on spin-echo echo-planar imaging (SE-EPI), and issues arise from the sensitivity of the echo-planar readout to field inhomogeneities due to metallic hip implants or significant rectal gas in prostate MRI patients3. The susceptibility artifacts associated with these sources of field inhomogeneity results in significant distortion and signal loss, potentially leading to non-diagnostic DWI acquisitions. With prevalence of total hip arthroplasty in adults above 50 in the US being 2.34% as of 20104 and predicted to rise continuously in the coming decades5, this issue will become even more common. Previous studies have shown decreases in gas-induced susceptibility artifacts with micro-enemas6, however, this may not always be logistically feasible, and no similar solution is possible for hip implants. Diffusion weighted fast spin echo (DW-FSE) offers an alternative means to obtain diffusion imaging without distortion from off-resonance, and with decreased signal loss from susceptibility7. Our objective is to test feasibility of a diffusion prepared fast spin-echo sequence for use in prostate imaging, by comparison to SE-EPI based multi-shot DWI (msDWI) and reduced field of view (rFOV) single shot DWI (ssDWI).Methods
This prospective study enrolled patients undergoing prostate MRI with IRB approval and informed consent. Ten (N=10) patients underwent prostate MRI, which included a 2D rFOV ssDWI (GE FOCUS), a 2D msDWI (GE MUSE8), and a 3D rFOV diffusion-prepared fast spin echo (DW-FSE) 9,10. As part of our standard institutional protocol all patients were instructed to perform a fleet enema prior to arriving at the facility6. Scans were obtained on 3T scanners (GE Healthcare 3T SIGNA Premier, Waukesha, WI) using a 30-channel anterior phased array coil (AIR coil, GE Healthcare) and a 60-channel phased-array posterior coil. Imaging parameters are summarized in Table 1. To compare distortion in images the visible prostate was measured on all three diffusion sequences in the axial plane in anteroposterior (AP) and mediolateral (ML) dimensions, and a ratio was obtained by dividing the two values. All measurements were performed on the high b-value (500s/mm2 or 800s/mm2) diffusion images.Results
Of the 10 patients enrolled, 1 had a metallic hip implant. There was good agreement between the measurements of the prostate on all DWI sequences in comparison to T2-weighted FSE in the absence of hip implants (Fig 2). For the patient with the metallic hip implant the measurements in the mediolateral dimension were significantly distorted for the ssDWI and msDWI sequences in comparison to the DWI-FSE sequence.In two patients without hip implants with significant findings (PI-RADS 4 lesion – Fig 3, prostate abscess – Fig 4), all 3 sequences gave diagnostic results. For the patient with the hip implant (Fig 5), both ssDWI and msDWI demonstrated significant distortion and loss of signal obscuring the majority of the right prostate gland, while DWI-FSE gave diagnostic images.
Discussion
Our results are consistent with prior studies that have shown decreased artifacts with diffusion weighted fast spin echo 7,9,10. We showed that lesions with restricted diffusion remain conspicuous on DWI-FSE, and that in the case of a hip implant there was improved visualization and decreased distortion of the prostate with DWI-FSE.While DWI-FSE is insensitive to susceptibility artifacts, the primary drawback is that the signal is halved due to the stimulated echo used for eliminating non-CPMG artifacts9. This signal reduction was offset by reducing the voxel size of the DWI-FSE relative to DW-EPI, and by increasing the number of averages (with the drawback of increasing the scan time).
Another limitation was the absence of fat saturation in the DWI-FSE. In the presence of off-resonance from hip replacements, inversion recovery (STIR) is required to robustly suppress fat, since chemically selective fat suppression may saturate water signal. However, STIR additionally reduces SNR and therefore was not employed.
While our current study shows promising results, it is limited by a small sample size and will need further validation in larger cohorts, particularly in more patients with hip replacements.
Conclusion
Diffusion prepared FSE is a promising alternative to both single-shot and multi-shot EPI diffusion weighted imaging in patients with metallic hip replacements or significant rectal gas artifact.Acknowledgements
This project received research support from GE Healthcare.References
1. Wang, L., Lu, B., He, M., Wang, Y., Wang, Z., & Du, L. (2022). Prostate Cancer Incidence and Mortality: Global Status and Temporal Trends in 89 Countries From 2000 to 2019. Frontiers in Public Health, 10, 811044. https://doi.org/10.3389/fpubh.2022.811044
2. PIRADS-V2-1.pdf. (n.d.). Retrieved November 5, 2023, from https://www.acr.org/-/media/ACR/Files/RADS/Pi-RADS/PIRADS-V2-1.pdf?la=en
3. Stocker, D., Manoliu, A., Becker, A. S., Barth, B. K., Nanz, D., Klarhöfer, M., & Donati, O. F. (2018). Image Quality and Geometric Distortion of Modern Diffusion-Weighted Imaging Sequences in Magnetic Resonance Imaging of the Prostate. Investigative Radiology, 53(4), 200–206. https://doi.org/10.1097/RLI.0000000000000429
4. Maradit Kremers, H., Larson, D. R., Crowson, C. S., Kremers, W. K., Washington, R. E., Steiner, C. A., Jiranek, W. A., & Berry, D. J. (2015). Prevalence of Total Hip and Knee Replacement in the United States. The Journal of Bone and Joint Surgery. American Volume, 97(17), 1386–1397. https://doi.org/10.2106/JBJS.N.01141
5. Shichman, I., Roof, M., Askew, N., Nherera, L., Rozell, J. C., Seyler, T. M., & Schwarzkopf, R. (2023). Projections and Epidemiology of Primary Hip and Knee Arthroplasty in Medicare Patients to 2040-2060. JBJS Open Access, 8(1), e22.00112. https://doi.org/10.2106/JBJS.OA.22.00112
6. van Griethuysen, J. J. M., Bus, E. M., Hauptmann, M., Lahaye, M. J., Maas, M., ter Beek, L. C., Beets, G. L., Bakers, F. C. H., Beets-Tan, R. G. H., & Lambregts, D. M. J. (2018). Gas-induced susceptibility artefacts on diffusion-weighted MRI of the rectum at 1.5 T – Effect of applying a micro-enema to improve image quality. European Journal of Radiology, 99, 131–137. https://doi.org/10.1016/j.ejrad.2017.12.020
7. Lee, S.-Y., Meyer, B. P., Kurpad, S. N., & Budde, M. D. (2021). Diffusion-prepared fast spin echo for artifact-free spinal cord imaging. Magnetic Resonance in Medicine, 86(2), 984–994. https://doi.org/10.1002/mrm.28751
8. Chen, N., Guidon, A., Chang, H.-C., & Song, A. W. (2013). A robust multi-shot scan strategy for high-resolution diffusion weighted MRI enabled by multiplexed sensitivity-encoding (MUSE). NeuroImage, 72, 41–47. https://doi.org/10.1016/j.neuroimage.2013.01.038
9. Zhang, Q., Coolen, B. F., Versluis, M. J., Strijkers, G. J., & Nederveen, A. J. (2017). Diffusion-prepared stimulated-echo turbo spin echo (DPsti-TSE): An eddy current-insensitive sequence for three-dimensional high-resolution and undistorted diffusion-weighted imaging. NMR in Biomedicine, 30(7). https://doi.org/10.1002/nbm.3719
10. Hess, J. J., Lee, P. K., Zhou, X., Loening, A. M., & Hargreaves, B. A. (2023). 3D Distortionless Diffusion Weighted Imaging in the Prostate using a Diffusion Prepared Fast Spin-Echo Sequence. ISMRM Annual Conference 2023:2071.
Figures
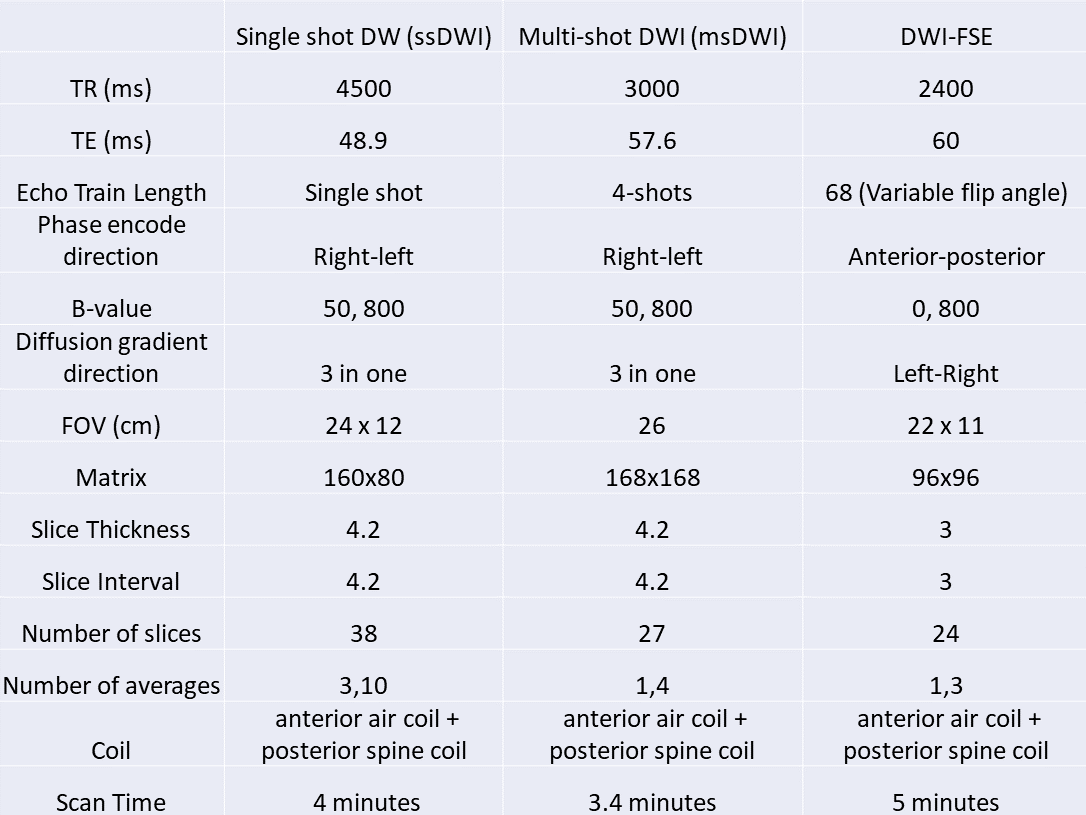
Figure 1. MRI parameters for the three diffusion sequences utilized. TR: repetition time; TE: time to echo; FOV: field of view.
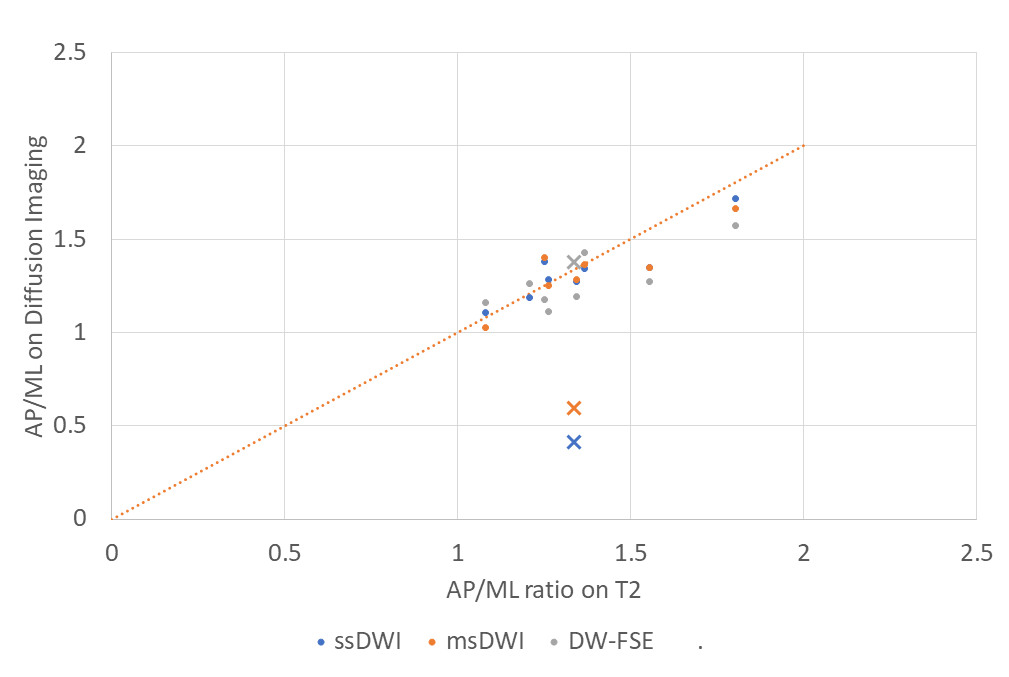
Figure 2. Ratio of anteroposterior measures of the prostate divided by mediolateral, with x axis corresponding to the T2 values and y axis values corresponding to ssDWI (blue), msDWI (orange), and DWI-FSE (grey). The “x” values correspond to the one case with a hip replacement, and show significant distortion for the ssDWI and msDWI sequences. The dotted orange line corresponds to x=y, the expected values for exact concordance of the AP/ML measurements between sequences.
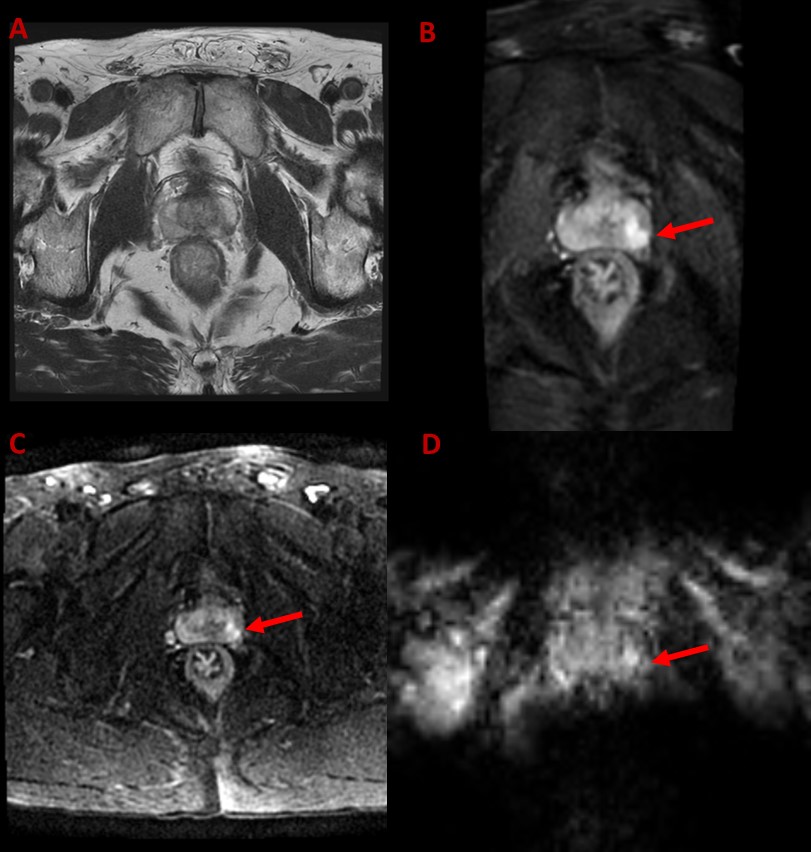
Figure 3. Prostate MRI of a patient with a left peripheral zone lesion, PI-RADS 4, clinically significant cancer is likely to be present. (A) Axial T2 FSE. (B) ssDWI with B=800s/mm2. (C) msDWI with B=800s/mm2. (D) DWI-FSE with B=800s/mm2.
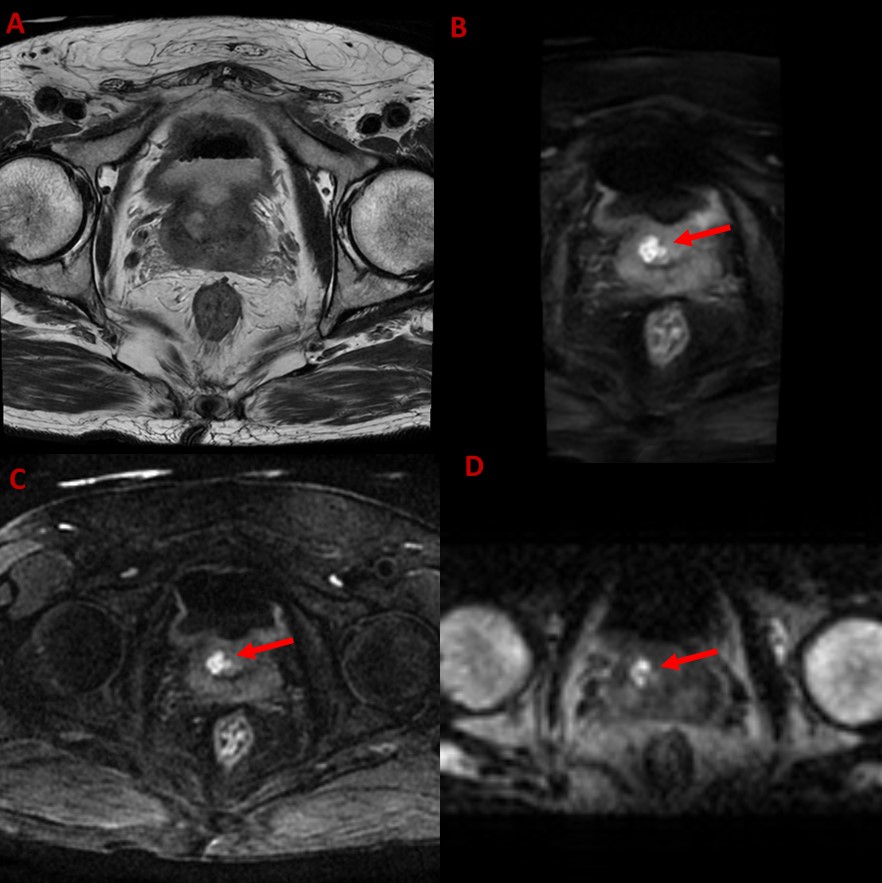
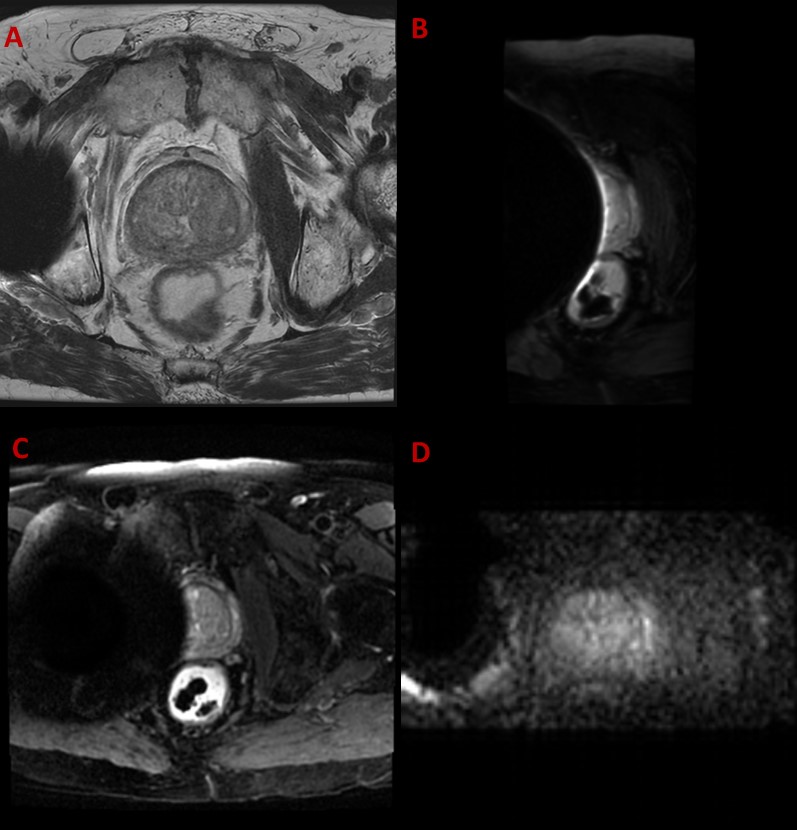
Figure 4. Prostate MRI of a patient with a right transition zone abscess. ADC value in the lesion measures 0.524 x 10-3 mm2/s on DWI-FSE, 0.697 x 10-3 mm2/s on ssDWI, and 0.627 x 10-3 mm2/s on msDWI. In the uninvolved prostate parenchyma, the ADC values measured 1.3 x 10-3 mm2/s on DWI-FSE, 1.317 x 10-3 mm2/s on ssDWI, and 1.354 x 10-3 mm2/s on msDWI. (A) Axial T2 FSE. (B) ssDWI with B=800s/mm2. (C) msDWI with B=800s/mm2. (D) DWI-FSE with B=800s/mm2.