3498
Time-dependent diffusion MRI for quantitative microstructural mapping of common brain tumors1Radiology, Sichuan Cancer Hospital & Institute,Affiliated Cancer Hospital of University of Electronic Science and Technology of China, Chengdu, China, 2MR Research Collaboration, Siemens Healthineers, chengdu, China, 3MR Research Collaboration, Siemens Healthineers, Shanghai, China
Synopsis
Keywords: Diffusion Modeling, Tumor, OGSE
Motivation: Different clinical managements are required for brain tumors such as glioblastoma, meningioma and metastases, with existing MRI techniques showing limitations in distinguishing them.
Goal(s): The study aims to validate the utility of td-dMRI to enhance the accuracy of brain tumors characterization, using the IMPULSED model to distinguish microstructural distinctions.
Approach: We used td-dMRI to explore microstructural mapping in glioblastoma, meningioma, and lung cancer patients with brain metastases by IMPULSED model, focusing on the parameters Dex, d, and vin to differentiate these brain tumors.
Results: The cell size and extracellular diffusivity of these tumors are distinctly different.
Impact: This study demonstrated that td-dMRI can non-invasively differentiate between glioblastomas, meningiomas and metastases. It proposes a potential change in diagnostic protocols, offering a pathway to more personalized management while reducing reliance on contrast agents.
Introduction
Accurate diagnostic differentiation among glioblastomas, meningiomas, and metastatic brain tumors is crucial, given that management differs for these tumors, timely and accurate identification is imperative. However, conventional magnetic resonance imaging (MRI) often reaches its limits when attempting to distinguish between these lesions due to appearing similar on conventional MRI. Optimized dynamic susceptibility contrast-enhanced (DSC) MRI protocols have been developed to distinguish between meningiomas and glioblastomas, as well as glioblastomas and metastases, with each protocol tailored to specific tumor characteristics1,2. However, a universally enhanced-MRI protocol for concurrently identifying all three tumors has rarely been established. Additionally, enhanced-MRI requires the administration of contrast agents, increasing burden of metabolism for patients. Many researchers have incorporated diffusion-weighted imaging (DWI) to distinguish among these tumors. However, reported apparent diffusion coefficient (ADC) values of the tumor parenchymal area and the peritumoral edema revealed conflicting results3,4. Recently, time-dependent diffusion magnetic resonance imaging (td-dMRI) has emerged as a technique capable of revealing microstructural details of brain tumors, such as cell size and cellularity5. So this paper aimed to explore the value of td-dMRI in the accurate identification of glioblastomas, meningiomas and metastases through microstructural imaging.Methods
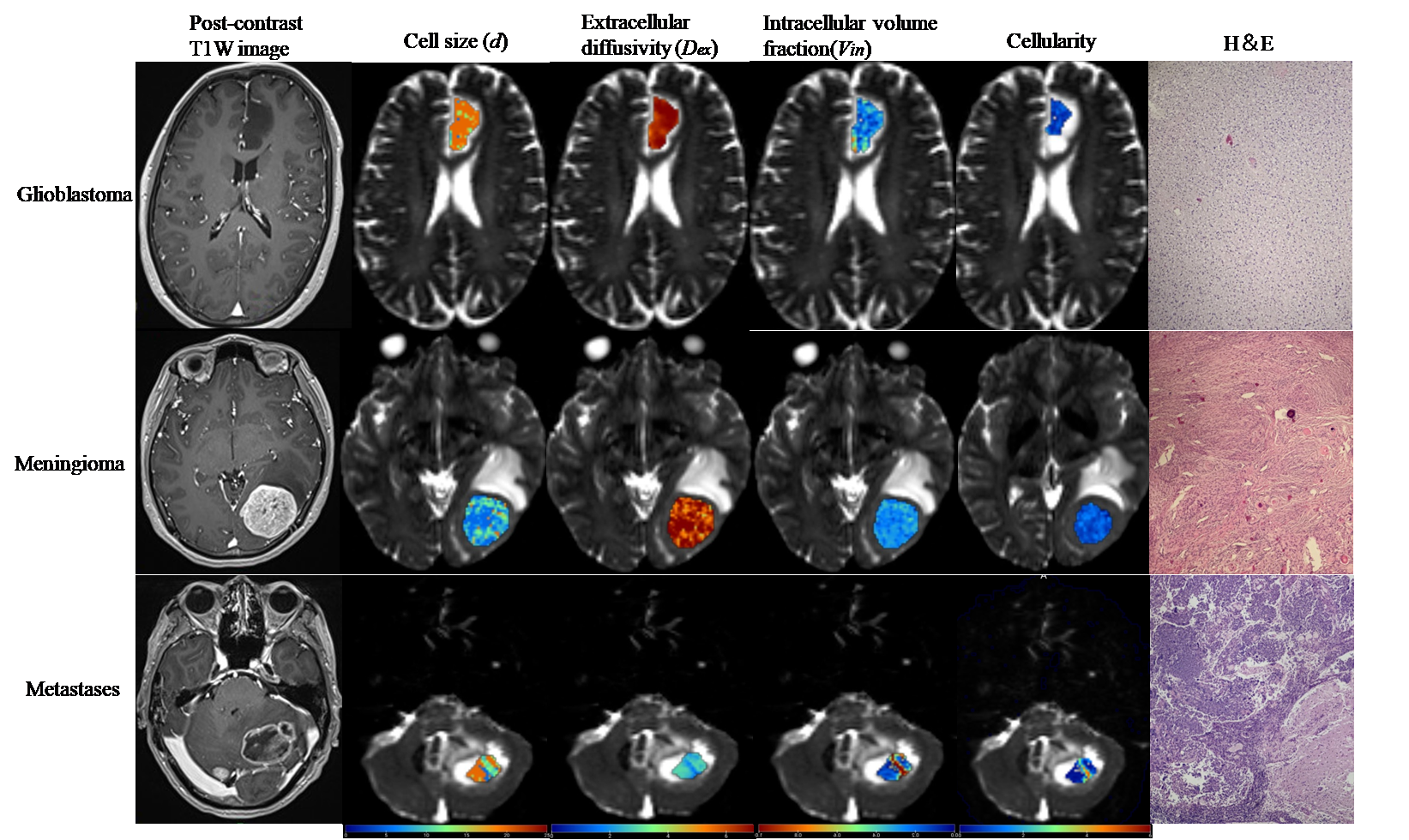
MR imaging: This retrospective study included 29 patients: 7patients with glioblastomas, aged 51.73±14.89 years, 11patients with meningiomas, aged 59.36 ±5.03years, and 11 lung cancer patients with brain metastases, aged 51.71 ± 8.16 years, who underwent td-dMRI on a 3T scanner (MAGNETOM Skyra, Siemens Healthineers, Erlangen, Germany) with a 16-channel head coil. The MRI protocol integrated oscillating gradient spin-echo (OGSE) and pulsed gradient spin-echo (PGSE) research sequences. OGSE operated at 35Hz and 20Hz, with effective diffusion times of 5.2 msec (b-values: 0, 350, 515 sec/mm2) and 8.8 msec (b-values: 0, 400, 1000 sec/mm2), respectively. The PGSE sequence was applied with an effective diffusion time of 55 msec, with b-values of 0, 400, and 1000 sec/mm2. Both sequences were harmonized to the following parameters: three diffusion directions, repetition time/echo time = 4900/162 ms, field of view = 204×204 mm2, in-plane resolution = 1.6×1.6 mm2, slices = 6, and section thickness = 5mm. The total scanning time for this td-dMRI protocol was approximately 7.5 minutes. DSC-MRI protocols were acquired for anatomical reference6.Reconstruction & Segmentation: The td-dMRI data are processed through the imaging microstructural parameters using limited spectrally edited diffusion (IMPULSED) model to compute the parameters4, including extracellular diffusivity (Dex), volume-weighted mean cell size (d), intracellular volume fraction (vin), and cellularity. The initial value of intracellular diffusivity (Din) was set at 1.5 µm2/ms for stability. Constraints were applied to IMPULSED model based on physiological plausibility: 0.2< d<20 μm, 0< vin<1, and 0< Dex<3 μm2/ms. Fitting of IMPULSED model was performed using the least square curve fitting toolbox in MATLAB (MathWorks, Inc.). The regions of interest of tumor parenchymal area were manually delineated on each slice based on PGSE image after being aligned with the DCE-MRI images by an experienced radiologist, excluding necrotic areas and surrounding tissue.
Statistical Analysis: All statistical analysis was performed using SPSS, version 23 (IBM, Chicago), and a P value less than 0.05 was accepted as significance. The differences in parameters among glioblastomas, meningiomas and metastases were assessed using one-way analysis of variance (ANOVA), followed by the post hoc Tamhane test used for dual group comparisons.
Results
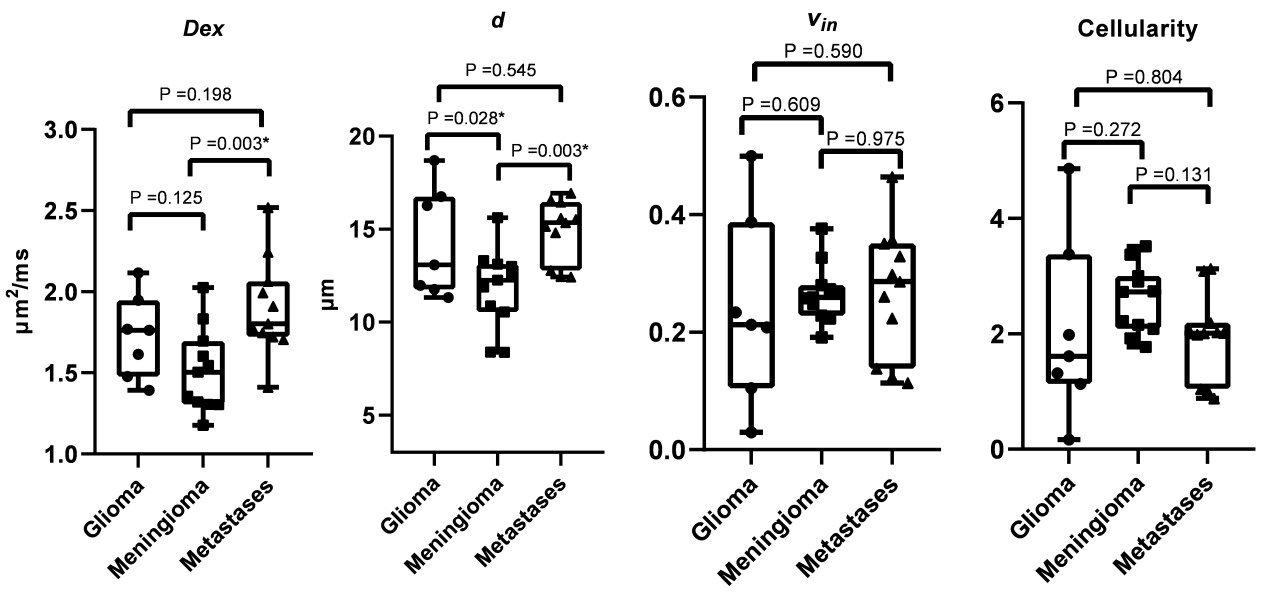
Figure 1 shows the microstructural mapping results using the td-dMRI in three representative cases. The mean values of Dex, d, vin and cellularity for each tumor type are summarized in Table 1. Compared with glioblastomas and metastases, meningiomas showed significantly lower values of d, and compared with metastases, meningiomas showed significantly lower values of Dex (all P< 0.05)(Figure 2).Discussion and Conclusion
This study demonstrated the potential of td-dMRI to provide enhanced diagnostic accuracy through microstructural imaging. The underlying mechanism for the higher Dex in brain metastases than in meningioma may be that the brain metastases are more prone to liquefaction and necrosis and have faster cell proliferation7.Our sample size was small, which limited the statistical power and might lead to false negative. Future research will aim to broaden the dataset and examine additional parameters, including ADC from OGSE image, to enhance the robustness and diagnostic utility of td-dMRI in tumor identification. Also, the combination of td-dMRI with other imaging modalities, such as molecular imaging or perfusion MRI, may also enhance our ability to noninvasively differentiate the three brain tumors.Acknowledgements
No acknowledgement found.References
1. Pantelis G, Dionisis , Ioannis K, at al. Improving brain tumor characterization on MRI by probabilistic neural networks and non-linear transformation of textural features. Comput Meth Prog Bio. 2008;89(1):24-32.
2. Lee MD, Baird GL, Bell LC, at al. Utility of Percentage Signal Recovery and Baseline Signal in DSC-MRI Optimized for Relative CBV Measurement for Differentiating Glioblastoma, Lymphoma, Metastasis, and Meningioma. Am J Neuroradiol. 2019;40(9):1445-1450.
3. Cindil E, Sendur HN, Cerit MN, at al. Validation of combined use of DWI and percentage signal recovery-optimized protocol of DSC-MRI in differentiation of high-grade glioma, metastasis, and lymphoma. Neuroradiology.2021;63:331–342.
4. Zhang G, Chen X, Zhang S, et al. Discrimination between solitary brain metastasis and glioblastoma multiforme by using ADC-based texture analysis: a comparison of two different ROI placements. Acad Radiol. 2019;26:1466–72.
5. Xu J, Jiang X, Li H, et al. Magnetic resonance imaging of mean cell size in human breast tumors. Magn Reson Med. 2020;83:2002-2014.
6. Cindil E, Sendur HN, Cerit MN, et al. Validation of combined use of DWI and percentage signal recovery-optimized protocol of DSC-MRI in differentiation of high-grade glioma, metastasis, and lymphoma. Neuroradiology. 2021;63:331–42.
7. Ricardo McFaline-Figueroa J & Eudocia Q Lee. Brain tumors. Am J Med. 2018 Aug;131(8):874-882.
Figures