3509
Diagnostic Value of Combined PI-RADS v2.1 and PSAD in Detecting Clinically Significant Prostate Cancer in the Gray Zone of PSA: A Dual-Center Study1Sixth Medical Center, Chinese PLA General Hospital, Beijing, China, 2First Medical Center, Chinese PLA General Hospital, Beijing, China
Synopsis
Keywords: Prostate, Prostate, Clinically Significant Prostate cancer,PSA density,PSA gray zone,PI-RADS v2.1
Motivation: It is crucial to improve the accuracy of detection of clinically significant prostate cancer (csPCa) within the PSA gray zone.
Goal(s): To combine PI-RADS v2.1 with prostate-specific antigen density(PSAD) derivatives to improve the predictive value of csPCa in the PSA gray zone.
Approach: Based on a dual-center study, logistic regression was used to analyze the predictive value of the multi-parameter combination on csPCa in the training group, the receiver operating characteristic curve(ROC) curves were used to evaluate the diagnostic performance, and conducting external validation.
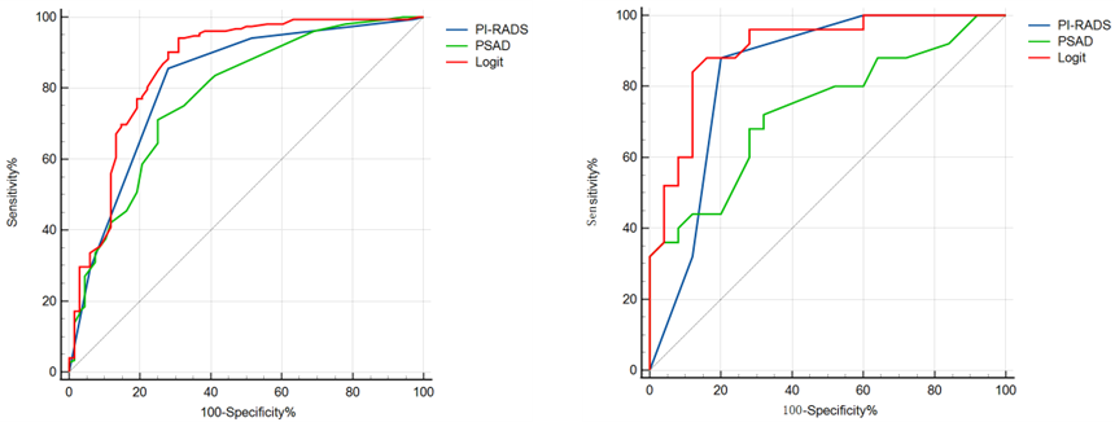
Results: The area under curve (AUC) of combining of PI-RADS v2.1 and PSAD was the highest for predicting csPCa.
Impact: The dual-center study demonstrates combining of PI-RADS v2.1 and PSAD improved the predictive performance of csPCa in the PSA gray zone, and grouping PSAD with PI-RADS risk stratification can have more direct clinical applications.
Prostate cancer (PCa) has a relatively high incidence worldwide.1-2 Currently, total prostate-specific antigen (tPSA) remains the preferred screening indicator for prostate cancer. However, tPSA has insufficient specificity, especially when tPSA levels are between 4-10 ng/ml, known as the diagnostic gray zone, resulting high false positives. where approximately 80% of patients may undergo unnecessary biopsies.3 It is unequivocally significant to improve the accuracy of detection for clinically significant prostate cancer (csPCa) in the PSA gray zone.
Multiparametric magnetic resonance imaging (mpMRI) of the prostate aids in the diagnosis of PCa in patients within the PSA gray zone.4-5 The Prostate Imaging Reporting and Data System (PI-RADS) has been widely accepted and applied in clinical practice since its release, and it effectively detects csPCa.5-6 In 2019, the PI-RADS v2.1 was released, which has higher diagnostic performance compared to v2.0.7 However, there have been only a few studies that have used PI-RADS v2.1 specifically for patients in the PSA gray zone. Prostate specific antigen density (PSAD) can improve the diagnostic accuracy of csPCa in the PSA gray zone.7 Studies have shown that combining of PI-RADS and PSAD improves the predictive performance of csPCa in the PSA gray zone, but most studies are single-center studies.
Objective Based on dual-center study, to investigate the diagnostic value of combining of PI-RADS v2.1 and PSAD for csPCa in the gray zone of PSA levels (4-10 ng/ml).
Materials and Methods We retrospectively collected 220 men that suspected prostate cancer patients in the PSA gray zone in Cohort 1. External cohort included 50 men that met our criteria. Two radiologists blinded to the clinical data reviewed MRI and scored the lesions according to the PI-RADS v2.1 guidelines. Cohort 1 was used as the training group, and an external cohort served as the testing group. Logistic regression was used to analyze the predictive value of the multi-parameter combination on csPCa. Receiver operating characteristic curves(ROC) were generated to evaluate the diagnostic performance and were validated in the testing group.
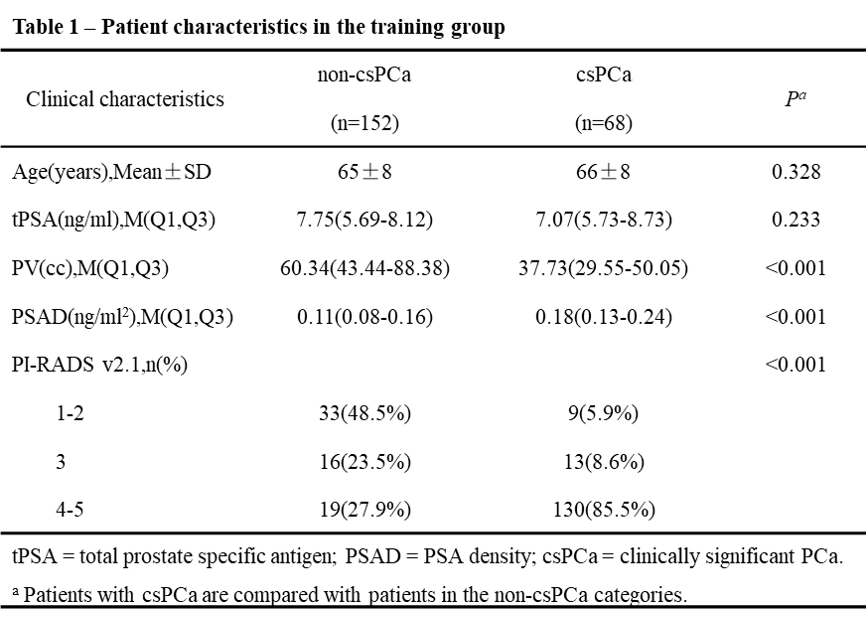
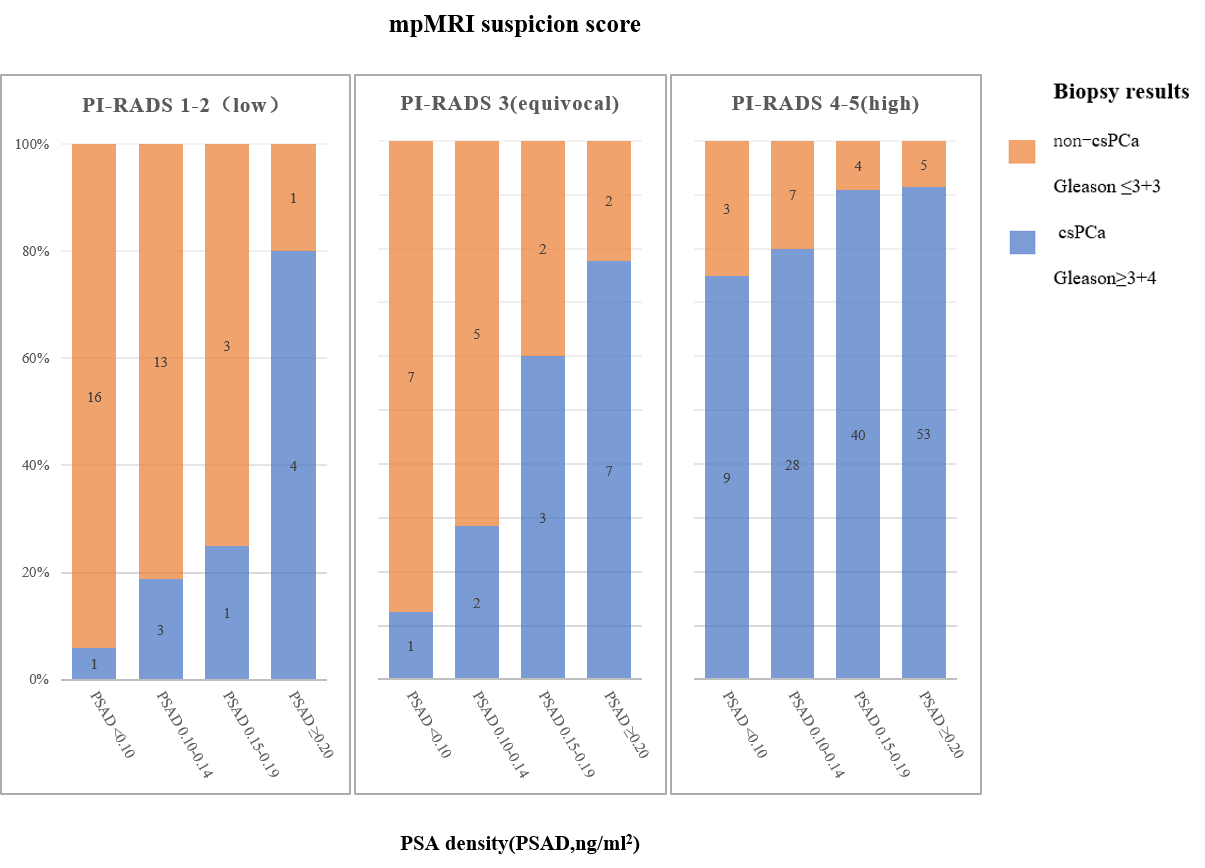
Results A total of 152 (69.1%) patients was diagnosed with csPCa in Cohort 1. Logistic regression analysis revealed that PSAD value and PI-RADS v2.1 score were predictive factors for the csPCa and non-csPCa. High area under the curve of the regression model was found in Cohort 1 and External cohort for csPCa (0.860 vs. 0.906). CsPCa detection rates were high when PI-RADS score 4-5 and PSAD≥0.15 ng/ml2 (91%-94%), while a lower detection rate of csPCa when the PI-RADS score≤2 and PSAD < 0.15 ng/ml2 (0%-12%).
Discussion
In our study, the prevalence of csPCa in the PSA gray zone ranged from 50% to 69%, which is higher than previous study.8-9 This could be due to differences in the population studied. Our dual-center study demonstrated that PI-RADS v2.1 and PSAD are independent predictive factors for predicting csPCa in the PSA gray zone, and their combined application can improve the diagnostic performance.
The PI-RADS score has been widely used in clinical practice, while effective, this approach cannot be directly used as a basis for biopsy or follow-up assessments. Although the PI-RADS v2.1 had an advantage in predicting csPCa in this study, achieving higher PPV in the training group compared to the study by Grey et al.10(86.7% vs. 58%). However, relying solely on PI-RADS to predict biopsy results has certain limitations. If the biopsy indication threshold was set at a PI-RADS score≥4, 14.47% of csPCa patients in our study's training group would be missed. Importantly, the diagnostic efficiency of combining PI-RADS and PSAD is higher than using either of them alone.
PSAD has been demonstrated in previous studies11-12 to be an independent predictive factor for csPCa in the PSA gray zone and can improve predictive accuracy. In our study, the optimal cutoff value for PSAD was 0.15 ng/ml2, with an AUC of 0.83 in the testing group, similar to the study by Zhang et al.13 Our study's PPV in the training group was higher than reported by Hu et al.14 (86% vs. 32%), possibly due to differences in csPCa prevalence in the study populations.
In the training group, if patients with PI-RADS 1-2 scores did not undergo biopsy, 21% of csPCa cases would be missed. However, when combined with PSAD <0.15 ng/ml2, this result decreased to 12%. We believe that grouping PSAD with PI-RADS risk stratification can have more direct clinical applications.
Conclusion PI-RADS v2.1 and PSAD are independent risk factors for predicting csPCa in the PSA gray zone. Combining the PI-RADS and PSAD improved the predictive performance of csPCa.
Acknowledgements
We acknowledge the financial support from the National Natural Science Foundation of China (Grant 81971580 and 82271951 and 81771785) and Beijing Municipal Natural Science Foundation (Grant 7222167) and The Sixth Medical Center of PLA General HospitalInnovation Cultivation Fund (Grant CXPY202107).References
1. SIEGEL R L, MILLER K D, WAGLE N S, et al. Cancer statistics, 2023[J]. CA: a cancer journal for clinicians, 2023, 73(1):17–48.
2. Cao W, Chen H-D, Yu Y-W, et al. Changing profiles of cancer burden worldwide and in China: a secondary analysis of the global cancer statistics 2020[J]. Chinese medical journal, 2021, 134(7):783–791. 3. Halpern JA, Oromendia C, Shoag JE, Mittal S, Cosiano MF, et al. Use of digital rectal examination as an adjunct to prostate-specific antigen in the detection of clinically significant prostate cancer. J Urol 2018; 199: 947–53.
4. Stabile A, Giganti F, Rosenkrantz A B, et al. Multiparametric MRI for prostate cancer diagnosis: current status and future directions[J]. Nature reviews. Urology, 2020, 17(1):41–61.
5. Li X, Li C, Chen M. Patients With "Gray Zone" PSA Levels: Application of Prostate MRI and MRS in the Diagnosis of Prostate Cancer[J]. Journal of magnetic resonance imaging : JMRI, 2023, 57(4):992–1010.
6. Tamada T, Kido A, Takeuchi M, et al. Comparison of PI-RADS version 2 and PI-RADS version 2.1 for the detection of transition zone prostate cancer. Eur J Radiol 2019;121:108704.
7. Nordström T, Akre O, Aly M, et al. Prostate-specific antigen (PSA) density in the diagnostic algorithm of prostate cancer[J]. Prostate cancer and prostatic diseases, 2018, 21(1):57–63.
8. Qi Y, Zhang S, Wei J, et al. Multiparametric MRI-Based Radiomics for Prostate Cancer Screening With PSA in 4-10 ng/mL to Reduce Unnecessary Biopsies[J]. Journal of magnetic resonance imaging : JMRI, 2020, 51(6):1890–1899.
9. Xu N, Wu Y-P, Chen D-N, et al. Can Prostate Imaging Reporting and Data System Version 2 reduce unnecessary prostate biopsies in men with PSA levels of 4-10 ng/ml?[J]. Journal of cancer research and clinical oncology, 2018, 144(5):987–995.
10. Grey A D R, Chana M S, Popert R, et al. Diagnostic accuracy of magnetic resonance imaging (MRI) prostate imaging reporting and data system (PI-RADS) scoring in a transperineal prostate biopsy setting[J]. BJU international, 2015, 115(5):728–735.
11. Aminsharifi A, Howard L, Wu Y, et al. Prostate Specific Antigen Density as a Predictor of Clinically Significant Prostate Cancer When the Prostate Specific Antigen is in the Diagnostic Gray Zone: Defining the Optimum Cutoff Point Stratified by Race and Body Mass Index[J]. The Journal of urology, 2018, 200(4):758–766.
12. Jue J S, Barboza M P, Prakash N S, et al. Re-examining Prostate-specific Antigen (PSA) Density: Defining the Optimal PSA Range and Patients for Using PSA Density to Predict Prostate Cancer Using Extended Template Biopsy[J]. Urology, 2017, 105:123–128.
13. Zhang C-C, Tu X, Lin T-H, et al. Combining clinical parameters and multiparametric magnetic resonance imaging to stratify biopsy-naïve men for an optimum diagnostic strategy with prostate-specific antigen 4 ng ml-1 to 10 ng ml-1[J]. Asian journal of andrology, 2022.
14. Hu C, Sun J, Xu Z, et al. Development and external validation of a novel nomogram to predict prostate cancer in biopsy-naïve patients with PSA <10 ng/ml and PI-RADS v2.1 = 3 lesions[J]. Cancer medicine, 2023, 12(3):2560–2571.
Figures