3494
MAP-MRI: a Potential Tool for Investigating Pathophysiological Mechanisms in Pediatric Basic Intermittent Exotropia1School of Medicine, The Chinese University of Hong Kong, Shenzhen, Shenzhen, China, 2Shenzhen Research Institute of Big Data, Shenzhen, China, 3The Chinese University of Hong Kong, Shenzhen, Shenzhen, China, 4School of Computer Science and Engineering, Beihang University, Beijing, China, 5MR Research Collaboration, Siemens Healthineers Ltd., Beijing, China, 6Beijing Tongren Hospital, Capital Medical University, Beijing, China
Synopsis
Keywords: Diffusion Modeling, Diffusion/other diffusion imaging techniques, MAPMRI
Motivation: To better understand the pathophysiological progression mechanism of childhood basic-type IXT and develop an accurate approach for early diagnosis.
Goal(s): To find a valuable tool in reflecting the pathological changes of the visual center pathway in IXT children.
Approach: A voxel-wise analysis was performed for MAPMRI-derived parameters between IXT patients and health controls, and a DTI analysis was used as reference.
Impact: We firstly explored MAPMRI’s value in detecting abnormal pathological changes of the primary and higher visual center, and the ocular movement pathway in children with basic IXT. This discovery enhances comprehension of IXT's pathology and offers insights for early diagnosis.
Introduction
Intermittent exotropia (IXT) is the most prevalent type of exotropia in childhood, characterized by intermittent outward deviation of one or both eyes[1], bringing a considerable burden on affected individuals and society. Untreated childhood-onset IXT can deteriorate over time, potentially progressing into constant exotropia[1, 2], ultimately resulting in a decline in binocular or monocular visual function in certain cases[3]. However, early and accurate diagnosis of childhood basic-type IXT remains challenging. Recent clinical diagnosis of IXT is assessed by binocular sensory status (fusion and stereopsis) and binocular motor alignment[3], and Newcastle Control Score grades the severity of IXT[4], but misdiagnosis frequently occurs because of the intermittent nature of IXT and the limited competency of children to cooperate with the eye examinations[5]. Recent MRI studies have found abnormal morphological changes in the cerebral cortex[6] and functional changes in neural activity in brain regions responsible for controlling eye movements and binocular fusion in IXT children[7, 8], which suggests cortical changes is a worthwhile direction for developing better diagnosis method. However, the underlying mechanism of progression in IXT still awaits determination. Mean Apparent Propagator (MAP) MRI is an advanced diffusion imaging technique renowned for its precision in mapping tissue microstructure, which has more advantages such as improved resolution, sensitivity, and specificity compared to preexisting methods, especially conventional diffusion imaging techniques.[9] In this study, we first utilize MAPMRI to observe microstructural alterations in the visual and ocular motor pathways of children with basic-type IXT. A correlation study was also performed to better understand the pathophysiology of IXT and to develop an early and accurate diagnostic approach. Conventional DTI imaging was used as reference.Methods
MRI data, T1-weighted, and diffusion-weighted scans were obtained from 31 children and adolescent IXT patients and 37 healthy controls. Ophthalmic examinations and neuropsychology scale study were assessed in both groups. MAPMRI and DTI parameter maps were produced from the diffusion-weighted scans. The MAPMRI parameters investigated included mean square displacement (MSD), nonGaussianity (NG), non-Gaussianity axial (NGAx), non-Gaussianity vertical (NGRad), Q-space inverse variance (QIV), return to the origin probability (RTOP), return to the axis probability (RTAP), and return to the plane probability (RTPP).Results
Compared to HC group, the IXT group showed significantly different MAPMRI parameter maps in the following brain regions (p<0.01), shown in Table 1. MSD, RTAP, RTOP, and NG value decreased significantly in right middle occipital gyrus and right superior occipital gyrus. MSD, RTAP, and RTOP value decreased significantly in right inferior occipital gyrus and right middle temporal gyrus. MSD value decreased in left superior occipital gyrus, right and left supplementary motor area. RTAP, RTOP, RTPP, NG, NGax, and NGrad value decreased in left middle occipital gyrus. RTOP value decreased in left calcarine fissure. QIV, RTAP, and RTOP value decreased in left superior frontal gyrus (orbital part). QIV value decreased in left middle frontal gyrus (orbital part). Compared to HC group, the IXT group also showed different DTI parameter maps in the following brain regions, shown in Table 1. MD value decreased in left middle occipital gyrus, left calcarine fissure, left superior frontal gyrus (orbital part), left middle frontal gyrus (orbital part), left supplementary motor area, right supplementary motor area, left inferior occipital gyrus, and right superior frontal gyrus (dorsolateral). FA value decreased in left and right supplementary motor area.Brain regions (right and left precuneus) where MAPMRI parameters were significantly correlated with clinical characteristics in IXT patients were shown in Table 2.
Discussion
The findings of decreased MAPMRI parameters in multiple brain regions in IXT patients suggests cortical microstructure changes in primary visual center, advanced visual center, and eye movement center pathways in children with basic-type IXT, consistent with previous hypothesis of the progression mechanism of IXT[8]. Decreased RTOP value in left calcarine fissure suggests the abnormal microstructural changes in primary visual cortex. Decreased multiple MAPMRI parameters in right middle occipital gyrus, right superior occipital gyrus, right inferior occipital gyrus, right middle temporal gyrus, left superior occipital gyrus, and left middle occipital gyrus indicates the abnormal microstructural changes in advanced visual cortex. Decreased QIV value in left middle frontal gyrus (orbital part) and decreased QIV, RTAP, and RTOP value in left superior frontal gyrus (orbital part) suggests the abnormal microstructural changes in eye movement center. Although both DTI and MAPMRI found abnormal brain changes, MAPMRI found more abnormal brain regions compared to DTI, highlighting its advantages of improved resolution, sensitivity, and specificity. According to the associations between clinical characteristics and MAPMRI parameters, MAPMRI showed clinical feasibility in the application of diagnosis of IXT.Acknowledgements
No acknowledgement found.References
1. Pediatric Eye Disease Investigator, G., et al., Three-Year Observation of Children 3 to 10 Years of Age with Untreated Intermittent Exotropia. Ophthalmology, 2019. 126(9): p. 1249-1260.
2. Cotter, S.A., et al., Three-year observation of children 12 to 35 months old with untreated intermittent exotropia. Ophthalmic Physiol Opt, 2020. 40(2): p. 202-215.
3. Sprunger, D.T., et al., Esotropia and Exotropia Preferred Practice Pattern(R). Ophthalmology, 2023. 130(3): p. P179-P221.
4. Haggerty, H., et al., The Newcastle Control Score: a new method of grading the severity of intermittent distance exotropia. Br J Ophthalmol, 2004. 88(2): p. 233-5.
5. Liu, Y., et al.,Diagnosis and treatment of intermittent exotropia based on the Preferred Practice Pattern of the United States. Chin J Ophthalmol and Otorhinolaryngol, 2019. 19(01): p. 6-8.
6. Wang, X., et al., Abnormal cortical morphology in children and adolescents with intermittent exotropia. Front Neurosci, 2022. 16: p. 923213.
7. Zhu, H., et al., Structural and Functional Changes of Brain in Children With Intermittent Exotropia: A Study Combining Multiple MRI Modalities. J Neuroophthalmol, 2023.
8. Fei, N., et al., Structural and spontaneous functional brain changes in visual and oculomotor areas identified by functional localization task in intermittent exotropia children. Brain Res, 2023. 1819: p. 148543.
9. Ozarslan, E., et al., Mean apparent propagator (MAP) MRI: a novel diffusion imaging method for mapping tissue microstructure. Neuroimage, 2013. 78: p. 16-32.
Figures
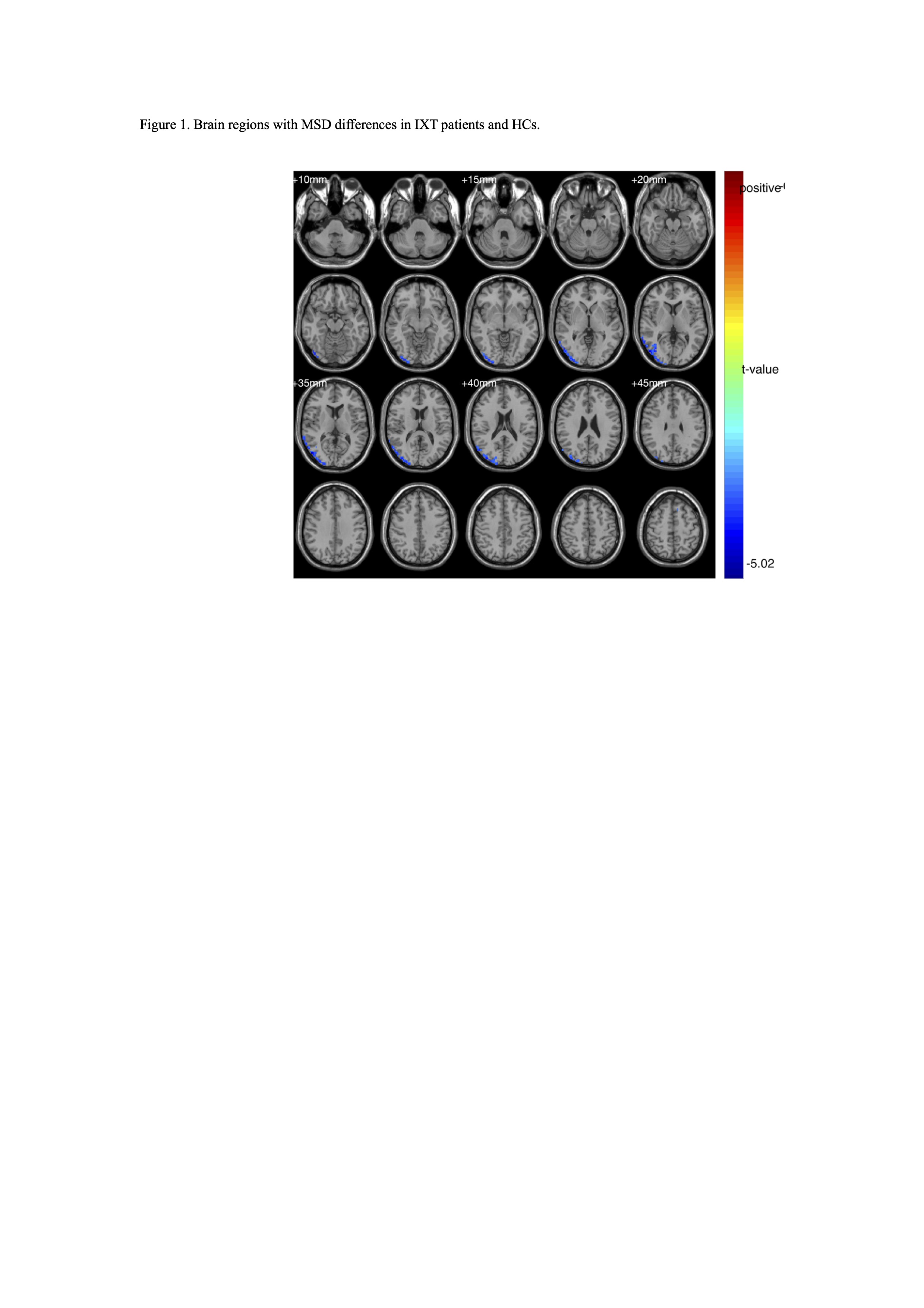
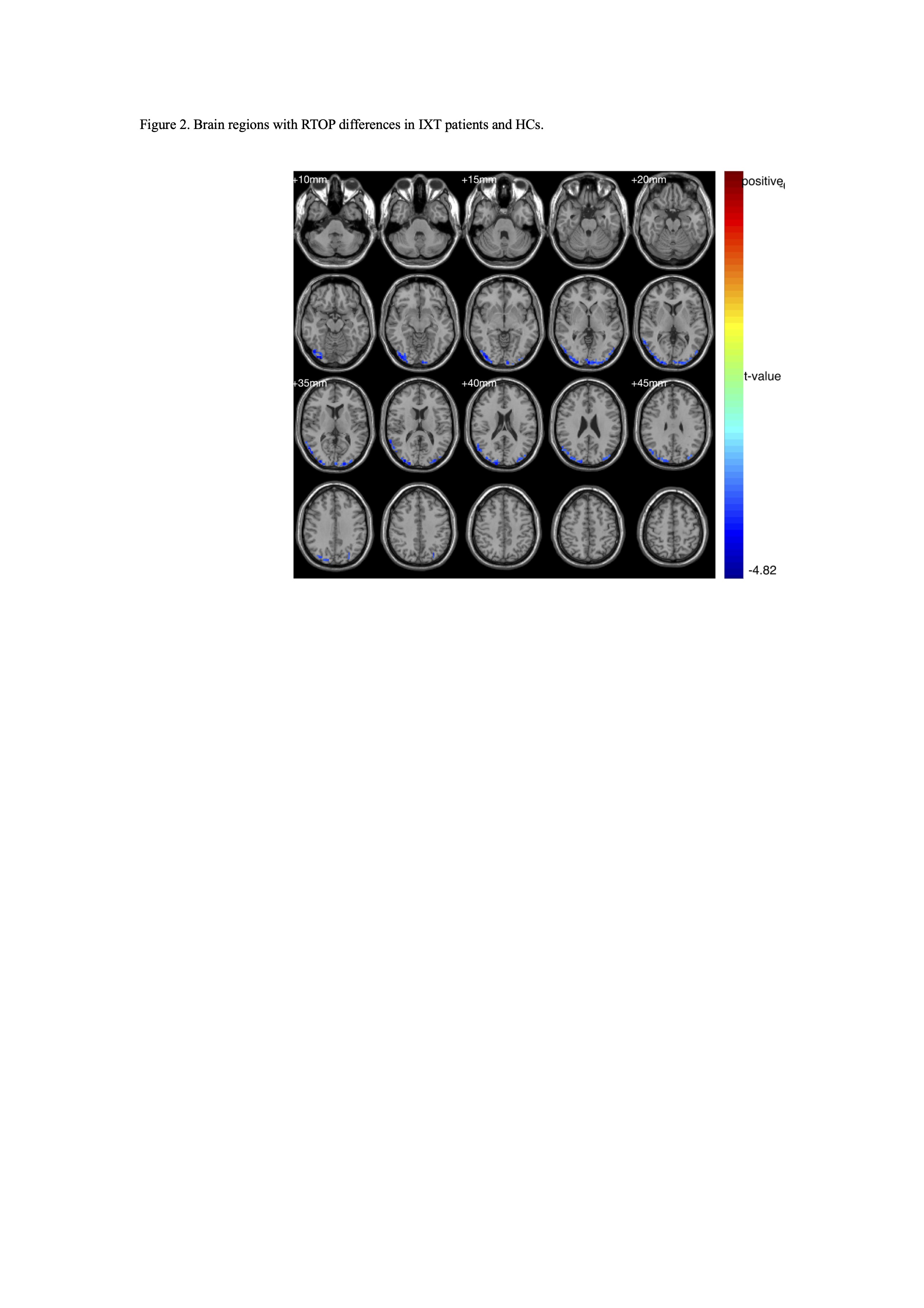
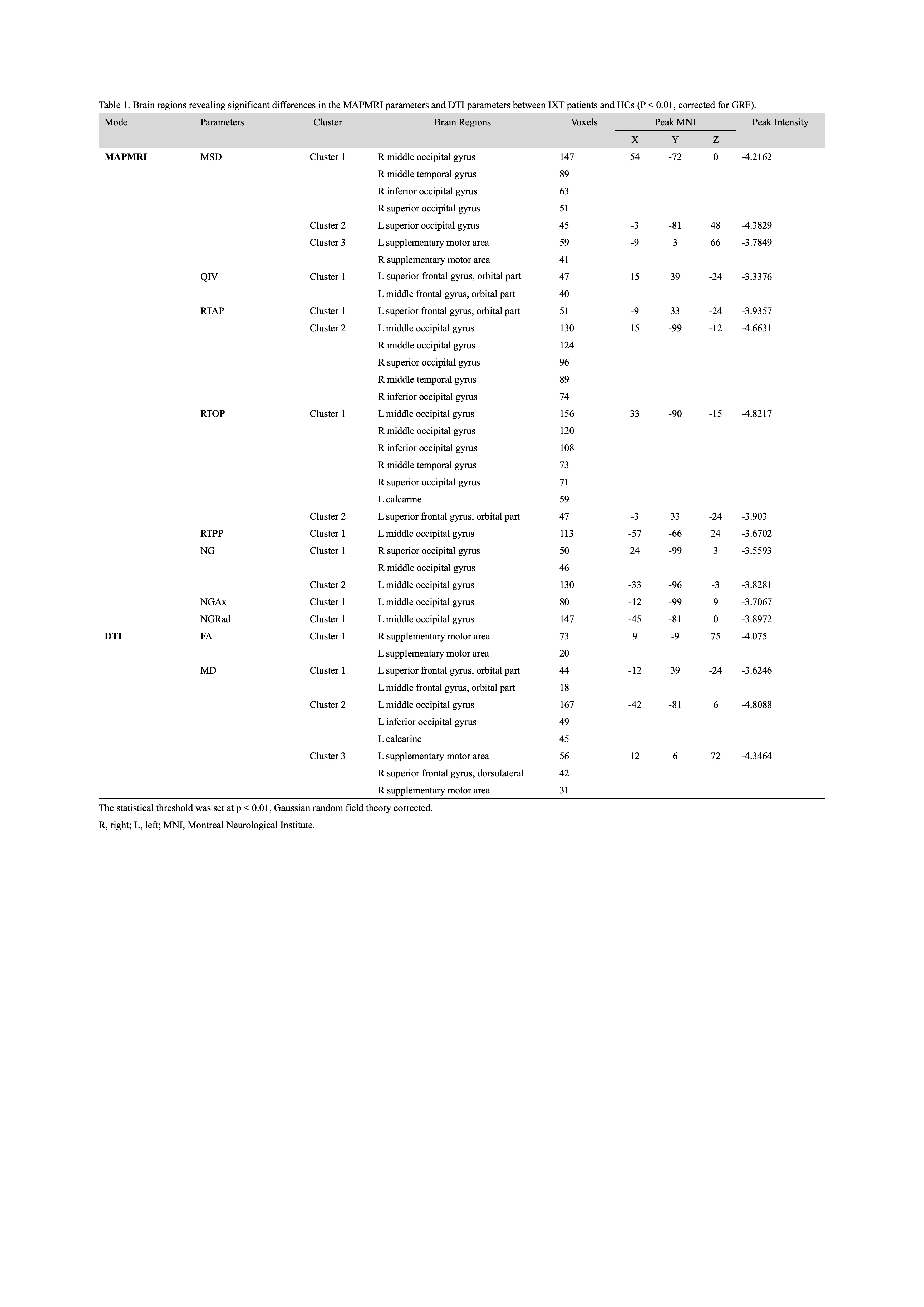
Table 1. Brain regions revealing significant differences in the MAPMRI parameters and DTI parameters between IXT patients and HCs (P < 0.01, corrected for GRF).
The statistical threshold was set at p < 0.01, Gaussian random field theory corrected.
R, right; L, left; MNI, Montreal Neurological Institute.
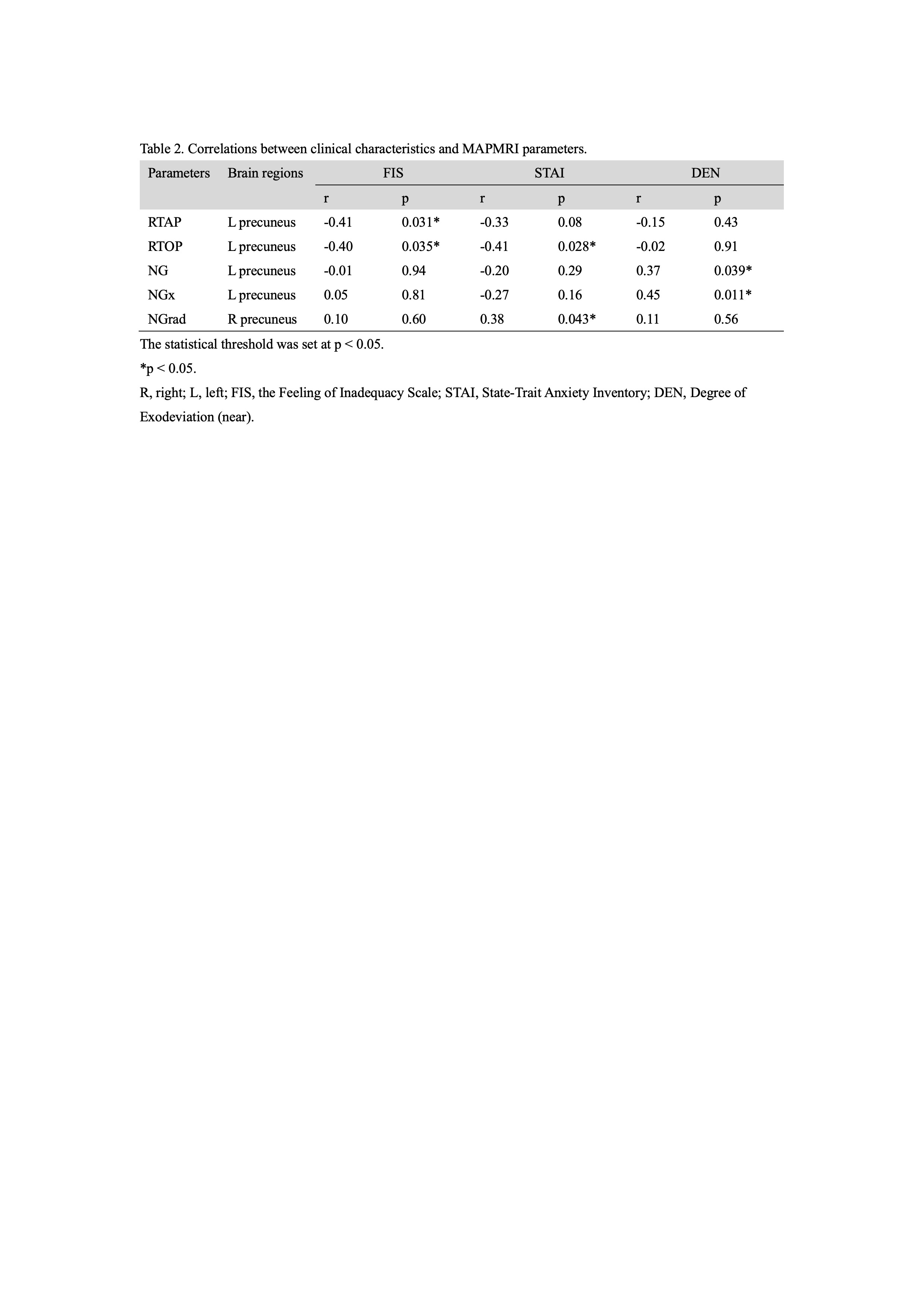
Table 2. Correlations between clinical characteristics and MAPMRI parameters.
The statistical threshold was set at p < 0.05.
*p < 0.05.
R, right; L, left; FIS, the Feeling of Inadequacy Scale; STAI, State-Trait Anxiety Inventory; DEN, Degree of Exodeviation (near).