3506
The Efficacy of Short Repetition Time DWI in Highlighting Prostate Cancer1Radiology, Kawasaki Medical School, Okayama, Japan, 2Philips Japan, Tokyo, Japan, 3Radiology, Radiolonet Tokai, Nagoya, Japan, 4Urology, Kawasaki Medical School, Okayama, Japan
Synopsis
Keywords: Prostate, Prostate, apparent diffusion coefficient; repetition time; diffusion-weighted imaging; magnetic resonance imaging; prostate cancer
Motivation: Assessing whether short repetition time (TR) diffusion-weighted imaging (DWI) surpasses conventional long TR DWI for prostate cancer detection.
Goal(s): To compare the image quality and diagnostic accuracy of short TR DWI to long TR DWI using a 3.0-Tesla MRI.
Approach: Twenty-five prostate cancer patients were imaged with both short (1850 ms) and long (6000 ms) TR DWI. We analyzed signal-to-noise ratio (SNR), contrast-to-noise ratio (CNR), and apparent diffusion coefficient (ADC), with additional qualitative diagnostic assessments.
Results: Short TR DWI yielded higher CNR and visual scores with stable SNR, alongside robust ADC correlations, enhancing diagnostic performance notably for non-specialist readers.
Impact: Short repetition time diffusion-weighted imaging's improved prostate cancer detection could enhance diagnostic performance for non-specialist readers, influencing treatment and patient outcomes. It invites new magnetic resonance imaging research and may transform standard prostate cancer diagnostic protocols, reducing unnecessary invasive procedures.
INTRODUCTION
The struggle against prostate cancer (PCa), a pervasive health concern, continues to be a challenge due to diagnostic complexities, specifically in the precise characterization and staging of lesions. biparametric MRI assesses prostate lesions through diffusion-weighted imaging (DWI), Apparent Diffusion Coefficient (ADC) maps, and T2-weighted (T2WI). DWI and ADC are pivotal due to their high lesion contrast in the prostate1,2. However, the efficacy of conventional DWI in PCa detection can be hindered by suboptimal signal-to-noise (SNR) and contrast-to-noise ratios (CNR), especially at certain b-values1-7. Our study introduces 'short TR DWI,' an advanced imaging approach designed to boost diffusion contrast, particularly in instances where long TR DWI yields uncertain results. This method exploits the unique lower T1 values inherent to PCa compared to surrounding tissues8-12, aiming to refine both the visibility of lesions and the overall diagnostic accuracy for clinicians.METHODS
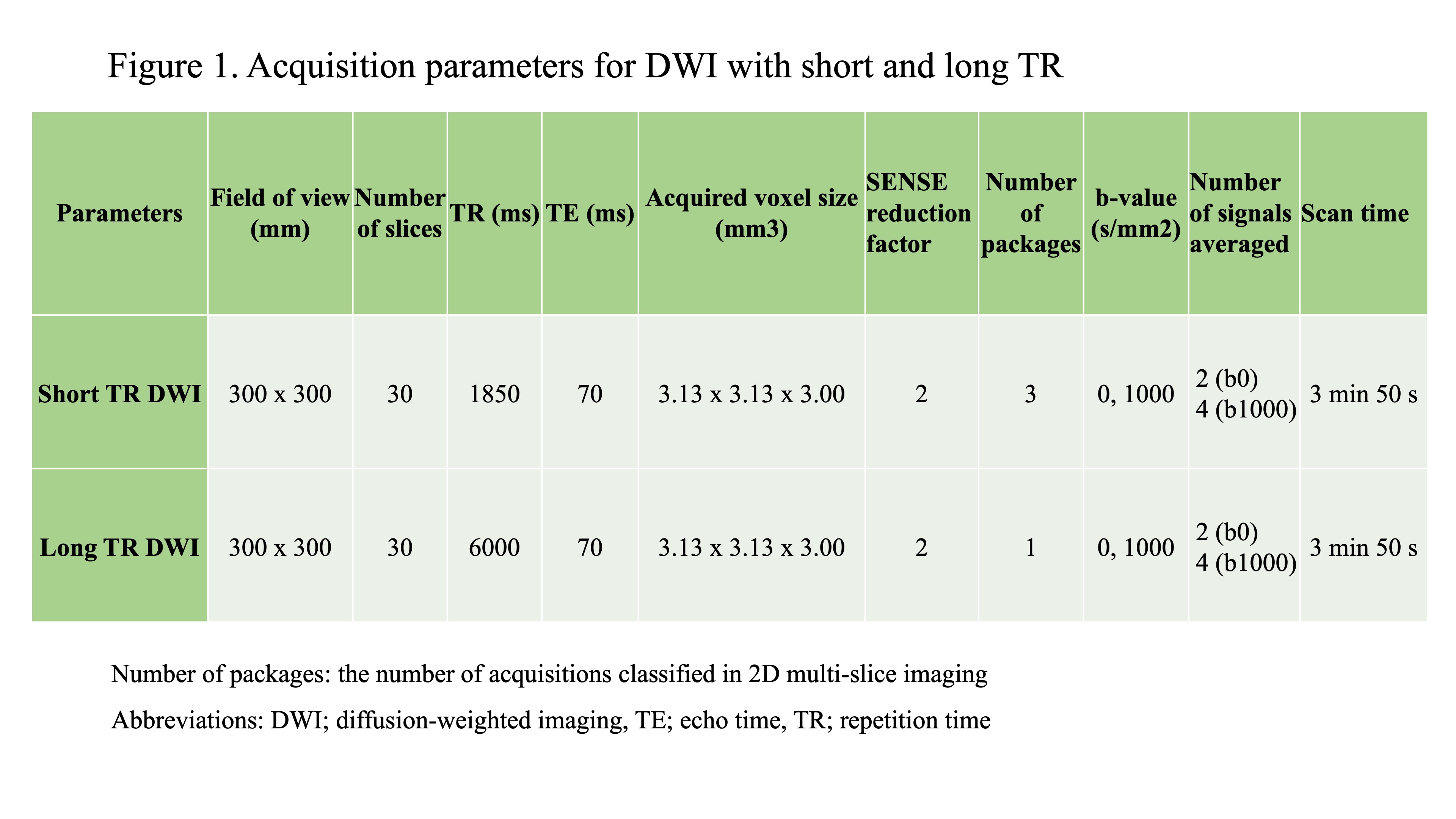
This study enrolled a cohort of twenty-five patients with histologically proven PCa. This study's MRI procedures were conducted using a 3.0-Tesla MRI system (Ingenia 3.0T CX; Philips Healthcare), equipped with both anterior and integrated posterior coils. The imaging suite included DWI at b-values of 0 and 1000, T1 mapping, and T2WI, which were pertinent for evaluating prostate cancer lesions, pinpointing their anatomical position, and measuring T1 values, respectively. For DWI, we employed spin-echo type single-shot echo planar imaging with two repetition times: a short TR of 1850 ms and a standard long TR of 6000 ms, the latter being the conventional protocol in our institution and serving as the benchmark for this research. The detailed parameters for these DWI sequences are catalogued in Figure1. Our primary metrics for comparison were the SNR, CNR, visual assessment score, ADC, and overall diagnostic performance. We applied paired t-tests for SNR and CNR evaluations, the Wilcoxon signed-rank test for visual assessment, Pearson’s correlation and Bland–Altman plots for analyzing ADC values, and for diagnostic performance, the McNemar test along with receiver operating characteristic (ROC) analysis and Delong test were utilized.RESULTS
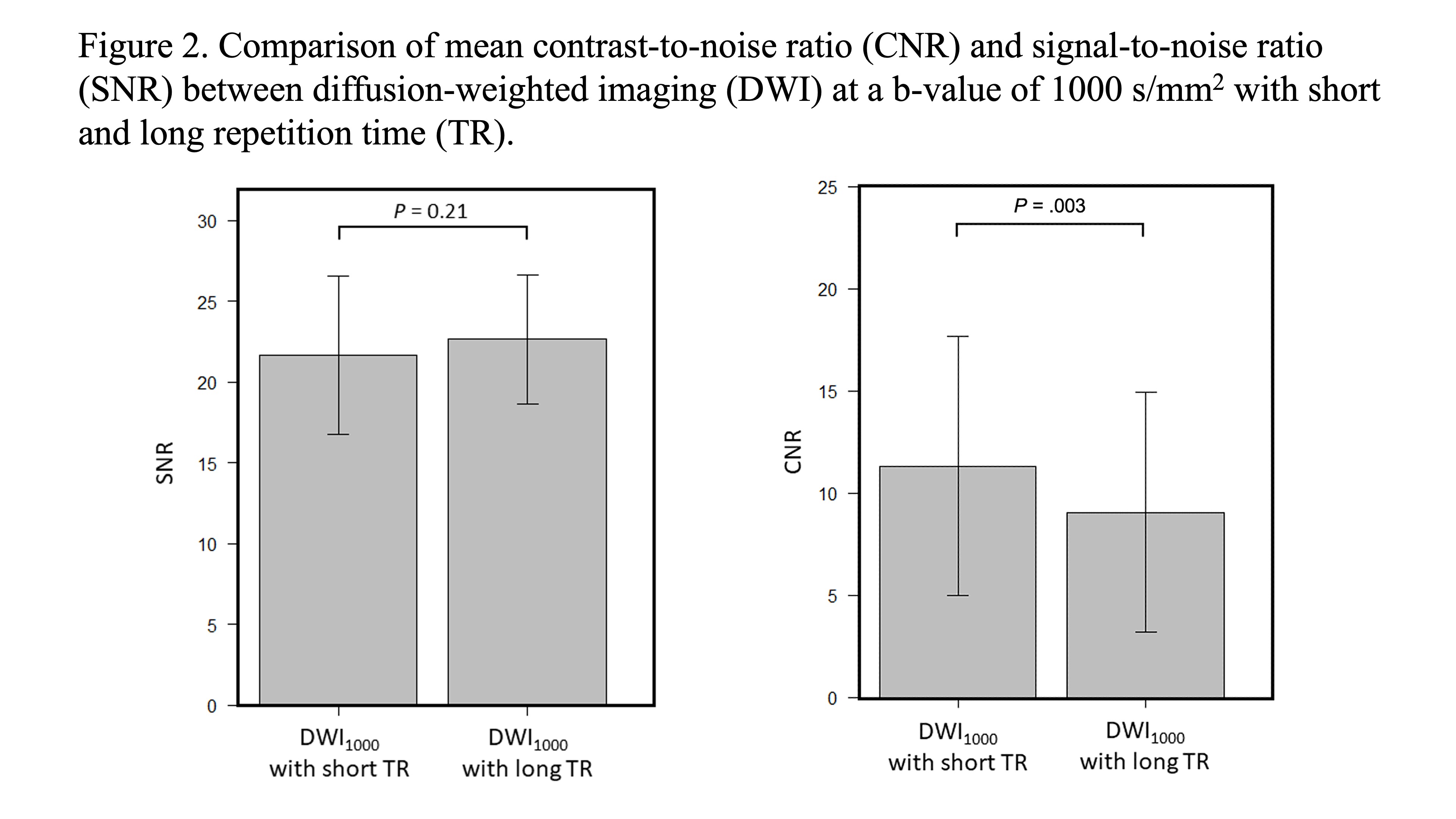
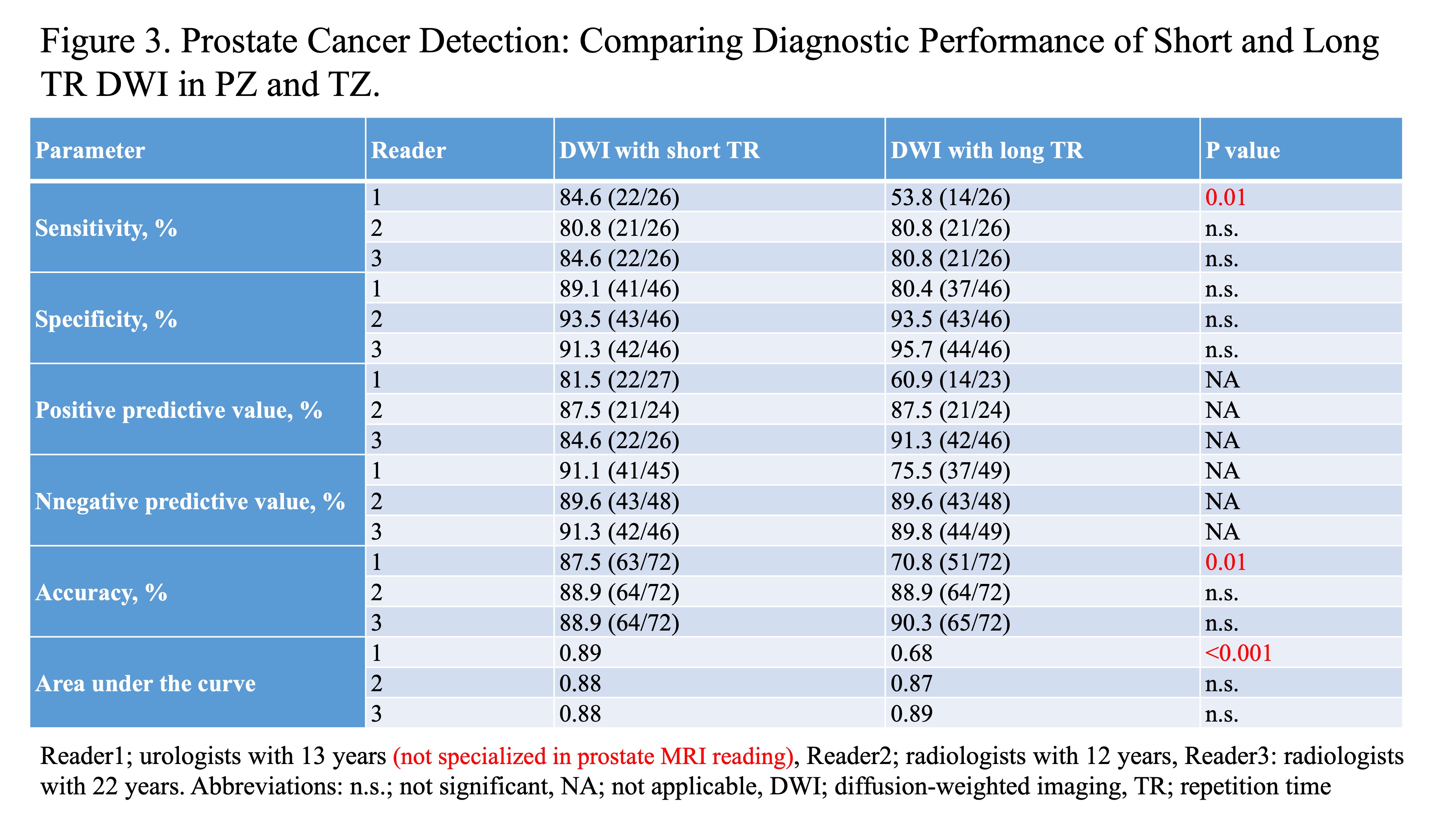
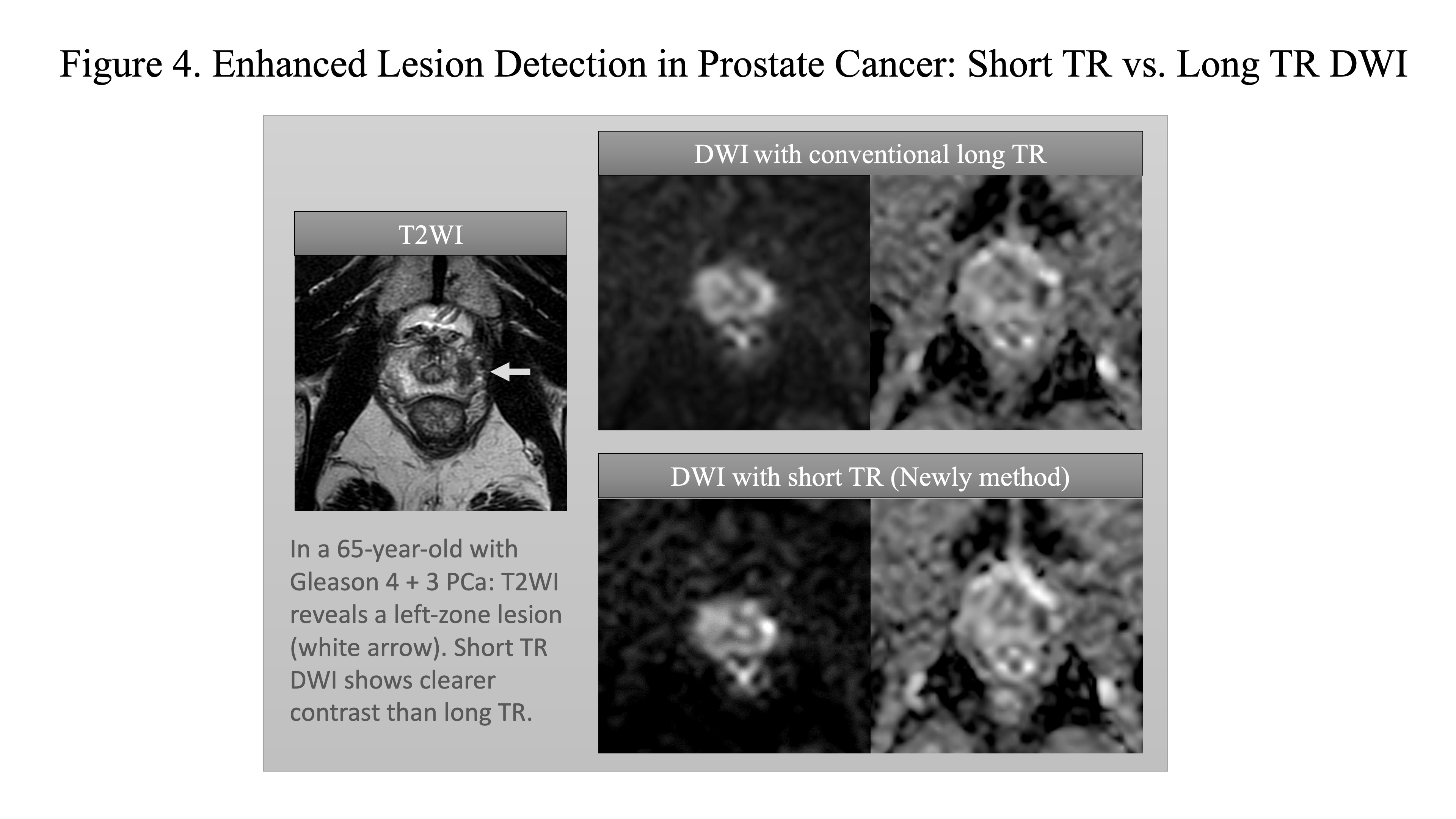
Upon analyzing the image sets, it became evident that the short TR DWI configuration delivered a markedly superior contrast-to-noise ratio and visual assessment scores at the b1000 level (P = .003 and P = .002, respectively), in stark contrast to the SNR, which remained equivalently distributed between both TR settings (P = .21) (Figure2). The fidelity of ADC measurements was affirmed by strong correlations between short and long TR sequences, underscoring a reliable diffusion assessment irrespective of TR length. The mean T1 value in PCa was significantly lower than that in NPT (P = .002). In a comparison of diagnostic performance by three readers using PI-RADS v2.1 DWI scores, two (radiologists) found the short TR DWI equivalent to the long TR DWI, while one reader (urologist, Non-specialist Reader) showed significantly higher sensitivity, accuracy, and diagnostic performance with short TR DWI (Figure3). Representative images are shown in Figure 4.DISCUSSION
The superior performance of short TR DWI can be ascribed to two primary influences: the enhanced magnetization transfer effect owing to an increased number of packages and the intrinsically shorter T1 values in PCa tissues, as opposed to normal prostatic tissue (NPT), which promotes greater signal distinction. Our research intimates that short TR DWI furnishes superior image quality and might increase the diagnostic performance. The virtue of short TR DWI lies in its adaptability, as it can be seamlessly incorporated into the protocols of most MRI facilities without necessitating specialized software or intricate techniques. Importantly, our findings suggest that short TR DWI may enhance diagnostic performance for readers not specialized in prostate MRI interpretation. The limitations of our study, including its retrospective nature, limited cohort size, and singular institutional perspective, must be acknowledged as they may influence the broad applicability of our results.CONCLUSION
Short TR DWI has emerged as a significant innovation for augmenting diffusion contrast in the MRI evaluation of PCa, surpassing traditional long TR DWI. This novel technique could substantially improve PCa visualization, thereby influencing clinical decision-making and patient care strategies, with particular benefits for non-specialist readers in enhancing diagnostic performance. Its integration may also refine computed DWI procedures. While promising, these initial findings necessitate further confirmation through broader studies. Future investigations should also aim to optimize additional imaging parameters, like echo time (TE), to further amplify the contrast and detection of PCa.Acknowledgements
No acknowledgement found.References
1. Barentsz JO, Richenberg J, Clements R, et al. ESUR prostate MR guidelines 2012. Eur Radiol. 2012;22(4):746–57.
2. Turkbey B, Rosenkrantz AB, Haider MA, et al. Prostate imaging reporting and data system. version 2.1: 2019 Update of Prostate Imaging Reporting and Data System. version2. Eur Urol. 2019;76(3):340–51.
3. Bratan F, Niaf E, Melodelima C, et al. Influence of imaging and histological factors on prostate cancer detection and localisation on multiparametric MRI: a prospective study. Eur Radiol. 2013;23(7):2019–29.
4. Kido A, Tamada T, Kanomata N, et al. Multidimensional analysis of clinicopathological characteristics of false-negative clinically significant prostate cancers on multiparametric MRI of the prostate in Japanese men. Jpn J Radiol. 2019;37(2):154–64.
5. Ahmed HU, El-Shater Bosaily A, Brown LC, et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (Promis): a paired validating confirmatory study. Lancet. 2017;389(10071):815–22.
6. Delongchamps NB, Lefèvre A, Bouazza N, et al. Detection of significant prostate cancer with magnetic resonance targeted biopsies – should transrectal ultrasound-magnetic resonance imaging fusion guided biopsies alone be a standard of care? J Urol. 2015. 193(4):1198-204
7. Schoots IG, Roobol MJ, Nieboer D, et al. Magnetic resonance imaging-targeted biopsy may enhance the diagnostic accuracy of significant prostate cancer detection compared to standard transrectal ultrasound-guided biopsy: a systematic review and meta-analysis. Eur Urol. 2015;68(3):438–50.
8. Baur ADJ, Hansen CM, Rogasch J, et al. Evaluation of T1 relaxation time in prostate cancer and benign prostate tissue using a Modified Look-Locker inversion recovery sequence. Sci Rep. 2020;10(1):3121.
9. Panda A, Obmann VC, Lo WC, et al. MR fingerprinting and ADC mapping for characterization of lesions in the transition zone of the prostate gland. Radiology. 2019;292(3):685–94.
10. Arita Y, Akita H, Fujiwara H, et al. Synthetic magnetic resonance imaging for primary prostate cancer evaluation: diagnostic potential of a non-contrast-enhanced bi-parametric approach enhanced with relaxometry measurements. Eur J Radiol Open. 2022;9:100403.
11. Al-Bourini O, Seif Amir Hosseini A, Giganti F, et al. T1 mapping of the prostate using single-shot T1FLASH: a clinical feasibility study to optimize prostate cancer assessment. Invest Radiol. 2023;58(6):380–7.
12. Yu AC, Badve C, Ponsky LE, Pahwa S, Dastmalchian S, Rogers M, et al. Development of a combined MR fingerprinting and diffusion examination for prostate cancer. Radiology. 2017;283(3):729–38. https://doi.org/10.1148/radiol.2017161599
Figures
Figure
1. Acquisition
parameters for DWI with short and long TR
Number
of packages: the number of acquisitions classified in 2D multi-slice imaging
Abbreviations: DWI; diffusion-weighted imaging, TE; echo time, TR; repetition time